
- Current
- Browse
- Collections
-
For contributors
- For Authors
- Instructions to authors
- Article processing charge
- e-submission
- For Reviewers
- Instructions for reviewers
- How to become a reviewer
- Best reviewers
- For Readers
- Readership
- Subscription
- Permission guidelines
- About
- Editorial policy
Articles
- Page Path
- HOME > Diabetes Metab J > Volume 41(5); 2017 > Article
-
Original ArticleClinical Diabetes & Therapeutics Effects of Lobeglitazone, a Novel Thiazolidinedione, on Bone Mineral Density in Patients with Type 2 Diabetes Mellitus over 52 Weeks
-
Soo Lim1, Kyoung Min Kim1, Sin Gon Kim2, Doo Man Kim3, Jeong-Taek Woo4, Choon Hee Chung5, Kyung Soo Ko6, Jeong Hyun Park7, Yongsoo Park8,9, Sang Jin Kim10, Hak Chul Jang1, Dong Seop Choi2

-
Diabetes & Metabolism Journal 2017;41(5):377-385.
DOI: https://doi.org/10.4093/dmj.2017.41.5.377
Published online: October 24, 2017
1Department of Internal Medicine, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea.
2Department of Internal Medicine, Korea University Anam Hospital, Korea University College of Medicine, Seoul, Korea.
3Department of Internal Medicine, Hallym University Kangdong Sacred Heart Hospital, Hallym University College of Medicine, Seoul, Korea.
4Department of Internal Medicine, Kyung Hee University Hospital, Kyung Hee University School of Medicine, Seoul, Korea.
5Department of Internal Medicine, Wonju Severance Christian Hospital, Yonsei University Wonju College of Medicine, Wonju, Korea.
6Department of Internal Medicine, Cardiovascular and Metabolic Disease Center, Inje University Sanggye Paik Hospital, Inje University College of Medicine, Seoul, Korea.
7Department of Internal Medicine, Inje University Busan Paik Hospital, Inje University College of Medicine, Busan, Korea.
8Kosair Children's Hospital Research Institute, University of Louisville, Louisville, KY, USA.
9Department of Internal Medicine, Hanyang University Guri Hospital, Hanyang University College of Medicine, Guri, Korea.
10Department of Internal Medicine, Soon Chun Hyang University Cheonan Hospital, Soon Chun Hyang University College of Medicine, Cheonan, Korea.
- Corresponding author: Dong Seop Choi. Department of Internal Medicine, Korea University Anam Hospital, Korea University College of Medicine, 73 Inchon-ro, Seongbuk-gu, Seoul 02841, Korea. cdongs@kumc.or.kr
- *Soo Lim and Kyoung Min Kim contributed equally to this study as first authors.
Copyright © 2017 Korean Diabetes Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Background
- The aim of this multicenter, randomized, double-blind study was to examine the effect of lobeglitazone, a novel thiazolidinedione, on the changes in bone mineral density (BMD) in patients with type 2 diabetes mellitus.
-
Methods
- A 24-week, double-blinded phase was followed by a 28-week, open-label phase, in which the placebo group also started to receive lobeglitazone. A total of 170 patients aged 34 to 76 years were randomly assigned in a 2:1 ratio to receive lobeglitazone 0.5 mg or a matching placebo orally, once daily. BMD was assessed using dual-energy X-ray absorptiometry at week 24 and at the end of the study (week 52).
-
Results
- During the double-blinded phase, the femur neck BMD showed decreasing patterns in both groups, without statistical significance (−0.85%±0.36% and −0.78%±0.46% in the lobeglitazone and placebo groups, respectively). The treatment difference between the groups was 0.07%, which was also not statistically significant. Further, minimal, nonsignificant decreases were observed in both groups in the total hip BMD compared to values at baseline, and these differences also did not significantly differ between the groups. During the open-label phase, the BMD was further decreased, but not significantly, by −0.32% at the femur neck and by −0.60% at the total hip in the lobeglitazone group, and these changes did not significantly differ compared with the original placebo group switched to lobeglitazone.
-
Conclusion
- Our results indicate that treatment with lobeglitazone 0.5 mg over 52 weeks showed no detrimental effect on the BMD compared to the placebo.
- The bone mineral density (BMD) tends to be increased in patients with type 2 diabetes mellitus (T2DM) because they are commonly overweight or obese [1]. However, the risk of osteoporotic fracture is significantly increased in patients with T2DM, with approximately a two-fold relative risk compared to those without diabetes [23]. The impaired bone quality and increased risk of falls might attenuate or offset the positive effect of the relatively large body weight on bone strength in subjects with T2DM [45]. Moreover, the mortality related to osteoporotic fracture is much higher in diabetic patients compared to their nondiabetic counterparts [2]. Given the deterioration of bone strength and higher mortality and morbidity in diabetic patients with fracture, the skeletal effects of antidiabetic drugs represent a major issue [6].
- Thiazolidinediones (TZDs) are a class of antidiabetic drugs that work by increasing insulin sensitivity by activating peroxisome proliferator-activated receptor γ (PPARγ) [78]. TZDs are known to inhibit differentiation of osteoblasts by overweighing adipogenesis from mesenchymal stem cells, which are the common progenitors of both adipocytes and osteoblasts [9]. Furthermore, some data suggest that TZDs may also partially promote osteoclastogenesis [10]. In many clinical trials, the BMD was found to decrease and the risk of fractures was found to increase in diabetic patients treated with rosiglitazone [1112]. Accordingly, there are many concerns about whether long-term administration of TZDs is associated with decreased BMD and increased osteoporotic fractures [1213]. These negative effects of TZDs on bone strength have become a major limitation in prescribing TZDs to diabetic patients, particularly those at high risk of fractures.
- Several TZDs have demonstrated similar glucose-lowering efficacies and are currently being used as antidiabetic drugs. However, these drugs have shown distinguishable properties in terms of their effects on diverse organs, systems, and processes, including energy metabolism, skeletal biology, the vasculature, and lipid profiles [1415]. Especially pioglitazone has been reported to show fewer negative effects on bone metabolism compared to rosiglitazone [1617]. Based on these findings, it is conceivable that the effects on bone metabolism might differ between different TZDs, independently of their glucose-lowering potency.
- Lobeglitazone is a novel PPARγ agonist with proven glucose-lowering potency in previous clinical trials and has been used to treat diabetic patients in several Asian countries [1819]. In the present study, we evaluated the effects of 52 weeks of treatment with lobeglitazone on BMD as a means to determine whether lobeglitazone treatment shows negative effects on BMD compared to a placebo.
INTRODUCTION
- Study design and patients
- This was a 52-week, multicenter, randomized, controlled trial to investigate the effect of lobeglitazone on BMD. This study consisted of two phases: a 24-week, double-blinded study followed by a 28-week open-label extension study in which the placebo group also started to receive lobeglitazone. This study was conducted at nine centers in South Korea between 2009 and 2011. In the first double-blinded phase, the patients were randomized into two groups in a 2:1 ratio: one group treated with lobeglitazone 0.5 mg and one group administered a placebo drug for 24 weeks. After completing the first phase of the study, a 28-week, open-label extension phase was conducted, with the patients receiving lobeglitazone continuing on the same drug, whereas the patients in the placebo group were switched to lobeglitazone and continued on this drug for 28 weeks. In our previous studies using the same cohort, the glucose-lowering efficacy and safety of lobeglitazone were demonstrated [1819]. In the present study, the main inclusion criteria were as follows: age 18 to 80 years; T2DM diagnosed at least 3 months prior to the study enrollment; glycosylated hemoglobin (HbA1c) 6.5% to 9.0% at the screening test if medication with oral hypoglycemic agents had been stopped less than 3 months ago, or HbA1c 7.0% to 10.0% at the screening test if patients were drug-naïve or had ceased medication with antidiabetic drugs more than 3 months previously; body mass index between 21 and 40 kg/m2; fasting serum C-peptide level >1.0 ng/mL. The exclusion criteria were as follows: fasting plasma glucose (FPG) level >250 mg/dL; triglyceride level >500 mg/dL; treatment with insulin or TZDs within 60 days; uncontrolled hypertension; history of cardiovascular diseases, including myocardial infarction, uncompensated heart failure, cerebral infarction, cerebral hemorrhage, or unstable angina within 6 months; severe hepatic or renal dysfunction; anemia for any reason; uncontrolled other disease or diabetic complications; and a history of cancer within 5 years. Subjects who used drugs affecting bone metabolism, including bisphosphonates, raloxifene, sex hormone-replacement therapy, or teriparatide, were also excluded. Subjects who were using lipid-lowering agents were allowed to maintain those drugs. This study was approved by each study center's Institutional Review Board (B-0704-044-009) and was carried out in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki). All patients provided informed consent to participate.
- The primary outcome was the changes in the femur neck BMD from baseline to the end of treatment. The secondary endpoints were the changes in total hip BMD during the study period and the percent of patients who showed changes of BMD more than −3.5% at the femur neck or total hip in each study phase.
- Dual-energy X-ray absorptiometry
- The BMDs at the femur neck and total hip area were measured by dual-energy X-ray absorptiometry (DXA) (Hologic Inc., Bedford, MA, USA; or GE Healthcare Lunar, Madison, WI, USA) in each center. DXA scans were performed at baseline and at week 24 and at the end of the study. BMD values from both systems were converted to standardized BMD values using a conversion formula, which is previously defined [20]. Changes in the BMD were calculated as the percentage of changes of the absolute BMD during the study period. The coefficient variations of BMD measurements in each center ranged from 0.8% to 1.8% for both the femur neck and total hip.
- Biochemical parameters
- After overnight fasting for at least 12 hours, serum was collected. The serum concentrations of total cholesterol, triglycerides, high density lipoprotein cholesterol, low density lipoprotein cholesterol, blood urea nitrogen, creatinine, HbA1c, and FPG were measured by standard biochemical methods.
- Statistical analysis
- Data are expressed as mean±standard deviation for continuous variables or as the number and the percentage of patients for categorical variables. The mean percent changes of BMD were calculated using the BMD values at baseline and at weeks 24 and 52. The comparisons of the changes from before and after the treatment within the groups were analyzed by the paired t-test, and differences between the study groups were assessed by repeated measures analysis of variance at the end of the study. Significant BMD loss was defined as a reduction of >3.5% in each study phase than 3.5% loss in each study phase, which was assumed as the least significant change calculated with precision multiplied by 2.77. All statistical analyses were performed using SPSS version 18 (SPSS Inc., Chicago, IL, USA). Values of P<0.05 were considered significant.
METHODS
- Demographics and baseline characteristics
- The detailed information about the subject enrollment and randomization has been previously described [1819]. A total of 173 patients were randomly assigned to the lobeglitazone or control group in a 2:1 ratio. The BMD values in three patients in the lobeglitazone group from the original study were not provided, and those patients were thus excluded from the present analysis. The baseline characteristics of the 170 patients who were finally included in the analyses are provided in Table 1. There were no differences in any of the demographic, anthropometric, or clinical characteristics at baseline between the two groups. Further, the BMD values were comparable between the groups for all patients and for men and women when analyzed separately (Table 2).
- Changes in bone mineral density
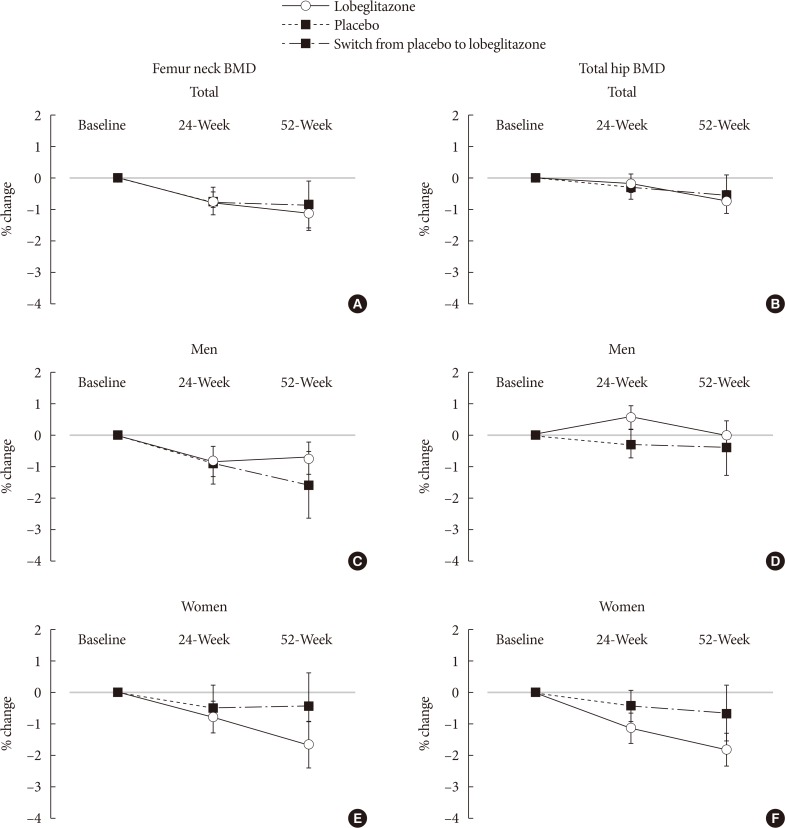
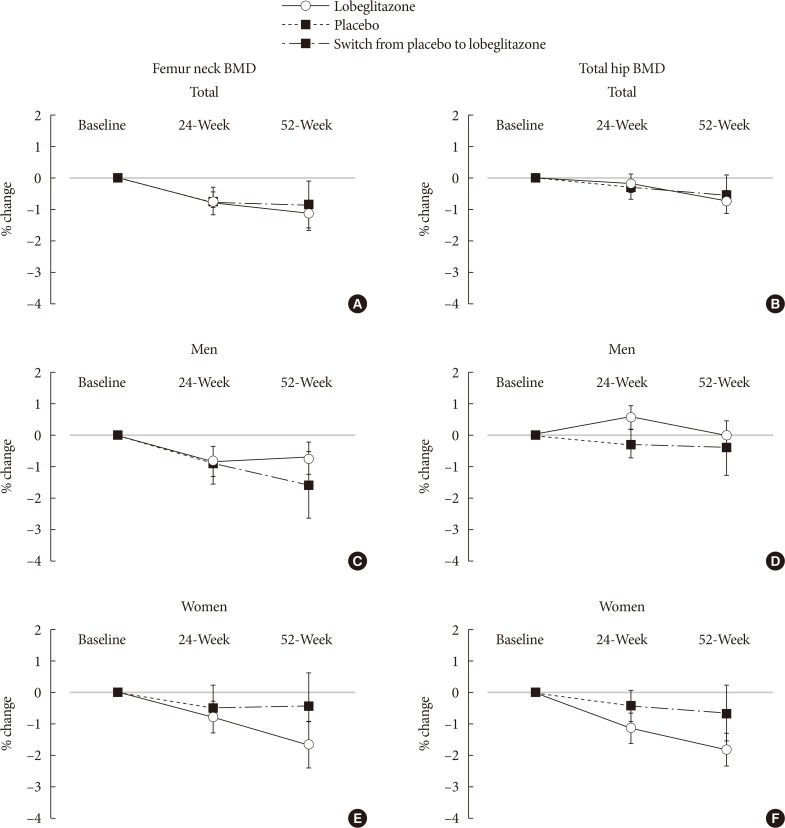
- Changes in BMD at the femur neck and total hip in the total subjects and in men and women are presented in Figs. 1 and 2. During the placebo, controlled, blinded phase, the femur neck BMD at 24 weeks had decreased by −0.85%±0.36% in the lobeglitazone group and by −0.78%±0.46% in the placebo group compared to values at baseline; however, these changes were not statistically significant. The difference between the groups was 0.07%, and this was also statistically insignificant (Figs. 1A and 2A). Minimal nonsignificant decreases were observed in both groups in total hip BMD, with no treatment difference noted between the groups (−0.17%±0.30% in the lobeglitazone group vs. −0.35%±0.34% in the placebo group; treatment difference, 0.17%; P>0.05 for all) (Figs. 1B and 2B). During the open-label phase, in which the placebo was switched to lobeglitazone, the BMD was further decreased by −0.32% in the femur neck and by −0.60% in the total hip, without statistical significances, in the lobeglitazone group (Figs. 1A, B and 2). In the group that switched to lobeglitazone during the open-label phase, there was a slight increase in the femur neck BMD and a decrease in the total hip BMD; however, these changes similarly did not reach statistical significance, and there were no significant differences compared to the lobeglitazone-maintained group (Figs. 1A, B and 2). Similar trends were observed in both men and women when analyzed separately (Fig. 1C and F).
- We also compared the BMD changes in women and men older than 50 years or younger. Consequently, the BMD changes were not different between the treatment groups regardless of their ages, indicating that lobeglitazone administration did not show any significant effects on BMD changes in subgroups that have higher risk of rapid bone loss (data not shown).
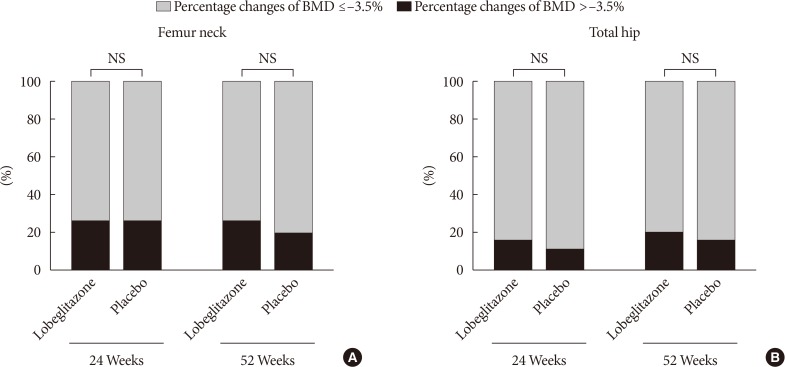
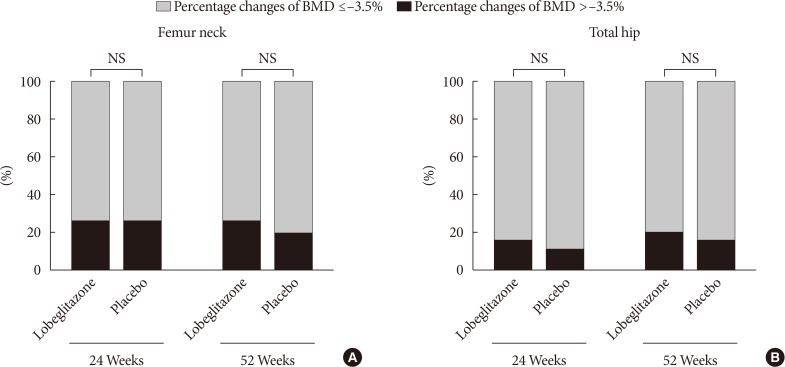
- The ratios of patients showing significant bone loss during the double-blinded or open-label phase did not differ between the groups at either the femur neck (25.5% in the lobeglitazone group vs. 25.2% in the placebo group during the double-blinded phase; 26.2% in the lobeglitazone group vs. 18.5% in the group switched from placebo to lobeglitazone during the open-label phase) or total hip (15.0% vs. 10.9% and 20.0% vs. 14.8%, respectively; P>0.05 for all) (Fig. 3).
RESULTS
- In this study, we investigated the effects of a novel TZD, lobeglitazone, on BMD in subjects with T2DM after 52 weeks of treatment. The results from the present study revealed neutral effects of lobeglitazone on BMD changes in this study population. No statistically significant differences were observed between the lobeglitazone and placebo groups in the changes in BMD at the femur neck and total hip compared to baseline during both the double-blinded and open-labeled periods.
- TZDs are insulin-sensitizing agents [2122] and are considered one of the major therapeutic drug classes for the management of diabetes [7]. TZDs increase insulin sensitivity by activating PPARγ, mainly in the adipose tissue and muscle, and show beneficial effects in preventing vascular complications in patients with insulin resistance [2324]. However, despite these benefits, severe clinical issues are related to TZDs, especially the predisposition to fractures [12]. Both adipocytes and osteoblasts differentiate from the same mesenchymal stem cells [2526], and TZDs are known to induce adipocyte differentiation [8] and suppress osteoblastogenesis [27]. Therefore, TZDs might have potentially negative effects on bone metabolism. Accordingly, rapid bone loss and increased risk of fractures have been reported in several clinical studies on TZDs [1128]. Thus, given the increased fragility of diabetes patients, the negative influence on bone has become a significant limitation in TZD prescription.
- Interestingly, rosiglitazone and pioglitazone show somewhat different profiles in their effects on diverse organs. Rosiglitazone, which was once withdrawn from the market because of an increased risk of cardiovascular events [29], has been reported to decrease BMD and increase fracture risks [11]. On the other hand, basic and clinical studies with pioglitazone revealed cardiovascular benefits [3031], although its effect on the skeletal system remains inconclusive, with several studies finding no meaningful influences on bone [1632]. In addition, these two drugs also exert distinct effects on lipid profiles and skeletal muscle biology [1415].
- Lobeglitazone, a novel PPARγ agonist, has proven glucose-lowering efficacy [181933] and a higher affinity with PPARγ compared to rosiglitazone or pioglitazone [3334]. This profile enables lower dosage as an antidiabetic therapeutic drug; thereby, decreasing the risks of dose-related side-effects. Moreover, the detrimental effects of rosiglitazone on bone are known to result partially from stimulated osteoclastogenesis [35]. However, this phenomenon has not been demonstrated with other TZDs [36]. In the present study, treatment with lobeglitazone 0.5 mg did not affect bone metabolism. The lower dosage of lobeglitazone and its differential effects on bone cells might contribute to the current study findings. However, mechanistic studies to elucidate its effects of bone biology are required to confirm this speculation.
- There are several strengths to this study. First, this was a multicenter, placebo-controlled, randomized clinical study. Second, BMD was measured in 98% of the participants. Third, diabetic patients taking other medications such as glucagon-like peptide-1 agonists or sodium-glucose cotransporter inhibitors were excluded because these agents might affect bone metabolism.
- However, several limitations should be noted. First, the primary outcome of the original study was changes in the HbA1c level. Therefore, the sample size was calculated based on the determination of the glucose-lowering efficacy, and not powered to investigate BMD changes. Second, approximately half of the study subjects were treatment-naïve patients whose bone quality is thus not expected to be greatly affected by long-term hyperglycemia. Therefore, we cannot extend the current study findings to diabetic populations with a long duration of disease. Third, bone formation and resorption markers were not assessed in the present study, which made it impossible to assess the effect of lobeglitazone on the bone turnover rate per se. Fourth, BMDs were measured only at the femur neck and total hip areas, not at the lumbar spine. Fifth, the study sample size was too small to evaluate the lobeglitazone effects on fracture risks, even though any new fractures had not happened during the study periods in both groups. Last, the study duration was only 52 weeks, which is not enough time to conclude the long-term cumulative effects of lobeglitazone on bone health.
- The prevalence of diabetes is increasing substantially worldwide, mainly due to increasing rates of obesity and insulin resistance [37383940], as well as in the increasing number of elderly people, in whom fracture is a critical factor affecting quality of life and mortality [2]. Under these circumstances, TZDs will continue to play a crucial role in diabetes management, and awareness of both the beneficial and side effects of these drugs is important in daily clinical practice [41]. In this study, treatment of lobeglitazone 0.5 mg once a day for 52 weeks showed no detrimental effect on BMD at the femur neck and total hip area compared to placebo. Longer-term and mechanistic studies are needed to confirm this finding.
DISCUSSION
-
Acknowledgements
- The original investigators were responsible for the study design and protocol. The current investigators were responsible for analysis plans, statistical analysis, and reporting of the results. The decision to submit the manuscript for publication was made jointly by all authors.
ACKNOWLEDGMENTS
-
CONFLICTS OF INTEREST: The original study was funded by CKD Pharmaceutical Corporation. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
NOTES
- 1. Strotmeyer ES, Cauley JA, Schwartz AV, Nevitt MC, Resnick HE, Zmuda JM, Bauer DC, Tylavsky FA, de Rekeneire N, Harris TB, Newman AB. Health ABC Study. Diabetes is associated independently of body composition with BMD and bone volume in older white and black men and women: The Health, Aging, and Body Composition Study. J Bone Miner Res 2004;19:1084-1091. ArticlePubMed
- 2. Liao CC, Lin CS, Shih CC, Yeh CC, Chang YC, Lee YW, Chen TL. Increased risk of fracture and postfracture adverse events in patients with diabetes: two nationwide population-based retrospective cohort studies. Diabetes Care 2014;37:2246-2252. ArticlePubMedPDF
- 3. Hofbauer LC, Brueck CC, Singh SK, Dobnig H. Osteoporosis in patients with diabetes mellitus. J Bone Miner Res 2007;22:1317-1328. ArticlePubMed
- 4. Starup-Linde J, Frost M, Vestergaard P, Abrahamsen B. Epidemiology of fractures in diabetes. Calcif Tissue Int 2017;100:109-121. ArticlePubMedPDF
- 5. Choi YJ, Chung YS. Type 2 diabetes mellitus and bone fragility: special focus on bone imaging. Osteoporos Sarcopenia 2016;2:20-24.ArticlePubMedPMC
- 6. Palermo A, D'Onofrio L, Eastell R, Schwartz AV, Pozzilli P, Napoli N. Oral anti-diabetic drugs and fracture risk, cut to the bone: safe or dangerous? A narrative review. Osteoporos Int 2015;26:2073-2089. ArticlePubMedPDF
- 7. Yki-Jarvinen H. Thiazolidinediones. N Engl J Med 2004;351:1106-1118. ArticlePubMed
- 8. Cariou B, Charbonnel B, Staels B. Thiazolidinediones and PPARγ agonists: time for a reassessment. Trends Endocrinol Metab 2012;23:205-215. ArticlePubMed
- 9. Rzonca SO, Suva LJ, Gaddy D, Montague DC, Lecka-Czernik B. Bone is a target for the antidiabetic compound rosiglitazone. Endocrinology 2004;145:401-406. ArticlePubMed
- 10. Wei W, Wang X, Yang M, Smith LC, Dechow PC, Sonoda J, Evans RM, Wan Y. PGC1beta mediates PPARgamma activation of osteoclastogenesis and rosiglitazone-induced bone loss. Cell Metab 2010;11:503-516. PubMedPMC
- 11. Bilezikian JP, Josse RG, Eastell R, Lewiecki EM, Miller CG, Wooddell M, Northcutt AR, Kravitz BG, Paul G, Cobitz AR, Nino AJ, Fitzpatrick LA. Rosiglitazone decreases bone mineral density and increases bone turnover in postmenopausal women with type 2 diabetes mellitus. J Clin Endocrinol Metab 2013;98:1519-1528. ArticlePubMed
- 12. Zhu ZN, Jiang YF, Ding T. Risk of fracture with thiazolidinediones: an updated meta-analysis of randomized clinical trials. Bone 2014;68:115-123. ArticlePubMed
- 13. Billington EO, Grey A, Bolland MJ. The effect of thiazolidinediones on bone mineral density and bone turnover: systematic review and meta-analysis. Diabetologia 2015;58:2238-2246. ArticlePubMedPDF
- 14. Goldberg RB, Kendall DM, Deeg MA, Buse JB, Zagar AJ, Pinaire JA, Tan MH, Khan MA, Perez AT, Jacober SJ. GLAI Study Investigators. A comparison of lipid and glycemic effects of pioglitazone and rosiglitazone in patients with type 2 diabetes and dyslipidemia. Diabetes Care 2005;28:1547-1554. ArticlePubMedPDF
- 15. Rabol R, Boushel R, Almdal T, Hansen CN, Ploug T, Haugaard SB, Prats C, Madsbad S, Dela F. Opposite effects of pioglitazone and rosiglitazone on mitochondrial respiration in skeletal muscle of patients with type 2 diabetes. Diabetes Obes Metab 2010;12:806-814. ArticlePubMed
- 16. Bone HG, Lindsay R, McClung MR, Perez AT, Raanan MG, Spanheimer RG. Effects of pioglitazone on bone in postmenopausal women with impaired fasting glucose or impaired glucose tolerance: a randomized, double-blind, placebo-controlled study. J Clin Endocrinol Metab 2013;98:4691-4701. ArticlePubMed
- 17. Li R, Xu W, Luo S, Xu H, Tong G, Zeng L, Zhu D, Weng J. Effect of exenatide, insulin and pioglitazone on bone metabolism in patients with newly diagnosed type 2 diabetes. Acta Diabetol 2015;52:1083-1091. ArticlePubMedPDF
- 18. Kim SG, Kim DM, Woo JT, Jang HC, Chung CH, Ko KS, Park JH, Park YS, Kim SJ, Choi DS. Efficacy and safety of lobeglitazone monotherapy in patients with type 2 diabetes mellitus over 24-weeks: a multicenter, randomized, double-blind, parallel-group, placebo controlled trial. PLoS One 2014;9:e92843. ArticlePubMedPMC
- 19. Kim SH, Kim SG, Kim DM, Woo JT, Jang HC, Chung CH, Ko KS, Park JH, Park YS, Kim SJ, Choi DS. Safety and efficacy of lobeglitazone monotherapy in patients with type 2 diabetes mellitus over 52 weeks: an open-label extension study. Diabetes Res Clin Pract 2015;110:e27-e30. ArticlePubMed
- 20. Fan B, Lu Y, Genant H, Fuerst T, Shepherd J. Does standardized BMD still remove differences between Hologic and GE-Lunar state-of-the-art DXA systems? Osteoporos Int 2010;21:1227-1236. ArticlePubMed
- 21. Kahn BB, McGraw TE. Rosiglitazone, PPARγ, and type 2 diabetes. N Engl J Med 2010;363:2667-2669. ArticlePubMedPMC
- 22. Home PD, Jones NP, Pocock SJ, Beck-Nielsen H, Gomis R, Hanefeld M, Komajda M, Curtis P. RECORD Study Group. Rosiglitazone RECORD study: glucose control outcomes at 18 months. Diabet Med 2007;24:626-634. ArticlePubMedPMC
- 23. Kernan WN, Viscoli CM, Furie KL, Young LH, Inzucchi SE, Gorman M, Guarino PD, Lovejoy AM, Peduzzi PN, Conwit R, Brass LM, Schwartz GG, Adams HP Jr, Berger L, Carolei A, Clark W, Coull B, Ford GA, Kleindorfer D, O'Leary JR, Parsons MW, Ringleb P, Sen S, Spence JD, Tanne D, Wang D, Winder TR. IRIS Trial Investigators. Pioglitazone after ischemic stroke or transient ischemic attack. N Engl J Med 2016;374:1321-1331. ArticlePubMedPMC
- 24. Liu J, Wang LN. Peroxisome proliferator-activated receptor gamma agonists for preventing recurrent stroke and other vascular events in patients with stroke or transient ischaemic attack. Cochrane Database Syst Rev 2015;(10):CD010693ArticlePubMed
- 25. Bianco P, Riminucci M, Gronthos S, Robey PG. Bone marrow stromal stem cells: nature, biology, and potential applications. Stem Cells 2001;19:180-192. ArticlePubMedPDF
- 26. Moerman EJ, Teng K, Lipschitz DA, Lecka-Czernik B. Aging activates adipogenic and suppresses osteogenic programs in mesenchymal marrow stroma/stem cells: the role of PPAR-gamma2 transcription factor and TGF-beta/BMP signaling pathways. Aging Cell 2004;3:379-389. ArticlePubMedPMC
- 27. Patel JJ, Butters OR, Arnett TR. PPAR agonists stimulate adipogenesis at the expense of osteoblast differentiation while inhibiting osteoclast formation and activity. Cell Biochem Funct 2014;32:368-377. ArticlePubMed
- 28. Aubert RE, Herrera V, Chen W, Haffner SM, Pendergrass M. Rosiglitazone and pioglitazone increase fracture risk in women and men with type 2 diabetes. Diabetes Obes Metab 2010;12:716-721. ArticlePubMed
- 29. Nissen SE, Wolski K. Effect of rosiglitazone on the risk of myocardial infarction and death from cardiovascular causes. N Engl J Med 2007;356:2457-2471. ArticlePubMed
- 30. Erdmann E, Dormandy JA, Charbonnel B, Massi-Benedetti M, Moules IK, Skene AM. PROactive Investigators. The effect of pioglitazone on recurrent myocardial infarction in 2,445 patients with type 2 diabetes and previous myocardial infarction: results from the PROactive (PROactive 05) Study. J Am Coll Cardiol 2007;49:1772-1780. PubMed
- 31. Osman I, Segar L. Pioglitazone, a PPARγ agonist, attenuates PDGF-induced vascular smooth muscle cell proliferation through AMPK-dependent and AMPK-independent inhibition of mTOR/p70S6K and ERK signaling. Biochem Pharmacol 2016;101:54-70. ArticlePubMed
- 32. Grey A, Bolland M, Fenwick S, Horne A, Gamble G, Drury PL, Reid IR. The skeletal effects of pioglitazone in type 2 diabetes or impaired glucose tolerance: a randomized controlled trial. Eur J Endocrinol 2013;170:255-262. ArticlePubMed
- 33. Lee HW, Kim BY, Ahn JB, Kang SK, Lee JH, Shin JS, Ahn SK, Lee SJ, Yoon SS. Molecular design, synthesis, and hypoglycemic and hypolipidemic activities of novel pyrimidine derivatives having thiazolidinedione. Eur J Med Chem 2005;40:862-874. ArticlePubMed
- 34. Kim BY, Ahn JB, Lee HW, Kang SK, Lee JH, Shin JS, Ahn SK, Hong CI, Yoon SS. Synthesis and biological activity of novel substituted pyridines and purines containing 2,4-thiazolidinedione. Eur J Med Chem 2004;39:433-447. ArticlePubMed
- 35. Wu H, Li L, Ma Y, Chen Y, Zhao J, Lu Y, Shen P. Regulation of selective PPARγ modulators in the differentiation of osteoclasts. J Cell Biochem 2013;114:1969-1977. ArticlePubMed
- 36. Okazaki R, Toriumi M, Fukumoto S, Miyamoto M, Fujita T, Tanaka K, Takeuchi Y. Thiazolidinediones inhibit osteoclastlike cell formation and bone resorption in vitro. Endocrinology 1999;140:5060-5065. ArticlePubMed
- 37. Weng J, Bi Y. Diabetes in China: the challenge now. J Diabetes Investig 2010;1:170-171.ArticlePubMedPMC
- 38. Song SO, Lee YH, Kim DW, Song YD, Nam JY, Park KH, Kim DJ, Park SW, Lee HC, Lee BW. Trends in diabetes incidence in the last decade based on Korean National Health Insurance Claims Data. Endocrinol Metab (Seoul) 2016;31:292-299. ArticlePubMedPMCPDF
- 39. Jeon JY, Ko SH, Kwon HS, Kim NH, Kim JH, Kim CS, Song KH, Won JC, Lim S, Choi SH, Jang MJ, Kim Y, Oh K, Kim DJ, Cha BY. Taskforce Team of Diabetes Fact Sheet of the Korean Diabetes Association. Prevalence of diabetes and prediabetes according to fasting plasma glucose and HbA1c. Diabetes Metab J 2013;37:349-357. ArticlePubMedPMC
- 40. Danaei G, Finucane MM, Lu Y, Singh GM, Cowan MJ, Paciorek CJ, Lin JK, Farzadfar F, Khang YH, Stevens GA, Rao M, Ali MK, Riley LM, Robinson CA, Ezzati M. Global Burden of Metabolic Risk Factors of Chronic Diseases Collaborating Group (Blood Glucose). National, regional, and global trends in fasting plasma glucose and diabetes prevalence since 1980: systematic analysis of health examination surveys and epidemiological studies with 370 country-years and 2·7 million participants. Lancet 2011;378:31-40. ArticlePubMed
- 41. Bae KH, Seo JB, Jung YA, Seo HY, Kang SH, Jeon HJ, Lee JM, Lee S, Kim JG, Lee IK, Jung GS, Park KG. Lobeglitazone, a novel peroxisome proliferator-activated receptor γ agonist, attenuates renal fibrosis caused by unilateral ureteral obstruction in mice. Endocrinol Metab (Seoul) 2017;32:115-123. ArticlePubMedPMCPDF
REFERENCES
Mean percentage of changes in bone mineral density (BMD) during the study period for the femur neck and total hip in (A, B) all subjects, (C, D) men, and (E, F) women.
Mean percentage changes in bone mineral density (BMD) for the (A) femur neck and (B) total hip during the double-blinded and open-labeled phases. NS, not significant.

Ratios of subjects who showed significant bone loss at the (A) femur neck and (B) total hip during the double-blinded and open-labeled phases. BMD, bone mineral density; NS, not significant.
Baseline characteristics of the study participants
Baseline bone mineral density in total, men, and women according to the treatment groups
Figure & Data
References
Citations
- Efficacy and safety of novel thiazolidinedione lobeglitazone for managing type-2 diabetes a meta-analysis
Deep Dutta, Saptarshi Bhattacharya, Manoj Kumar, Priyankar K. Datta, Ritin Mohindra, Meha Sharma
Diabetes & Metabolic Syndrome: Clinical Research & Reviews.2023; 17(1): 102697. CrossRef - Efficacy and safety of lobeglitazone, a new Thiazolidinedione, as compared to the standard of care in type 2 diabetes mellitus: A systematic review and meta-analysis
Shashank R. Joshi, Saibal Das, Suja Xaviar, Shambo Samrat Samajdar, Indranil Saha, Sougata Sarkar, Shatavisa Mukherjee, Santanu Kumar Tripathi, Jyotirmoy Pal, Nandini Chatterjee
Diabetes & Metabolic Syndrome: Clinical Research & Reviews.2023; 17(1): 102703. CrossRef - The benefits of adipocyte metabolism in bone health and regeneration
Lisa-Marie Burkhardt, Christian H. Bucher, Julia Löffler, Charlotte Rinne, Georg N. Duda, Sven Geissler, Tim J. Schulz, Katharina Schmidt-Bleek
Frontiers in Cell and Developmental Biology.2023;[Epub] CrossRef - Will lobeglitazone rival pioglitazone? A systematic review and critical appraisal
Kalyan Kumar Gangopadhyay, Awadhesh Kumar Singh
Diabetes & Metabolic Syndrome: Clinical Research & Reviews.2023; 17(4): 102747. CrossRef - Comparison of therapeutic efficacy and safety of sitagliptin, dapagliflozin, or lobeglitazone adjunct therapy in patients with type 2 diabetes mellitus inadequately controlled on sulfonylurea and metformin: Third agent study
Jun Hwa Hong, Jun Sung Moon, Kayeon Seong, Soo Lim
Diabetes Research and Clinical Practice.2023; 203: 110872. CrossRef - Bone Mineral Density Evaluation Among Type 2 Diabetic Patients in Rural Haryana, India: An Analytical Cross-Sectional Study
Nitish Khandelwal, Surbhi Rajauria, Siddhesh Pandurang Kanjalkar, Omkar Shivaji Chavanke, Sanjay Rai
Cureus.2023;[Epub] CrossRef - Lobeglitazone and Its Therapeutic Benefits: A Review
Balamurugan M, Sarumathy S, Robinson R
Cureus.2023;[Epub] CrossRef - A double‐blind, Randomized controlled trial on glucose‐lowering EFfects and safety of adding 0.25 or 0.5 mg lobeglitazone in type 2 diabetes patients with INadequate control on metformin and dipeptidyl peptidase‐4 inhibitor therapy: REFIND study
Soree Ryang, Sang Soo Kim, Ji Cheol Bae, Ji Min Han, Su Kyoung Kwon, Young Il Kim, Il Seong Nam‐Goong, Eun Sook Kim, Mi‐kyung Kim, Chang Won Lee, Soyeon Yoo, Gwanpyo Koh, Min Jeong Kwon, Jeong Hyun Park, In Joo Kim
Diabetes, Obesity and Metabolism.2022; 24(9): 1800. CrossRef - A Real-World Study of Long-Term Safety and Efficacy of Lobeglitazone in Korean Patients with Type 2 Diabetes Mellitus
Bo-Yeon Kim, Hyuk-Sang Kwon, Suk Kyeong Kim, Jung-Hyun Noh, Cheol-Young Park, Hyeong-Kyu Park, Kee-Ho Song, Jong Chul Won, Jae Myung Yu, Mi Young Lee, Jae Hyuk Lee, Soo Lim, Sung Wan Chun, In-Kyung Jeong, Choon Hee Chung, Seung Jin Han, Hee-Seok Kim, Ju-Y
Diabetes & Metabolism Journal.2022; 46(6): 855. CrossRef - Comparative Efficacy of Lobeglitazone Versus Pioglitazone on Albuminuria in Patients with Type 2 Diabetes Mellitus
Kyung-Soo Kim, Sangmo Hong, Hong-Yup Ahn, Cheol-Young Park
Diabetes Therapy.2021; 12(1): 171. CrossRef - Lobeglitazone: A Novel Thiazolidinedione for the Management of Type 2 Diabetes Mellitus
Jaehyun Bae, Taegyun Park, Hyeyoung Kim, Minyoung Lee, Bong-Soo Cha
Diabetes & Metabolism Journal.2021; 45(3): 326. CrossRef - Effect of lobeglitazone on motor function in rat model of Parkinson’s disease with diabetes co-morbidity
Kambiz Hassanzadeh, Arman Rahimmi, Mohammad Raman Moloudi, Rita Maccarone, Massimo Corbo, Esmael Izadpanah, Marco Feligioni
Brain Research Bulletin.2021; 173: 184. CrossRef - Recent Perspective on Thiazolidinedione
Won Jun Kim
The Journal of Korean Diabetes.2021; 22(2): 97. CrossRef - Use of in vitro bone models to screen for altered bone metabolism, osteopathies, and fracture healing: challenges of complex models
Sabrina Ehnert, Helen Rinderknecht, Romina H. Aspera-Werz, Victor Häussling, Andreas K. Nussler
Archives of Toxicology.2020; 94(12): 3937. CrossRef - Update on: effects of anti-diabetic drugs on bone metabolism
Guillaume Mabilleau, Béatrice Bouvard
Expert Review of Endocrinology & Metabolism.2020; 15(6): 415. CrossRef - The use of metformin, insulin, sulphonylureas, and thiazolidinediones and the risk of fracture: Systematic review and meta‐analysis of observational studies
Khemayanto Hidayat, Xuan Du, Meng‐Jiao Wu, Bi‐Min Shi
Obesity Reviews.2019; 20(10): 1494. CrossRef - Diabetes pharmacotherapy and effects on the musculoskeletal system
Evangelia Kalaitzoglou, John L. Fowlkes, Iuliana Popescu, Kathryn M. Thrailkill
Diabetes/Metabolism Research and Reviews.2019;[Epub] CrossRef - Morin Exerts Anti‐Arthritic Effects by Attenuating Synovial Angiogenesis via Activation of Peroxisome Proliferator Activated Receptor‐γ
Mengfan Yue, Ni Zeng, Yufeng Xia, Zhifeng Wei, Yue Dai
Molecular Nutrition & Food Research.2018;[Epub] CrossRef - The effects of diabetes therapy on bone: A clinical perspective
Karim G. Kheniser, Carmen M. Polanco Santos, Sangeeta R. Kashyap
Journal of Diabetes and its Complications.2018; 32(7): 713. CrossRef - Changes in the Bone Mineral Density of Femur Neck and Total Hip Over a 52-Week Treatment with Lobeglitazone
Da Young Lee, Ji A Seo
Diabetes & Metabolism Journal.2017; 41(5): 374. CrossRef
 PubReader
PubReader Cite
Cite- Figure
-

- Related articles
-
- The Beneficial Effect of Glycemic Control against Adverse Outcomes in Patients with Type 2 Diabetes Mellitus and Chronic Kidney Disease
- Clinical Effects of a Home Care Pilot Program for Patients with Type 1 Diabetes Mellitus: A Retrospective Cohort Study
- Safety of COVID-19 Vaccines among Patients with Type 2 Diabetes Mellitus: Real-World Data Analysis
- Efficacy and Safety of Enavogliflozin versus Dapagliflozin as Add-on to Metformin in Patients with Type 2 Diabetes Mellitus: A 24-Week, Double-Blind, Randomized Trial
- Effectiveness of Resistance Exercise on Inflammatory Biomarkers in Patients with Type 2 Diabetes Mellitus: A Systematic Review with Meta-Analysis



