
- Current
- Browse
- Collections
-
For contributors
- For Authors
- Instructions to authors
- Article processing charge
- e-submission
- For Reviewers
- Instructions for reviewers
- How to become a reviewer
- Best reviewers
- For Readers
- Readership
- Subscription
- Permission guidelines
- About
- Editorial policy
Articles
- Page Path
- HOME > Diabetes Metab J > Volume 47(1); 2023 > Article
-
Original ArticleLifestyle Effectiveness of Resistance Exercise on Inflammatory Biomarkers in Patients with Type 2 Diabetes Mellitus: A Systematic Review with Meta-Analysis
-
Rubén Fernández-Rodríguez1
 , Sonia Monedero-Carrasco1, Bruno Bizzozero-Peroni1,2, Miriam Garrido-Miguel1,3, Arthur Eumann Mesas1,4, Vicente Martínez-Vizcaíno1,5
, Sonia Monedero-Carrasco1, Bruno Bizzozero-Peroni1,2, Miriam Garrido-Miguel1,3, Arthur Eumann Mesas1,4, Vicente Martínez-Vizcaíno1,5 -
Diabetes & Metabolism Journal 2023;47(1):118-134.
DOI: https://doi.org/10.4093/dmj.2022.0007
Published online: April 29, 2022
1University of Castilla-La Mancha, Health and Social Research Center, Cuenca, Spain
2University of the Republic, Higher Institute of Physical Education, Rivera, Uruguay
3University of Castilla-La Mancha, Faculty of Nursing, Albacete, Spain
4State University of Londrina, Health Science Center, Londrina, Brazil
5University Autonomous of Chile, Faculty of Health Sciences, Talca, Chile
-
Corresponding author: Arthur Eumann Mesas Universidad de Castilla La-Mancha, Health and Social Research Center, Santa Teresa Jornet s/n, 16071 Cuenca, Spain E-mail: Arthur.EMesas@uclm.es
Copyright © 2023 Korean Diabetes Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Background
- Type 2 diabetes mellitus (T2DM) is related to increased inflammatory processes. The effects of resistance exercise on inflammatory biomarkers in T2DM are controversial. Our purpose was to determine the effectiveness of resistance exercise on inflammatory biomarkers in patients diagnosed with T2DM.
-
Methods
- We searched four databases until September 2021. We included randomized clinical trials (RCTs) of the effects of resistance exercise on inflammatory biomarkers (C-reactive protein [CRP], tumor necrosis factor alpha, interleukin-6, and interleukin-10) in patients with T2DM. A random effects meta-analysis was conducted to determine the standardized mean difference (SMD) and the raw mean difference (MD) for CRP.
-
Results
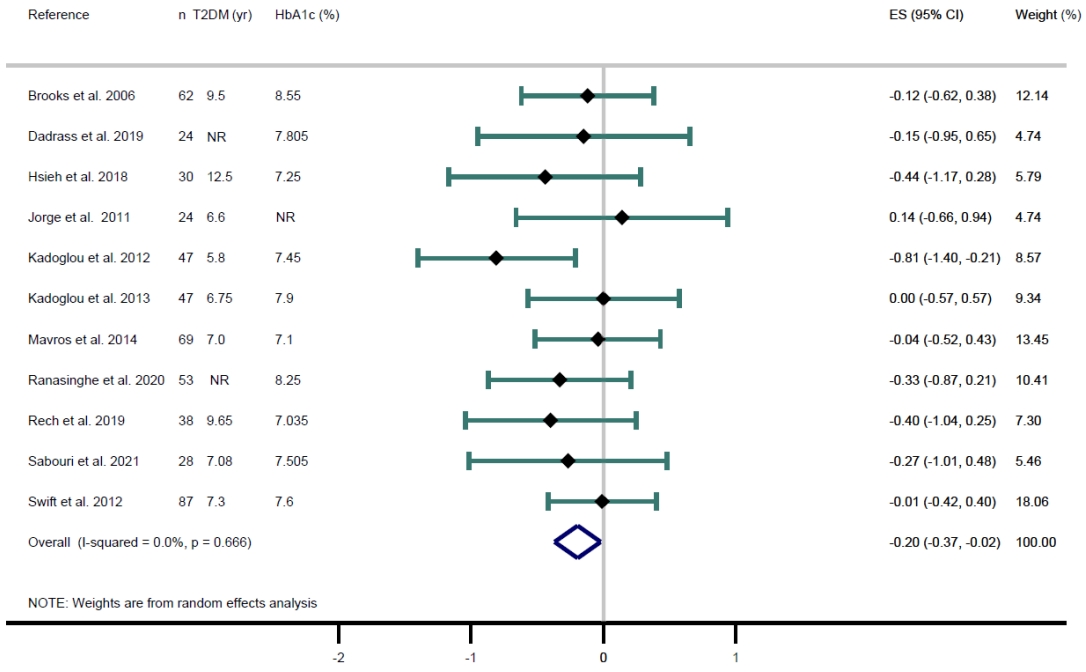
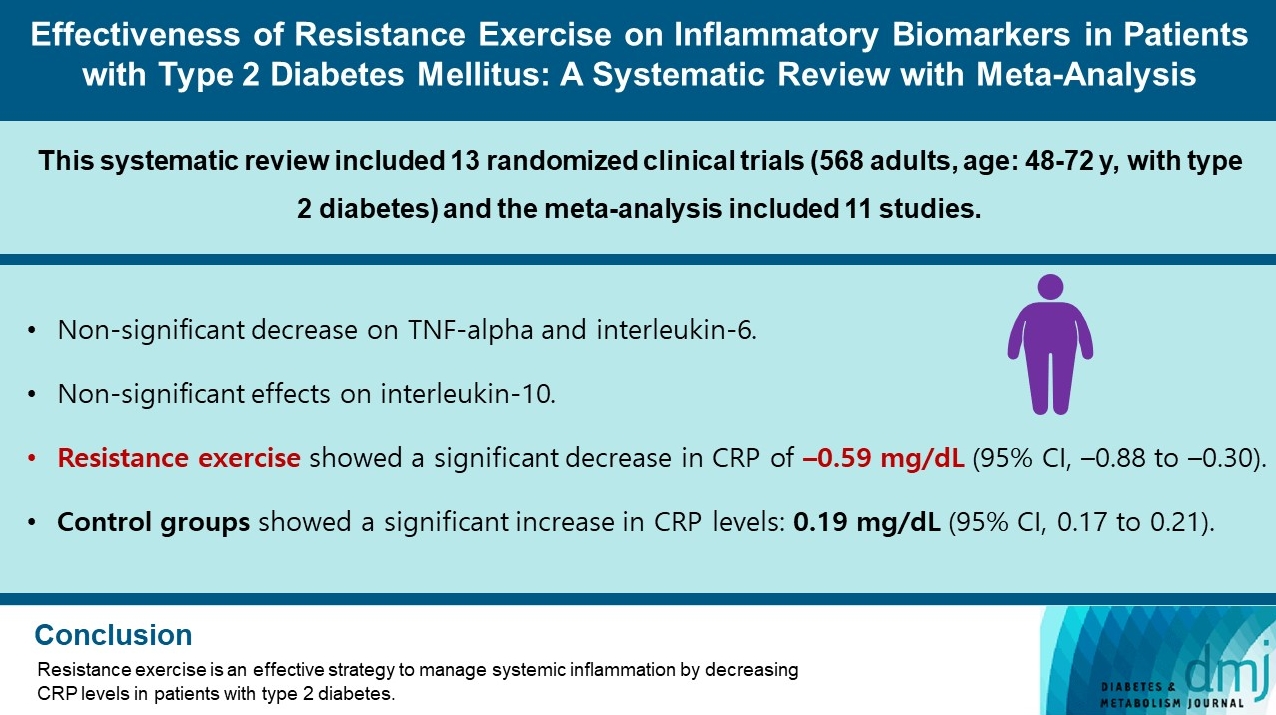
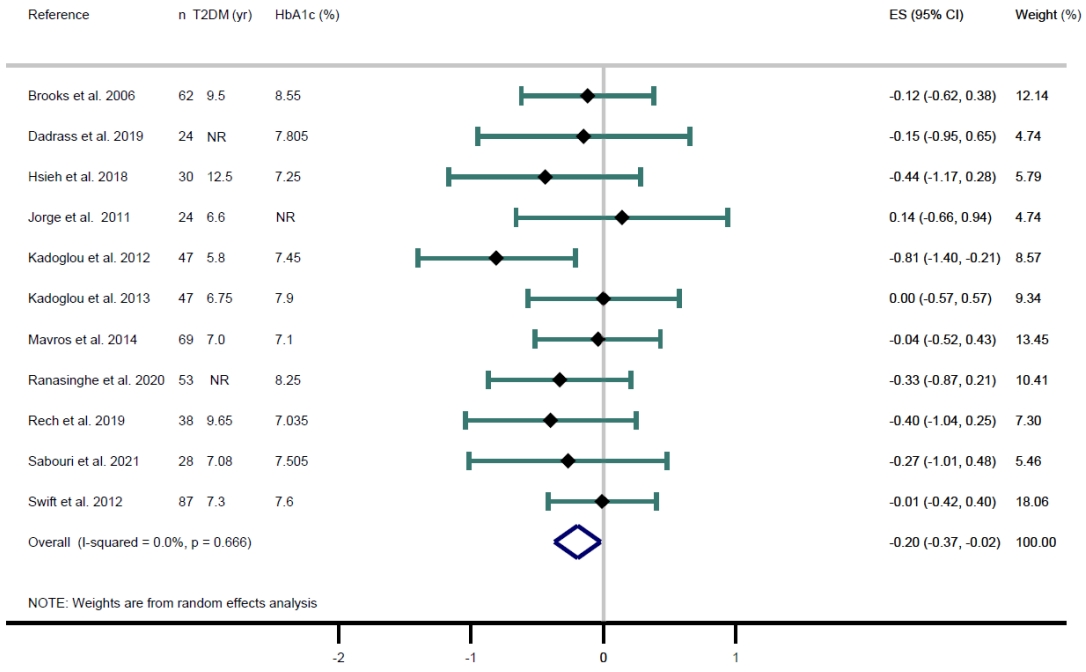
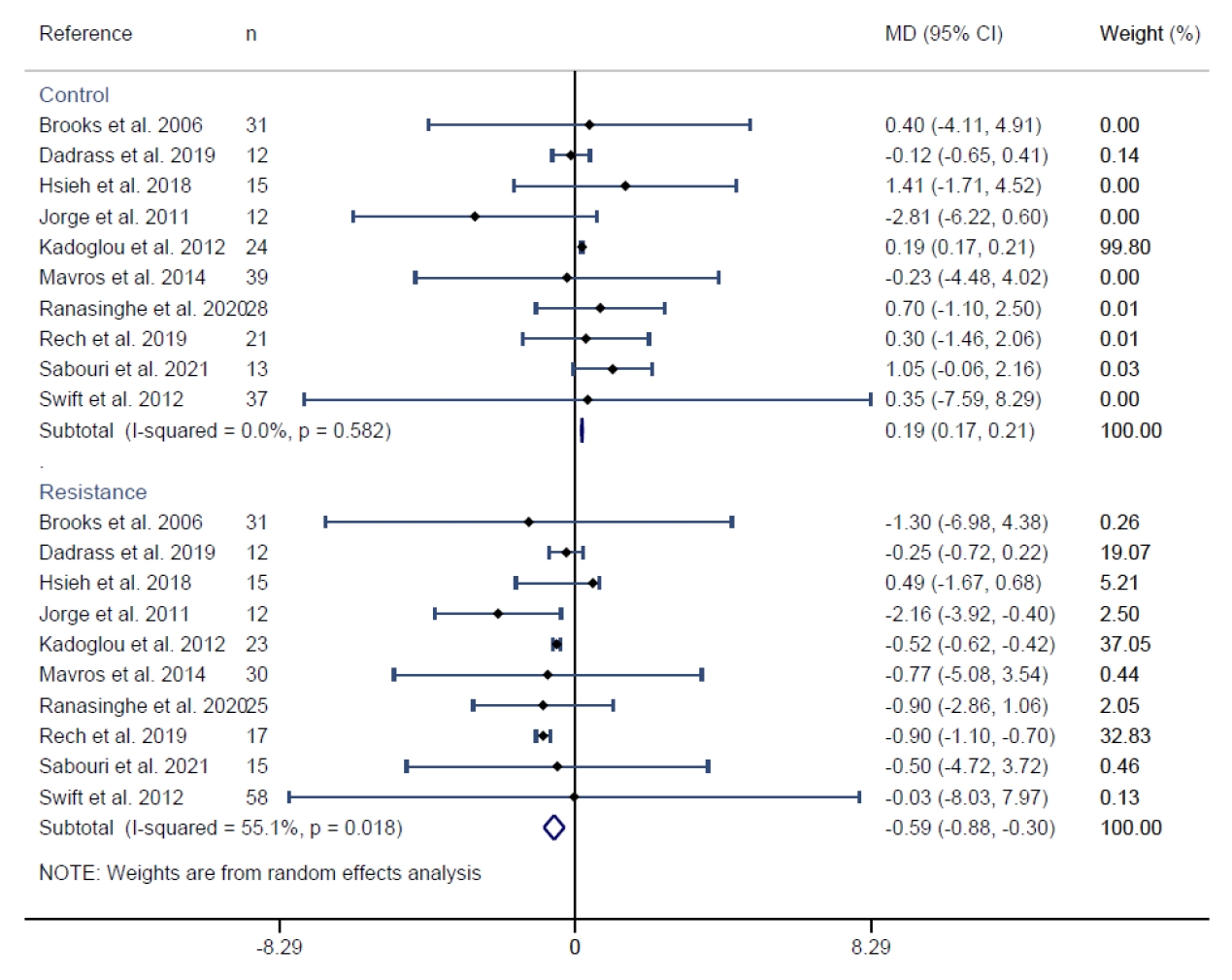
- Thirteen RCTs were included in the review, and 11 in the meta-analysis for CRP. Lower CRP levels were observed when resistance exercise was compared with the control groups (SMD=–0.20; 95% confidence interval [CI], –0.37 to –0.02). When conducting the MD meta-analysis, resistance exercise showed a significant decrease in CRP of –0.59 mg/dL (95% CI, –0.88 to –0.30); otherwise, in the control groups, the CRP values increased 0.19 mg/dL (95% CI, 0.17 to 0.21).
-
Conclusion
- Evidence supports resistance exercise as an effective strategy to manage systemic inflammation by decreasing CRP levels in patients with T2DM. The evidence is still inconclusive for other inflammatory biomarkers.
- In recent years, type 2 diabetes mellitus (T2DM) has been increasing exponentially [1], ranking among the 10 leading causes of death in adults, having a worldwide prevalence of over 9% and affecting approximately 463 million people [1]. Consequently, developing preventive measures to delay the onset and early treatment strategies to slow the progression of T2DM is a major concern among clinical health professionals and public health researchers [2].
- T2DM is caused by chronic inadequate insulin production by pancreatic β-cells, leading to hyperglycemia [3]. This causes an immune response that results in a chronic low-grade inflammatory status [3], which includes increased levels of inflammatory biomarkers such as C-reactive protein (CRP), tumor necrosis factor alpha (TNF-α), or interleukin-6 (IL-6) [4]. Low-grade chronic inflammation has great implications for the onset and progression of T2DM [5]. For instance, these biomarkers affect insulin production by progressive damage to pancreatic β-cells and inflammation [3], along with other factors (e.g., aging, physical inactivity, obesity, etc.) can be involved in the development of insulin resistance [3] and, therefore, promote the inefficient use of insulin by the body’s cells. Thus, both mechanisms contribute to chronic hyperglycemia [3]. Additionally, it is well established that patients with T2DM generally have higher adiposity levels [6], particularly visceral adiposity, which is also associated with chronic inflammation and insulin resistance [7].
- In this context, exercise could be a nonpharmacological intervention that may delay the progression of the disease and improve the management and quality of life of people with T2DM [2]. Accordingly, it has been suggested that exercise could delay the progression of insulin resistance [8] because of its effect on reducing circulating levels of inflammatory biomarkers such as CRP, TNF-α, and IL-6 [9,10]. In this sense, resistance exercise has gained importance for patients with T2DM [11] due to its multisystemic and specific musculoskeletal benefits [12]. Additionally, resistance exercise may be a useful exercise strategy in patients with a diagnosis of T2DM due to their exposure to accelerated muscle loss [13], which would be related to an increased risk of mortality and other comorbidities [14].
- There is increasing evidence of resistance exercise in different populations, and recently, international guidelines, including the American Diabetes Association Standards of Medical Care in Diabetes (2022) recommend resistance exercise of any intensity to improve glycemic control as well as strength, balance, and activities of daily living in patients with T2DM [15]. Despite this, although some studies have shown benefits on several health parameters, including inflammatory biomarkers [11,16], other studies have questioned its effectiveness [9]. Therefore, our purpose was to synthesize the current evidence and determine the effectiveness of resistance exercise on inflammatory biomarkers in patients with T2DM.
INTRODUCTION
- Ethical statement
- This systematic review and meta-analysis were conducted by collecting data from primary studies in which informed consent had been obtained by the respective original authors; thus, our review was exempt from ethics approval.
- Search strategy and study selection
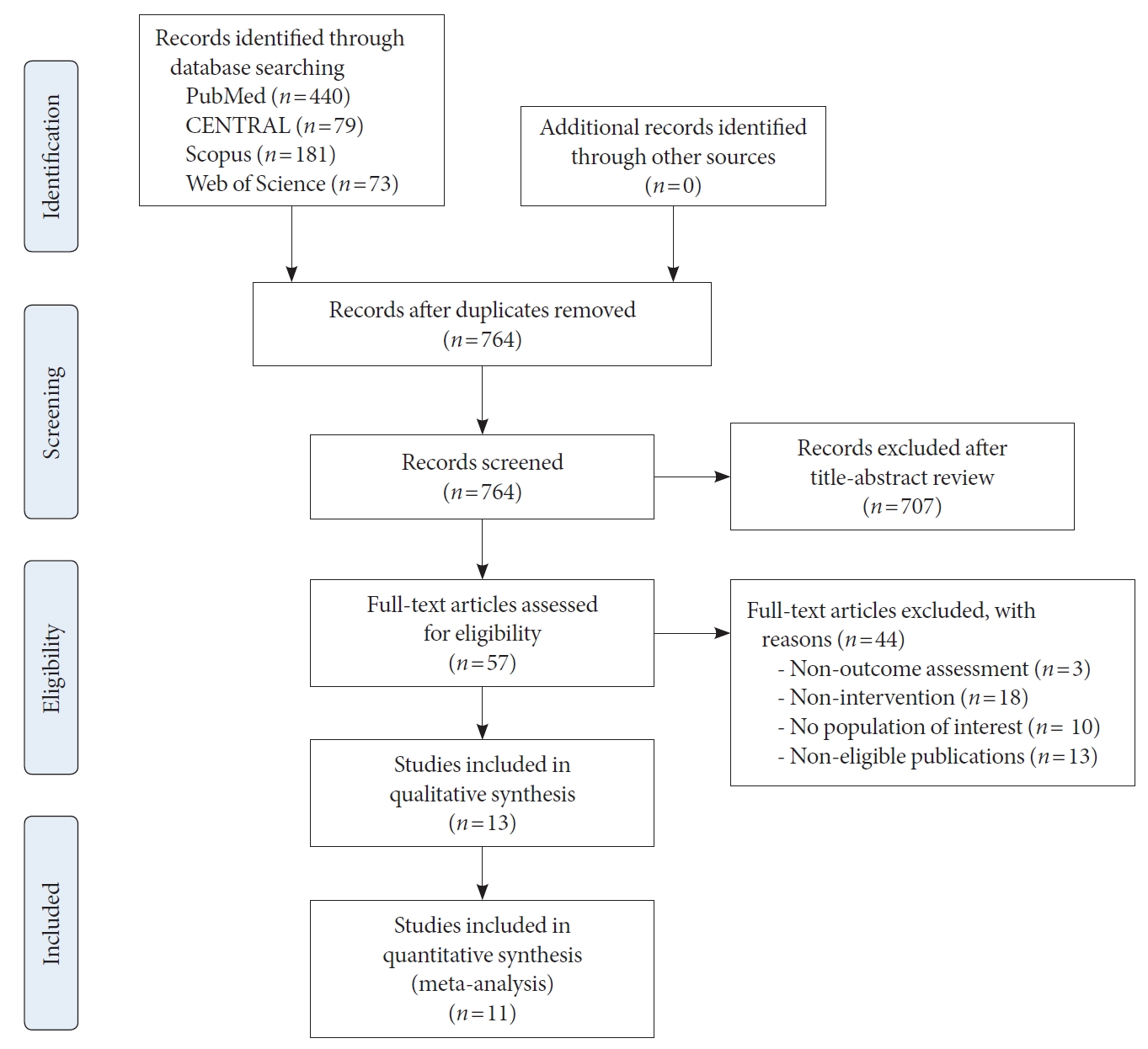
- The present systematic review and meta-analysis were conducted according to the recommendations of the Cochrane Handbook for Systematic Reviews of Interventions [17] and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (Appendix 1) [18]. We registered this review in the PROSPERO database (registration number: CRD42021261-762).
- A systematic search was conducted in the MEDLINE (via PubMed), Scopus, Cochrane CENTRAL, and Web of Science databases from inception until September 2021 to identify randomized controlled trials (RCTs) aimed at determining the effectiveness of resistance exercise on inflammatory biomarkers in adults diagnosed with T2DM. The search strategy combined the following medical subject headings with free terms and matching synonyms: ‘type 2 diabetes,’ ‘noninsulin-dependent diabetes mellitus,’ ‘resistance training,’ ‘resistance exercise,’ ‘strength training,’ ‘strength exercise,’ ‘strengthening,’ ‘inflammation,’ ‘inflammatory markers,’ ‘inflammatory cytokines,’ ‘inflammatory biomarkers,’ ‘c reactive protein,’ ‘tumor necrosis factor alpha,’ and ‘interleukin 6.’ The complete search strategy for each database is available in the Supplementary Table 1.
- Eligibility criteria
- The titles and abstracts of the retrieved articles were examined by two independent reviewers (R.F.R., S.M.C.) to identify suitable studies. Articles related to this systematic review were selected for full text screening and evaluated according to the eligibility criteria. The inclusion criteria were as follows: (1) type of participants: adults (≥18 years) with a medical diagnosis of T2DM; (2) type of intervention: at least one arm trial had to be related to resistance exercise; (3) control condition with nonexercise intervention (i.e., usual care, advice); (4) outcome: inflammatory biomarkers such as CRP, TNF-α, IL-6, or IL-10; (5) type of studies: RCTs. Moreover, the studies were excluded when (1) some participants were non-clinically diagnosed with T2DM and (2) resistance exercise was not the only type of exercise performed (i.e., multimodality, concurrent training). A third reviewer (A.E.M.) was consulted to resolve disagreements between reviewers. No language restrictions were applied. Excluded studies with the reason for exclusion are available in Supplementary Table 2.
- Data extraction and risk of bias assessment
- Two independent reviewers (R.F.R., S.M.C.) extracted the following information from the included studies: first author’s name and year of publication; country; study design; characteristics of the study population (mean age, women’s percentage, baseline body mass index [BMI], comorbidities), total sample size and sample size by group, intervention characteristics (exercise protocol), medication, comparison characteristics, outcome measures and main results. A third reviewer (A.E.M.) was consulted to resolve disagreements between reviewers.
- Two reviewers (R.F.R., S.M.C.) independently assessed the risk of bias of the included studies using the Cochrane risk-of-bias tool for randomized trials [19]. The following six domains were assessed: randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result. As it would be impossible to truly blind patients to treatment allocation in exercise trials, this specific item of the risk of bias was not included to generate the overall risk of bias assessment. In this sense, each domain was assessed as ‘low risk of bias,’ ‘some concerns,’ or ‘high risk of bias,’ and the overall risk of bias for each study was classified as (1) ‘low risk of bias’ when a low risk of bias was determined for all domains; (2) ‘some concerns’ when at least one domain was assessed as raising some concerns, but no single domain was assessed as high risk of bias; or (3) ‘high risk of bias’ when high risk of bias was reached for at least one domain or some concerns in multiple domains.
- Disagreements between initial reviewers were solved by a third coauthor (A.E.M.).
- Quality of evidence
- The “Grades of Recommendations, Assessment, Development, and Evaluation” (GRADE) tool was used to evaluate and summarize the quality of the evidence [20]. Based on the design of the studies, the inflammatory biomarker outcome measure was rated as high-, moderate-, low-or very low-quality evidence considering the following domains: (1) risk of bias (–1 when <75% of the analyzed studies were at low risk of bias); (2) inconsistency (–1 when I2 >50%); (3) indirect evidence (from population, intervention, control or outcomes); (4) imprecision displayed in wide confidence intervals (CIs); and (5) publication bias, which downgraded the quality of evidence risk of bias. The GRADE tool was used for those outcomes with enough data for the meta-analysis.
- Data analysis
- When at least five studies reported valid data for the outcome, we extracted the primary data from each study, including pre-post mean inflammatory biomarker values, standard deviations and sample sizes of intervention and control groups (CG). Therefore, meta-analyses were conducted for CRP (11 studies), TNF-α (six studies), and IL-6 (five studies) but not for IL-10 (two studies) as the statistical analysis would not be able to translate the potential effect of resistance exercise. The standardized mean difference (SMD) with its 95% CI was calculated for each study using the DerSimonian and Laird random-effects method [21]. Then, the pooled SMDs were estimated for the effect of resistance exercise versus the CG. Furthermore, to show the clinical change in outcome units of measurement (mg/dL), we computed the pooled raw mean difference (MD) after transforming all outcome data into the same unit. Additionally, the heterogeneity was evaluated with the I2 statistic as follows: I2 values of 0%–40% were considered to be ‘not important’ heterogeneity, 30%–60% indicated ‘moderate’ heterogeneity, 50%–90% indicated ‘substantial’ heterogeneity, and 75%–100% indicated ‘considerable’ heterogeneity, taking into account the corresponding P values and 95% CIs [22].
- We conducted a sensitivity analysis to determine the robustness of the summary estimates by removing each included study from the analysis one by one. Furthermore, subgroup analyses based on reported comorbidities, as well as meta-regression models considering mean age, sample size, length of the intervention, T2DM duration (years), total body fat percentage, glycosylated hemoglobin (HbA1c, %), blood glucose levels (mg/dL), and percentage of women, to determine their influence on the SMD estimates and on the raw MD for CRP levels were conducted. Moreover, we explore whether the MD on CRP levels (mg/dL) between resistance exercise and CG could be influenced by baseline HbA1c levels (%) considering as a cut point the median value of HbA1c among the studies (7.5%). Finally, we evaluated publication bias through visual inspection of funnel plots and Egger’s regression asymmetry test to assess small study effects [23]. We performed all statistical analyses using Stata SE version15 (StataCorp., College Station, TX, USA).
METHODS
- Study selection
- After duplicated articles were removed and analyzed by title and abstract, a total of 57 full-text articles were assessed for eligibility, of which 13 [24-36] were included in the systematic review, and 11 RCTs [25-34,36] were included for the meta-analysis on CRP levels (Fig. 1). The excluded studies with reasons for exclusion after full-text reading are available in Supplementary Table 2.
- Characteristics of studies
- The 13 RCTs included with a parallel design were conducted between 2006 and 2021. The studies were conducted in different countries such as Australia, Brazil, Grecia, Iran, Spain, Sri Lanka, Taiwan, and the USA. Further details are available in Table 1.
- Participants
- A total of 568 adults with T2DM (mean age between 48 and 72 years) were included. Among the participants, 261 adults were in the resistance exercise groups, and 256 were in the control conditions. Most studies had similar rates of men and women, except for one study in which only males were included [36]. The baseline BMI values of the participants ranged from 25 to 35 kg/m2 (Table 1). Moreover, six studies reported comorbidities across the included population, such as overweight and obesity [27,29,30,32,34,35]. The most reported medications prescribed were hypoglycemic, antihypertensive, and lipidlowering drugs. Further details of the covariates are available in Supplementary Table 3.
- Interventions
- Although the resistance exercise protocols were different across the intervention groups, the training length was set between 60 and 75 minutes, with a frequency of two to three sessions per week for 12 to 16 weeks. Eight studies performed resistance exercise with global protocols (i.e., upper limbs, core, and lower limbs) [26-29,31,33,34,36], four studies only included lower or upper limbs [24,25,30,32], and one study did not report the protocol [35]. Resistance exercise was performed using calisthenic exercises [26-28,34,36], dumbbells [24-27,29-33,35,36], and machines [24-28,30,34-36]. However, it was not reported to the rest of the groups [29,31-33].
- Among the CG there were five studies in which participants received usual care and advice through medical visits or by telephone [24,25,27,28,33,34]; four studies in which participants received recommendations about physical activity [30,32,33,35] and three studies that included a general stretching protocol [26,29,31].
- Outcome
- The CRP values were evaluated in 11 [25-34,36] out 13 included studies. Six studies measured TNF-α values [24,26,28,29,35,36], five studies measured IL-6 [26,28,29,35,36], and two studies reported IL-10 values [26,35]. Overall, inflammatory biomarkers were analyzed according to the clinical standards of the laboratory or the manufacturer’s guidelines with enzyme-linked immunosorbent assay (ELISA).
- Risk of bias
- When the RoB2 tool was used to assess the risk of bias, nine out of 11 studies scored at ‘low risk of bias’ [24-27,29,31,33,35,36], and four scored at ‘some concerns’ [28,30,32,34]. The risk of bias assessment is displayed in Supplementary Fig. 1.
- Quality of evidence
- The quality of evidence was rated as high for CRP outcomes, since the certainty assessment showed low concerns regarding the risk of bias, inconsistency, and imprecision. A table with a summary of the findings is available in Supplementary Table 4.
- Data synthesis
- The SMDs for the effect on CRP of resistance exercise versus control was –0.20 (95% CI, –0.37 to –0.02; I2=0%) (Fig. 2). Considering the mean raw difference in CRP levels, after resistance exercise, there was a significant reduction of -0.59 mg/dL (95% CI, –0.88 to –0.30; I2=55%); otherwise, the CRP values showed an increase in the CG of 0.19 mg/dL (95% CI, 0.17 to 0.21; I2=0%) (Fig. 3).
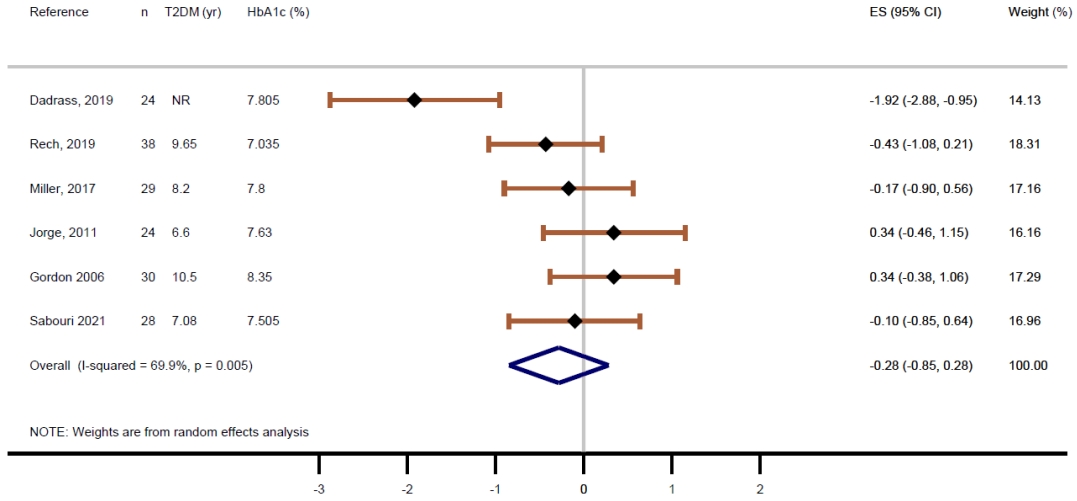
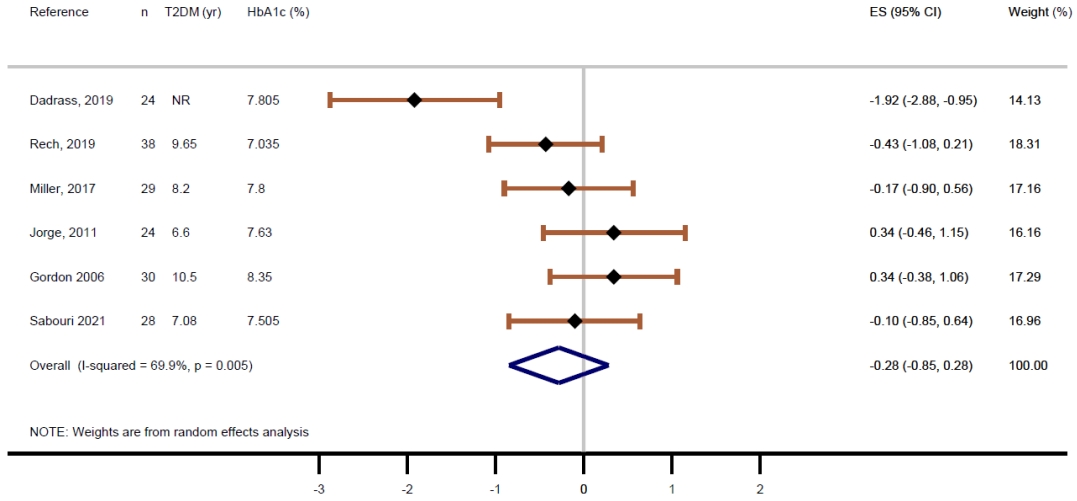
- The SMDs for the effect on TNF-α of resistance exercise versus CG showed a slight nonsignificant effect of –0.28 (95% CI, –0.85 to 0.28; I2=69.9%) (Fig. 4), as well as when considering IL-6 (SMD, –0.24; 95% CI, –1.43 to 0.96; I2=89.2%) (Fig. 5). Additionally, the effect plot without pooling the SMD for IL-6 and IL-10 are available in Supplementary Fig. 2.
- The negative SMD on CRP values was not modified when removing each included study one by one. Further details are displayed in Supplementary Table 5.
- The subgroup analysis considering potential comorbidities (i.e., overweight/obesity, hypertension) showed no differences in CRP values between participants with reported comorbidities (SMD, –0.12; 95% CI, –0.34 to 0.10; I2=0%) and those without them (SMD, –0.31; 95% CI, –0.63 to 0.01; I2=23%) (Supplementary Table 6). Regarding the coefficients and P values of the meta-regression models conducted for mean age (P=0.62), sample size (P=0.33), length of the intervention (P=0.22), T2DM duration (years) (P=0.78), total body fat percentage (P=0.66), HbA1c (%) (P=0.68), blood glucose levels (mg/dL) (P=0.76), and percentage of women (P=0.50), none of them significantly influenced the effects of resistance exercise on CRP levels (Supplementary Table 7). Meta-regression models conducted for the raw MD in CRP values showed a significant effect of baseline HbA1c (%) for the resistance exercise group (coef=0.78; P=0.01), while for the CG there was no significant effect of baseline HbA1c (%) (coef=–0.32; P=0.39) (Supplementary Table 8 and Supplementary Fig. 3). Finally, baseline HbA1c levels (%) influenced the response of resistance exercise when compared to CG, showing a significant reduction of –0.71 mg/dL (95% CI, –0.81 to –0.61; I2=0%) in CRP values in those patients with mean baseline HbA1c <7.5% (Supplementary Fig. 4).
- Funnel plot visual assessment and Egger’s test confirmed no significant publication bias regarding CRP levels among the RCTs included in the meta-analysis (P=0.388) (Supplementary Fig. 5).
RESULTS
Meta-analysis
Sensitivity analysis
Subgroup analyses and meta-regression
Publication bias
- This study aimed to systematically synthesize the evidence regarding resistance exercise effectiveness on inflammatory markers in adults diagnosed with T2DM. Our findings suggest that resistance exercise may reduce CRP values in patients with T2DM. When exploring potential effect modifiers such as comorbidities, age, sample size, length of the intervention, time since T2DM diagnosis, total body fat percentage, blood glucose levels, and percentage of women, none of them significantly influenced the effect size estimates for CRP levels. As an exception, baseline HbA1c (%) had a significant effect on the MD in CRP levels for resistance exercise groups, showing that when patients had higher levels of HbA1c, the anti-inflammatory effects of resistance exercise would be reduced. However, evidence regarding TNF-α, IL-6, and IL-10 levels is scarce, and the corresponding results are far from consistent.
- Circulating CRP levels were the most reported outcome. Most studies, except one [29], did not show a significant reduction in CRP values [25-34,36] compared to the control condition. Otherwise, when clinical differences were considered with the raw MD estimates, our results showed a significant reduction of CRP for resistance exercise while CG increased their values of CRP in mg/dL. Accordingly, previous evidence has demonstrated agreement with these results for patients with T2DM [37] and healthy participants [38]. However, these increased CRP levels after control conditions observed in seven out 10 studies were only significant in one study [30]. Of note, in this specific study, changes in CRP levels of the participants could be associated with their baseline clinical characteristics because they were obese (BMI, 32 kg/m2) with high fat mass percentage (34%), triglyceride levels (195 mg/dL), and insulin values (10.24 mU/L) [30]. Moreover, the overall increased CRP in the CG was markedly heterogeneous and may be related to the different recommendations given to the CG (i.e., no intervention, usual care, physical activity or healthy diet advice, low-impact activities, etc.). Despite this, a clinical message could be extrapolated: the resistance exercise seems to be a better option than the different control conditions to manage systemic inflammation for patients with T2DM. It would be worth noting that there are some potential factors not fully described among the studies that should be considered as the baseline diet quality [39], diets based on anti-inflammatory foods [40] or the physical activity levels sustained throughout life that may attenuate the progression on inflammation caused by the disease and the aging process [41].
- Despite this modest benefit on circulating CRP levels, other key factors associated with high oxidative stress in patients with T2DM could influence resistance exercise effectiveness, such as smoking status, physical inactivity, increased adiposity levels, diet [42], and pharmacological treatments [43], which could mask the effect of exercise in the T2DM population. In this sense, when we explored the meta-regression models for raw MD on circulating CRP levels, we found that the baseline HbA1c (%) may modify significantly the effect in the resistance exercise groups but no in CG. Of note that the pooled baseline HbA1c values for participants in the resistance exercise groups were slightly lower (7.5%) than for CG (7.7%), and only two studies reported good metabolic control (<7%) for the resistance exercise groups [26,33]. Because of the scarcity of trials making it difficult to clearly interpret this, it would be interesting that further studies explore the potential moderating role of HbA1c in the effectiveness of resistance exercise in patients with T2DM.
- Most studies have reported lower circulating TNF-α levels after resistance exercise [26,35,36]. Our meta-analysis showed a slight nonsignificant effect of resistance exercise for reducing TNF-α levels when compared to CG, which is similar to the results reported in a previous systematic review exploring the effects of aerobic exercise on inflammatory markers in T2DM patients [37]. However, two studies reported increased TNF-α levels after resistance exercise [24,29]. Specifically, in the study of Gordon et al. [24], the authors reported an increase in TNF-α expression in the trained muscle, but suggested that the poorly controlled T2DM and the elevated number of years with T2DM (10.5 years) could affect their results. Moreover, in Jorge et al. [29], the increased TNF-α levels could be explained because of the baseline differences in the HbA1c levels (%) for the resistance exercise group (8.27%) and the CG (6.99%); in addition, the authors also suggest that this surprising negative effect could be attributed by the poor metabolic control of participants. Even if the impact of resistance exercise on TNF-α levels are still unclear and needs to be further explored, it should be considered that increased muscle mass (hypertrophy) may be associated with decreased inflammation through the improvement in blood glucose levels and insulin resistance [25]. Moreover, when resistance exercise is prescribed to patients with T2DM, we should consider some factors that negatively impact muscle strength and progression of the disease such as age, diabetes duration, or fat percentage [44].
- Despite the potential role of IL-6 and IL-10 have in the inflammatory response, few studies have reported their circulating levels. In this sense, our data showed a slight nonsignificant effect of resistance exercise for reducing IL-6 values when compared to CG, with some studies showing a reduction in IL-6 [28,35,36], while others showed a nonsignificant increase after resistance exercise [26,29]. We must be cautious when interpreting these results as the increase in IL-6 reported in Jorge et al. [29] could be affected due to the high HbA1c levels (%) shown in the intervention group (8.27%) compared to the CG (6.99%); thus, this fact should be further explored in future trials. Moreover, in Rech et al. [26] the age of the participants may affect as older patients could need longer interventions to account for positive effects on inflammatory biomarkers or glycemic response; moreover, their life habits exceed the accuracy of the questionnaire (mainly in the CG), which may also have influenced the results.
- When considering the anti-inflammatory cytokine IL-10, the response after resistance exercise was not homogenous, showing nonsignificant reduced [35] or increased [26] circulating levels of IL-10. Although the scarcity of studies reporting this cytokine makes it difficult to better clarify the potential role of resistance exercise in the IL-10 response, it is recommended that future RCTs include IL-6 and IL-10 accounting for factors (i.e., physical activity status, diet, characteristics of the resistance exercise program, etc.) that could be potentially mediate the effect of resistance exercise on the response of these biomarkers.
- Some mechanisms should be stated when considering the potential benefits of resistance exercise on inflammation. First, acute exercise stimulates the release of IL-6 in muscular tissue, which may act at the systemic level, inhibiting proinflammatory cytokines such as TNF-α and increasing anti-inflammatory cytokines such as IL-10 [45]. Second, resistance exercise is associated with increased muscle mass, which may improve insulin sensitivity due to the key role of skeletal muscle in glucose uptake [25]. Third, resistance exercise could act on adipose tissue, diminishing adiposity, thus improving insulin sensitivity [46] and increasing vasodilatation, angiogenesis and blood flow, which may cause a reduction in hypoxia, macrophage infiltration and chronic inflammation in adipose tissue [45]. Moreover, mechanisms contributing to sarcopenia are also crucial to metabolic disorder pathogenesis (bidirectional relationship), with inflammation being a typical process involved in T2DM and skeletal muscle structure [47]. Finally, it is worth noting the influence of regular resistance exercise on the immune system, such as an increased T-cell count, which is related to IL-10 release and reduced expression of receptors associated with the production of inflammatory cytokines [45].
- Otherwise, the inconclusive results shown in some studies might be due to some related factors, such as weight gain, physical inactivity, and genetic predisposition, that may cause adipose tissue dysfunction and increased secretion of CRP, TNF-α, and IL-6 and decreased adiponectin levels (anti-inflammatory protein) [4]. In addition, age is a crucial factor in the progression of T2DM, the aging process is associated with increased levels of some inflammatory cytokines [48]. Of note, weight gain produced by some usual medications in T2DM, such as insulin and sulfonylureas, may also impact the results.
- Adding to the abovementioned confounding factors that may impact the results from primary studies, our review has some limitations that should be noted. First, the included exercise studies were not blinded because it would be impossible to truly blind participants to treatment allocation. Second, the heterogeneity among pharmacological treatments in patients with T2DM may introduce some kind of bias in our estimates. Third, the small total sample size (n=568), added to the heterogeneity among resistance exercise protocols and the nonreported exercise intensity in some studies, should be considered. Fourth, the overall metabolic control of participants included could have affected our estimates. Finally, studies evaluating the resistance exercise effect on the inflammatory response in patients with T2DM in the long term are lacking.
- In summary, our analyses suggest a significant reduction in CRP values after resistance exercise in patients with T2DM. Moreover, potential effect modifiers such as comorbidities, age, sample size, length of the intervention, time since T2DM diagnosis, total body fat percentage, blood glucose levels, and percentage of women did not significantly influence our effect size estimates, except for baseline HbA1c (%). Regarding TNF-α and IL-6 levels, resistance exercise showed a nonsignificant reduction. However, future trials would help to elucidate the controversial and heterogenous results for TNF-α, IL-6, and IL-10 levels. Thus, further studies should consider confounding factors that may have a direct or indirect impact on inflammatory biomarker levels (i.e., HbA1c levels, diabetes duration, diet quality, physical activity status, body composition, pharmacological treatments). Additionally, assessments of resistance exercise benefits in inflammatory biomarkers in patients with T2DM in the long term are strongly required. Current evidence indicates that prescribing resistance exercise to patients with T2DM can reduce inflammatory marker levels, specifically CRP in addition to the known benefits on body composition and metabolic parameters.
DISCUSSION
SUPPLEMENTARY MATERIALS
Supplementary Table 2.
Supplementary Table 3.
Supplementary Table 4.
Supplementary Table 6.
Supplementary Table 7.
Supplementary Table 8.
Supplementary Fig. 1.
Supplementary Fig. 2.
Supplementary Fig. 3.
Supplementary Fig. 4.
Supplementary Fig. 5.
-
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
AUTHOR CONTRIBUTIONS
Conception or design: R.F.R., S.M.C., B.B.P.
Acquisition, analysis, or interpretation of data: R.F.R., S.M.C., M.G.M., A.E.M., V.M.V.
Drafting the work or revising: R.F.R., S.M.C.
Final approval of the manuscript: R.F.R., S.M.C., B.B.P., M. G.M., A.E.M., V.M.V.
-
FUNDING
This study was funded by the European Regional Development Fund. The funding source had no such involvement or restrictions regarding publication. Bruno Bizzozero-Peroni is supported by a grant from the Universidad de Castilla-La Mancha co-financed by the European Social Fund (2020-PREDUCLM-16746). Arthur Eumann Mesas was supported by a ‘Beatriz Galindo’ contract (BEAGAL18/00093) by the Spanish Ministry of Education, Culture and Sport.
NOTES
-
Acknowledgements
- None


| Study | Sample size (% women) | Age, mean±SD, yr | Characteristics of the intervention | Comparison | Outcome | Main results | ||
|---|---|---|---|---|---|---|---|---|
| Gordon et al. (2006) [24] | n=30 (50%) | RE=67±2 | RE protocol | CG | TNF-α | No significant increase of TNF-α in the RE group, and no significant change in the CG. | ||
| RE=15 | CG=67±2 | →3×wk; 16 wk | → Telephone monitoring and face-to-face visits | |||||
| CG=15 | → Session: warm-up (5 min gentle walk+stretching); training (upper and lower body-machines)+T2DM related care | |||||||
| → Intensity: 60%–65% of 1 RM and progress 75%–80% of 1 RM at the end of the first 4 wk (wk 8 and 16 re-evaluation of 1 RM) | ||||||||
| → 3 sets of 8 reps, 3 sec rest between reps and 1–2 min between sets | ||||||||
| Brooks et al. (2006) [25] | n=62 (35.5%) | RE=66±2 | RE protocol | RE | CRP | CRP decreased in favor of RE but not significantly. | ||
| RE=31 | CG=66±1 | → 3×wk; 16 wk | → 16 wk | |||||
| CG=31 | → Supervised session: warm-up (5 min)–workout (35 min-upper and lower body-machines)–cool down (5 min)+standard care | → Standard care (health, glycemic control, self-monitoring, physical activity, medications and medical visits) | ||||||
| → Intensity: 60%–80% of 1 RM (1–8 wk) and 70%–80% of 1 RM (10–14 wk) | ||||||||
| → 3 sets of 8 reps/machine | ||||||||
| Jorge et al. (2011) [29] | n=24 (62.5%) | (53.9±9.9) | RE protocol | CG | TNF-α | hs-CRP decreased significantly in all groups. TNF-α and IL-6 increased in the ST group but not significantly. | ||
| RE=12 | RE=54±8.9 | → 3×wk; 12 wk | → 3×wk; 12 wk | CRP | ||||
| CG=12 | CG=53±9.8 | → Supervised session: training (60 min circuit 7 full body exercises: large muscle groups) | → Stretching | IL-6 | ||||
| AE=52±8.7 | AE | |||||||
| ST+AE=58±9.8 | → 60 min, 3×wk, 12 wk | |||||||
| → Supervised session: cycling | ||||||||
| → Intensity: heart rate according to lactate threshold | ||||||||
| RE+AE | ||||||||
| → 3×wk, 12 wk | ||||||||
| → Same intensity and volume | ||||||||
| Kadoglou et al. (2012) [30] | n=47 (25.53%) | RE=62±5.4 | RE protocol | CG | CRP | hs-CRP decreased in favor of RE group when compared to CG but not significantly. | ||
| RE=23 | CG=65±4.3 | → 45 min (basal) and 60 min (progression), 3×wk; 12 wk | → 150 min/wk: advice+daily physical activity (walking, cycling, swimming) varying from low to high intensity | |||||
| CG=24 | → Supervised session: calisthenics (jumping, skipping, gymnastics, ball games); training (upper and lower body: machines)–calisthenics (idem) | |||||||
| → Intensity: 60%–80% of 1 RM, 2–3 sets of 6–8 repetitions/exercise | ||||||||
| → 8 exercises with 1 min rest between exercises and 3 min between sets | ||||||||
| Swift et al. (2012) [31] | n=87 (61%) | (57.3±8.1) | RE protocol | CG | CRP | All intervention groups showed lower levels of CRP when compared to CG but not significantly. | ||
| RE=50 | RE=59±8 | → 3×wk, 36 wk | → 36 wk. No exercise prescription. Weekly stretching and relaxation classes | |||||
| CG=37 | CG=59±8.6 | → Supervised session: workout (whole body) | AE | |||||
| AE=56±7.9 | → 12 kcal/kg/wk | |||||||
| RE+AE=57±7.8 | → Intensity: 2 sets of 4 exercises (upper body), 3 sets of 3 exercises (lower body) and 2 sets of abs and back | → Supervised session: alternating walking on treadmill and cycling | ||||||
| → Intensity: 50%–80% maximal oxygen uptake | ||||||||
| → Each exercise 10–12 repetitions | RE+AE | |||||||
| → AE (supervised): | ||||||||
| → Weight progressively increased when the participant completed 12 repetitions of all exercises in 2 consecutive sessions | -10 kcal/kg/wk | |||||||
| - Intensity: 50%–80% maximal oxygen uptake | ||||||||
| → RE (supervised): | ||||||||
| -2*wk | ||||||||
| -9 exercises×1 set, incremental load | ||||||||
| Kadoglou et al. (2013) [32] | n=47 (27.78%) | RE=56±5.3 | RE protocol | CG | CRP | hs-CRP decreased in favor of AE, RE+AE when compared to RE and CG groups. | ||
| RE=23 | CG=58±7.2 | → Gradual increase of duration first 4 wk, then, 60 min 4×wk, 24 wk | → Physical activity (150 min/wk): low to moderate intensity walking | |||||
| CG=24 | AE=58±5.4 | → Supervised session: calisthenics (10 min)–training (8 upper and lower body exercises) | AE | |||||
| RE+AE= 58±6.5 | → Gradual duration over 4 wk; then 60 min, 4×wk, 6 mo | |||||||
| → Intensity: 60%–80% of 1 RM | → Supervised session: warm-up (10 min)–workout (45 min-walk- or run-on treadmill, bike or calisthenics)–cool down (5 min) | |||||||
| → 2–3 sets of 8–10 reps/exercise and 8 exercises | → Intensity: gradual over 4 wk, then 60%–75% of HRmax | |||||||
| RE+AE | ||||||||
| → 4×wk (1 of AE+1 of ST+2 of AE+ST), 6 mo | ||||||||
| → Session: warm up (10 min)–ST+AE training (45 min)–cool down (5 min) | ||||||||
| → Intensity: gradually increased during first 4 wk | ||||||||
| Mavros et al. (2014) [33] | n=69 (47.7%) | (68.2±5.7) | RE protocol | CG | CRP | CRP showed a not significant diminish in the RE group compared to CG. | ||
| RE=30 | RE=67±4.9 | → 3×wk, 48 wk | → 3×wk, 48 wk | |||||
| CG=39 | CG=69±6.3 | → Supervised session: training: concentric contraction (+fast as possible) and eccentric contraction 4 sec–whole body | → Non-progressive and low-intensity exercise, under supervision+regular care | |||||
| → Intensity: 80% of 1 RM (re-evaluation every 4 wk), 3 sets of 8 repetitions (2 sets of 8 for hip flexion, extension, and abduction) | ||||||||
| Hsieh et al. (2018) [34] | n=30 (63.3%) | RE=71±4.2 | RE protocol | CG | CRP | CRP levels decreased in RE group and increased in the CG but not significantly. | ||
| RE=15 | CG=72±4.5 | → 3×wk, 12 wk | → 3×wk, 12 wk | |||||
| CG=15 | → Supervised session: training–8 full body exercises (machines and body weight) | → Standard care and maintaining their daily activities and lifestyle | ||||||
| → 3 sets of 8–12 repetitions. Rest 60–90 sec between sets | ||||||||
| → Intensity: 40%–50% of 1 RM or 12–13 on the Borg scale | ||||||||
| → Progression 75% of 1 RM or 14–16 on the Borg scale at wk 12 | ||||||||
| Miller et al. (2017) [35] | 1) n=29 (44.8%) | RE+CD= 68±5.2 | RE+control diet (CD), (ST+CD) | CG+CD | TNF-α | No significant changes (TNF-α, IL-6, IL‑10) after 3, 6, 9, or 12 mo, except for TNF-α that showed a significant decrement at 9 and 12 mo for ST+CD when compared to CG+CD, and IL-10, which diminish significantly after 9 mo in the RE+CD group compared to CG+CD. | ||
| RE=16 | CG+CD= 67±5.3 | First phase (6 mo): 45 min, 3×wk, 24 wk | → 1st phase (6 mo): static pedalling without load+5 min of static stretching+healthy eating plan (evaluation every 2 wk) | IL-10 | ||||
| CG=13 | → Session: training (9 exercises–weights and machines)+healthy eating plan (evaluation every 2 wk) | IL-6 | ||||||
| 2) n=26 (44.8%) | → Intensity: 75%–85% of 1 RM, 3 sets of 8–10 repetitions | → 2nd phase (6 mo): static pedalling without load+5 min of static stretching | ||||||
| RE=14 | → Second phase (6 mo): 45 min, 3×wk, 24 wk | |||||||
| CG=12 | → Session: training (home exercises with dumbbells) | |||||||
| → Intensity: 60% of 1 RM | ||||||||
| → 3 sets of 8–10 repetitions | ||||||||
| Dadrass et al. (2019) [36] | n=24 (0%) | RE protocol | RE protocol | CG | IL-6 | IL-6 decreased significantly in all groups. TNF-α decreased significantly in ST+VitD and there were no changes in CG and GVitD. CRP decreased not significantly in all groups. | ||
| RE=12 | RE=55±5.9 | → 70 min, 3×wk, 12 wk | → Normal daily life+oral capsules (placebo) every 2 wk for 12 wk | TNF-α | ||||
| CG=12 | CG=53±8 | → Session: warm-up (10 min–walking and stretching); training (50 min–whole body-body weight and machines)–cool-down (10 min–stretching) | RE+VitD | CRP | ||||
| RE+VitD= 54±8 | → Intensity: 55% of 1 RM (1st mo); 65% of 1 RM (2nd mo) and 75% of 1 RM (3rd mo). Recalculated (4 and 8 wk) | → RE+VitD every 2 wk for 12 wk | ||||||
| VitD= 54±6.6 | → 10 exercises, 3 sets of 10 reps/exercise with 90 sec rest between sets and 30 sec between exercises | VitD | ||||||
| → Oral capsules (placebo) every 2 wk for 12 wk | → VitD every 2 wk for 12 wk | |||||||
| Rech et al. (2019) [26] | n=38 (47.4%) | RE=71±7.4 | → 3×wk, 12 ek | CG | TNF-α | TNF-α and ratio TNF-α/IL-10 decreased significantly in both groups. IL-6 and IL‑10 increased, and CRP decreased, but there were no significant interactions reported. | ||
| RE=17 | CG=68±6.5 | → Session: warm-up (on treadmill); training (functional exercises [i.e., step, squats]; and traditional (i.e., whole body using body weight and machines])–stretching exercises | → 45 min/session: joint mobilization+static stretching of large muscle groups (20–30 sec) | IL-10 | ||||
| CG=21 | → Intensity: f.e., intensity controlled through an scale (progress from 2 to 3 sets/exercise with 10–15 repetitions and 1 min rest); t.e., (progress from 2 to 3 sets/exercise and 12 to 10 repetitions, 1 min rest and 1.3 min progress) | CRP | ||||||
| IL-6 | ||||||||
| Ranasinghe et al. (2021) [27] | n=53 (53%) | (50.1±8.7) | RE protocol | CG | CRP | RE and AE decreased not significantly CRP levels when compared to CG. | ||
| RE=25 | RE=49±9 | → 60–75 min, 2×wk, 12 wk | → Usual clinic visits and contact once every 2 wk for 12 wk | |||||
| CG=28 | CG=49±7 | → Supervised session: warm-up (10 min–treadmill walking); workout (whole body–body weight, free weights, and machines)–cool down (10 min–dynamic and static stretching) | AE | |||||
| AE=52±9.8 | → 75 min, 2×wk, 12 wk | |||||||
| → Intensity: 50%–60% of 1 RM. Increase weight by 5% every 2 wk | → Supervised session: warm up (10 min–treadmill walking)–workout (circuit-walking, step, exercise bike)–cool down (10 min–static stretching) | |||||||
| → 3 sets of 8–10 repetitions | → Intensity: 60%–75% HRmax | |||||||
| Sabouri et al. (2021) [28] | n=28 (45.8%) | (50.1±8.7) | RE protocol | CG | TNF-α | TNF-α, IL-6, and CRP showed a significant decrease in RE groups. CG showed a nonsignificant decrease in TNF-α and IL‑6 and nonsignificant increase of CRP. | ||
| RE=15 | RE=51±4.5 | → 3×wk, 12 wk | → No intervention, 12 wk | CRP | ||||
| CG=13 | CG=52±3.2 | → Supervised session: 3 sets of 8 reps max RM (upper and lower body)+3 sets of 15 reps (abdomen), 1 min rest between sets | HIIT | IL-6 | ||||
| → 3×wk, 12 wk | ||||||||
| → Supervised session: at cycloergometer with protocol: 10×60 sec at 85%–90% of HRmax, 1 min of active recovery | ||||||||
| → Intensity: maximum weight for 8 repetitions | HIIT+ST | |||||||
| → 3×wk, 12 wk | ||||||||
| → Supervised session: first ST, then HIIT | ||||||||
SD, standard deviation; RE, resistance exercise; CG, control group; T2DM, type 2 diabetes mellitus; RM, repetition maximum; TNF-α, tumor necrosis factor alpha; CRP, C-reactive protein; AE, aerobic exercise; IL-6, interleukin-6; hs-CRP, high-sensitivity C-reactive protein; HRmax, heart rate max; CD, control diet; IL-10, interleukin-10; VitD, vitamin D; HIIT, high intensity interval training.
- 1. Saeedi P, Petersohn I, Salpea P, Malanda B, Karuranga S, Unwin N, et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res Clin Pract 2019;157:107843.ArticlePubMed
- 2. Teixeira-Lemos E, Nunes S, Teixeira F, Reis F. Regular physical exercise training assists in preventing type 2 diabetes development: focus on its antioxidant and anti-inflammatory properties. Cardiovasc Diabetol 2011;10:12.ArticlePubMedPMCPDF
- 3. Berbudi A, Rahmadika N, Tjahjadi AI, Ruslami R. Type 2 diabetes and its impact on the immune system. Curr Diabetes Rev 2020;16:442-9.ArticlePubMedPMC
- 4. Calle MC, Fernandez ML. Inflammation and type 2 diabetes. Diabetes Metab 2012;38:183-91.ArticlePubMed
- 5. King GL. The role of inflammatory cytokines in diabetes and its complications. J Periodontol 2008;79(8 Suppl):1527-34.ArticlePubMed
- 6. Neeland IJ, Turer AT, Ayers CR, Powell-Wiley TM, Vega GL, Farzaneh-Far R, et al. Dysfunctional adiposity and the risk of prediabetes and type 2 diabetes in obese adults. JAMA 2012;308:1150-9.ArticlePubMedPMC
- 7. Trayhurn P, Wood IS. Signalling role of adipose tissue: adipokines and inflammation in obesity. Biochem Soc Trans 2005;33(Pt 5):1078-81.ArticlePubMed
- 8. Balducci S, Sacchetti M, Haxhi J, Orlando G, D’Errico V, Fallucca S, et al. Physical exercise as therapy for type 2 diabetes mellitus. Diabetes Metab Res Rev 2014;30 Suppl 1:13-23.ArticlePubMed
- 9. Melo LC, Dativo-Medeiros J, Menezes-Silva CE, Barbosa FT, de Sousa-Rodrigues CF, Rabelo LA. Physical exercise on inflammatory markers in type 2 diabetes patients: a systematic review of randomized controlled trials. Oxid Med Cell Longev 2017;2017:8523728.ArticlePubMedPMCPDF
- 10. Chen X, Sun X, Wang C, He H. Effects of exercise on inflammatory cytokines in patients with type 2 diabetes: a meta-analysis of randomized controlled trials. Oxid Med Cell Longev 2020;2020:6660557.ArticlePubMedPMCPDF
- 11. Acosta-Manzano P, Rodriguez-Ayllon M, Acosta FM, Niederseer D, Niebauer J. Beyond general resistance training. Hypertrophy versus muscular endurance training as therapeutic interventions in adults with type 2 diabetes mellitus: a systematic review and meta-analysis. Obes Rev 2020;21:e13007.PubMed
- 12. Maestroni L, Read P, Bishop C, Papadopoulos K, Suchomel TJ, Comfort P, et al. The benefits of strength training on musculoskeletal system health: practical applications for interdisciplinary care. Sports Med 2020;50:1431-50.ArticlePubMedPDF
- 13. Andersen H, Nielsen S, Mogensen CE, Jakobsen J. Muscle strength in type 2 diabetes. Diabetes 2004;53:1543-8.ArticlePubMedPDF
- 14. Celis-Morales CA, Petermann F, Hui L, Lyall DM, Iliodromiti S, McLaren J, et al. Associations between diabetes and both cardiovascular disease and all-cause mortality are modified by grip strength: evidence from UK Biobank, a prospective population-based cohort study. Diabetes Care 2017;40:1710-8.ArticlePubMedPDF
- 15. American Diabetes Association. 5. Facilitating behavior change and well-being to improve health outcomes: standards of medical care in diabetes-2021. Diabetes Care 2021;44(Suppl 1):S53-72.ArticlePubMedPDF
- 16. Hayashino Y, Jackson JL, Hirata T, Fukumori N, Nakamura F, Fukuhara S, et al. Effects of exercise on C-reactive protein, inflammatory cytokine and adipokine in patients with type 2 diabetes: a meta-analysis of randomized controlled trials. Metabolism 2014;63:431-40.ArticlePubMed
- 17. Higgins J, Green S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (Updated March 2011). Available from: https://handbook-5-1.cochrane.org (cited 2022 Mar 23).
- 18. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71.ArticlePubMedPMC
- 19. Sterne JAC, Savovic J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ 2019;366:l4898.ArticlePubMed
- 20. Guyatt G, Oxman AD, Akl EA, Kunz R, Vist G, Brozek J, et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J Clin Epidemiol 2011;64:383-94.ArticlePubMed
- 21. DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials 1986;7:177-88.ArticlePubMed
- 22. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med 2002;21:1539-58.ArticlePubMed
- 23. Page MJ, Sterne J, Higgins J, Egger M. Investigating and dealing with publication bias and other reporting biases in meta-analyses of health research: a review. Res Synth Methods 2021;12:248-59.ArticlePubMedPDF
- 24. Gordon PL, Vannier E, Hamada K, Layne J, Hurley BF, Roubenoff R, et al. Resistance training alters cytokine gene expression in skeletal muscle of adults with type 2 diabetes. Int J Immunopathol Pharmacol 2006;19:739-49.ArticlePubMedPDF
- 25. Brooks N, Layne JE, Gordon PL, Roubenoff R, Nelson ME, Castaneda-Sceppa C. Strength training improves muscle quality and insulin sensitivity in Hispanic older adults with type 2 diabetes. Int J Med Sci 2006;4:19-27.ArticlePubMedPMC
- 26. Rech A, Botton CE, Lopez P, Quincozes-Santos A, Umpierre D, Pinto RS. Effects of short-term resistance training on endothelial function and inflammation markers in elderly patients with type 2 diabetes: a randomized controlled trial. Exp Gerontol 2019;118:19-25.ArticlePubMed
- 27. Ranasinghe C, Devage S, Constantine GR, Katulanda P, Hills AP, King NA. Glycemic and cardiometabolic effects of exercise in South Asian Sri Lankans with type 2 diabetes mellitus: a randomized controlled trial Sri Lanka diabetes aerobic and resistance training study (SL-DARTS). Diabetes Metab Syndr 2021;15:77-85.ArticlePubMed
- 28. Sabouri M, Hatami E, Pournemati P, Shabkhiz F. Inflammatory, antioxidant and glycemic status to different mode of high-intensity training in type 2 diabetes mellitus. Mol Biol Rep 2021;48:5291-304.ArticlePubMedPDF
- 29. Jorge ML, de Oliveira VN, Resende NM, Paraiso LF, Calixto A, Diniz AL, et al. The effects of aerobic, resistance, and combined exercise on metabolic control, inflammatory markers, adipocytokines, and muscle insulin signaling in patients with type 2 diabetes mellitus. Metabolism 2011;60:1244-52.ArticlePubMed
- 30. Kadoglou NP, Fotiadis G, Athanasiadou Z, Vitta I, Lampropoulos S, Vrabas IS. The effects of resistance training on ApoB/ ApoA-I ratio, Lp(a) and inflammatory markers in patients with type 2 diabetes. Endocrine 2012;42:561-9.ArticlePubMedPDF
- 31. Swift DL, Johannsen NM, Earnest CP, Blair SN, Church TS. Effect of exercise training modality on C-reactive protein in type 2 diabetes. Med Sci Sports Exerc 2012;44:1028-34.ArticlePubMedPMC
- 32. Kadoglou NP, Fotiadis G, Kapelouzou A, Kostakis A, Liapis CD, Vrabas IS. The differential anti-inflammatory effects of exercise modalities and their association with early carotid atherosclerosis progression in patients with type 2 diabetes. Diabet Med 2013;30:e41-50.ArticlePubMed
- 33. Mavros Y, Kay S, Simpson KA, Baker MK, Wang Y, Zhao RR, et al. Reductions in C-reactive protein in older adults with type 2 diabetes are related to improvements in body composition following a randomized controlled trial of resistance training. J Cachexia Sarcopenia Muscle 2014;5:111-20.ArticlePubMedPMC
- 34. Hsieh PL, Tseng CH, Tseng YJ, Yang WS. Resistance training improves muscle function and cardiometabolic risks but not quality of life in older people with type 2 diabetes mellitus: a randomized controlled trial. J Geriatr Phys Ther 2018;41:65-76.ArticlePubMed
- 35. Miller EG, Sethi P, Nowson CA, Dunstan DW, Daly RM. Effects of progressive resistance training and weight loss versus weight loss alone on inflammatory and endothelial biomarkers in older adults with type 2 diabetes. Eur J Appl Physiol 2017;117:1669-78.ArticlePubMedPDF
- 36. Dadrass A, Mohamadzadeh Salamat K, Hamidi K, Azizbeigi K. Anti-inflammatory effects of vitamin D and resistance training in men with type 2 diabetes mellitus and vitamin D deficiency: a randomized, double-blinded, placebo-controlled clinical trial. J Diabetes Metab Disord 2019;18:323-31.ArticlePubMedPMCPDF
- 37. Melo LC, Dativo-Medeiros J, Menezes-Silva CE, Barbosa FT, de Sousa-Rodrigues CF, Rabelo LA. Physical exercise on inflammatory markers in type 2 diabetes patients: a systematic review of randomized controlled trials. Oxid Med Cell Longev 2017;2017:8523728.ArticlePubMedPMCPDF
- 38. Cronin O, Keohane DM, Molloy MG, Shanahan F. The effect of exercise interventions on inflammatory biomarkers in healthy, physically inactive subjects: a systematic review. QJM 2017;110:629-37.ArticlePubMed
- 39. Coelho DB, Lopes L, de Oliveira EC, Becker LK, de Paula Costa G, Hermsdorff H, et al. Baseline diet quality is related to changes in the body composition and inflammatory markers: an intervention study based on resistance training and nutritional advice. Biomed Res Int 2021;2021:6681823.ArticlePubMedPMCPDF
- 40. Hariharan R, Odjidja EN, Scott D, Shivappa N, Hebert JR, Hodge A, et al. The dietary inflammatory index, obesity, type 2 diabetes, and cardiovascular risk factors and diseases. Obes Rev 2022;23:e13349.ArticlePubMedPDF
- 41. Wawrzyniak-Gramacka E, Hertmanowska N, Tylutka A, Morawin B, Wacka E, Gutowicz M, et al. The association of anti-inflammatory diet ingredients and lifestyle exercise with inflammaging. Nutrients 2021;13:3696.ArticlePubMedPMC
- 42. Anusruti A, Xuan Y, Gao X, Jansen E, Laetsch DC, Brenner H, et al. Factors associated with high oxidative stress in patients with type 2 diabetes: a meta-analysis of two cohort studies. BMJ Open Diabetes Res Care 2020;8:e000933.ArticlePubMedPMC
- 43. Tahrani AA, Barnett AH, Bailey CJ. Pharmacology and therapeutic implications of current drugs for type 2 diabetes mellitus. Nat Rev Endocrinol 2016;12:566-92.ArticlePubMedPDF
- 44. Chen CN, Chen TC, Tsai SC, Hwu CM. Factors associated with relative muscle strength in patients with type 2 diabetes mellitus. Arch Gerontol Geriatr 2021;95:104384.ArticlePubMed
- 45. You T, Arsenis NC, Disanzo BL, Lamonte MJ. Effects of exercise training on chronic inflammation in obesity: current evidence and potential mechanisms. Sports Med 2013;43:243-56.ArticlePubMedPDF
- 46. Gippini A, Mato A, Pazos R, Suarez B, Vila B, Gayoso P, et al. Effect of long-term strength training on glucose metabolism. Implications for individual impact of high lean mass and high fat mass on relationship between BMI and insulin sensitivity. J Endocrinol Invest 2002;25:520-5.ArticlePubMedPDF
- 47. Richter-Stretton GL, Fenning AS, Vella RK. Skeletal muscle: a bystander or influencer of metabolic syndrome? Diabetes Metab Syndr 2020;14:867-75.ArticlePubMed
- 48. Franceschi C, Campisi J. Chronic inflammation (inflammaging) and its potential contribution to age-associated diseases. J Gerontol A Biol Sci Med Sci 2014;69 Suppl 1:S4-9.ArticlePubMed
REFERENCES
Appendix
Appendix 1.
| Section and Topic | Item # | Checklist item | Location where item is reported | |
|---|---|---|---|---|
| TITLE | ||||
| Title | 1 | Identify the report as a systematic review. | 1, title | |
| ABSTRACT | ||||
| Abstract | 2 | See the PRISMA 2020 for Abstracts checklist. | 2 | |
| INTRODUCTION | ||||
| Rationale | 3 | Describe the rationale for the review in the context of existing knowledge. | 3 | |
| Objectives | 4 | Provide an explicit statement of the objective(s) or question(s) the review addresses. | 3-4 | |
| METHODS | ||||
| Eligibility criteria | 5 | Specify the inclusion and exclusion criteria for the review and how studies were grouped for the syntheses. | 4-5 | |
| Information sources | 6 | Specify all databases, registers, websites, organisations, reference lists and other sources searched or consulted to identify studies. Specify the date when each source was last searched or consulted. | 4, Supplementary Table 1 | |
| Search strategy | 7 | Present the full search strategies for all databases, registers and websites, including any filters and limits used. | Supplementary Table 1 | |
| Selection process | 8 | Specify the methods used to decide whether a study met the inclusion criteria of the review, including how many reviewers screened each record and each report retrieved, whether they worked independently, and if applicable, details of automation tools used in the process. | 4-5 | |
| Data collection process | 9 | Specify the methods used to collect data from reports, including how many reviewers collected data from each report, whether they worked independently, any processes for obtaining or confirming data from study investigators, and if applicable, details of automation tools used in the process. | 5-6 | |
| Data items | 10a | List and define all outcomes for which data were sought. Specify whether all results that were compatible with each outcome domain in each study were sought (e.g., for all measures, time points, analyses), and if not, the methods used to decide which results to collect. | 4, 6 | |
| 10b | List and define all other variables for which data were sought (e.g., participant and intervention characteristics, funding sources). Describe any assumptions made about any missing or unclear information. | 4, 6 | ||
| Study risk of bias assessment | 11 | Specify the methods used to assess risk of bias in the included studies, including details of the tool(s) used, how many reviewers assessed each study and whether they worked independently, and if applicable, details of automation tools used in the process. | 5 | |
| Effect measures | 12 | Specify for each outcome the effect measure(s) (e.g., risk ratio, mean difference) used in the synthesis or presentation of results. | 6 | |
| Synthesis methods | 13a | Describe the processes used to decide which studies were eligible for each synthesis (e.g., tabulating the study intervention characteristics and comparing against the planned groups for each synthesis (item #5)). | 6 | |
| 13b | Describe any methods required to prepare the data for presentation or synthesis, such as handling of missing summary statistics, or data conversions. | 6 | ||
| 13c | Describe any methods used to tabulate or visually display results of individual studies and syntheses. | 6 | ||
| 13d | Describe any methods used to synthesize results and provide a rationale for the choice(s). If meta-analysis was performed, describe the model(s), method(s) to identify the presence and extent of statistical heterogeneity, and software package(s) used. | 6 | ||
| 13e | Describe any methods used to explore possible causes of heterogeneity among study results (e.g. subgroup analysis, meta-regression). | 6 | ||
| 13f | Describe any sensitivity analyses conducted to assess robustness of the synthesized results. | 6 | ||
| Reporting bias assessment | 14 | Describe any methods used to assess risk of bias due to missing results in a synthesis (arising from reporting biases). | NA | |
| Certainty assessment | 15 | Describe any methods used to assess certainty (or confidence) in the body of evidence for an outcome. | 5-6 | |
| RESULTS | ||||
| Study selection | 16a | Describe the results of the search and selection process, from the number of records identified in the search to the number of studies included in the review, ideally using a flow diagram. | 7, Fig. 1 | |
| 16b | Cite studies that might appear to meet the inclusion criteria, but which were excluded, and explain why they were excluded. | Supplementary Table 2 | ||
| Study characteristics | 17 | Cite each included study and present its characteristics. | 7, 8, Table 1 | |
| Risk of bias in studies | 18 | Present assessments of risk of bias for each included study. | 8, Supplementary material | |
| Results of individual studies | 19 | For all outcomes, present, for each study: (a) summary statistics for each group (where appropriate) and (b) an effect estimate and its precision (e.g., confidence/credible interval), ideally using structured tables or plots. | 8, 9, Figs. 2, 3 | |
| Results of syntheses | 20a | For each synthesis, briefly summarise the characteristics and risk of bias among contributing studies. | 8, 9, Supplementary material | |
| 20b | Present results of all statistical syntheses conducted. If meta-analysis was done, present for each the summary estimate and its precision (e.g., confidence/credible interval) and measures of statistical heterogeneity. If comparing groups, describe the direction of the effect. | Figs. 2, 3 | ||
| 20c | Present results of all investigations of possible causes of heterogeneity among study results. | 9, Supplementary material | ||
| 20d | Present results of all sensitivity analyses conducted to assess the robustness of the synthesized results. | Supplementary material | ||
| Reporting biases | 21 | Present assessments of risk of bias due to missing results (arising from reporting biases) for each synthesis assessed. | NA | |
| Certainty of evidence | 22 | Present assessments of certainty (or confidence) in the body of evidence for each outcome assessed. | Supplementary Table 3 | |
| DISCUSSION | ||||
| Discussion | 23a | Provide a general interpretation of the results in the context of other evidence. | 9 | |
| 23b | Discuss any limitations of the evidence included in the review. | 10-11 | ||
| 23c | Discuss any limitations of the review processes used. | 11 | ||
| 23d | Discuss implications of the results for practice, policy, and future research. | 9-11 | ||
| OTHER INFORMATION | ||||
| Registration and protocol | 24a | Provide registration information for the review, including register name and registration number, or state that the review was not registered. | Title, 2 | |
| 24b | Indicate where the review protocol can be accessed, or state that a protocol was not prepared. | 2 (PROSPERO register) | ||
| 24c | Describe and explain any amendments to information provided at registration or in the protocol. | NA | ||
| Support | 25 | Describe sources of financial or non-financial support for the review, and the role of the funders or sponsors in the review. | Title | |
| Competing interests | 26 | Declare any competing interests of review authors. | Title | |
| A vailability of data, code and other materials | 27 | Report which of the following are publicly available and where they can be found: template data collection forms; data extracted from included studies; data used for all analyses; analytic code; any other materials used in the review. | NR | |
Figure & Data
References
Citations
- Körperliche Aktivität und Trainingstherapie bei Typ-2-Diabetes – ein Update
Andreas M. Nieß, Ansgar Thiel
Diabetologie und Stoffwechsel.2024; 19(01): 38. CrossRef - Genetic predisposition, lifestyle inflammation score, food-based dietary inflammatory index, and the risk for incident diabetes: Findings from the KoGES data
Hye Ah Lee, Hyesook Park, Bomi Park
Nutrition, Metabolism and Cardiovascular Diseases.2024; 34(3): 642. CrossRef - Associations of meeting 24-h movement guidelines and metabolic syndrome in Korean adults during the COVID-19 pandemic
S.W. Shin, Y. Choi, Y.H. Kang, J. Kim
Public Health.2024; 227: 187. CrossRef - Association of hypoglycemic events with cognitive impairment in patients with type 2 diabetes mellitus: Protocol for a dose-response meta-analysis
Min Ye, Ai Hong Yuan, Qi Qi Yang, Qun Wei Li, Fei Yue Li, Yan Wei, Muhammad Shahzad Aslam
PLOS ONE.2024; 19(2): e0296662. CrossRef - Exercise Interventions for the Prevention and Treatment of Anthracycline-Induced Cardiotoxicity in Women with Breast Cancer: A Systematic Review
Hongmei Li, Haiyun Liu, Boliang Wang, Xiao Jia, Jingjing Yu, Yurong Zhang, Die Sang, Yimin Zhang
Journal of Science in Sport and Exercise.2024;[Epub] CrossRef - Additive impact of diabetes and sarcopenia on all-cause and cardiovascular mortality: A longitudinal nationwide population-based study
Eyun Song, Soon Young Hwang, Min Jeong Park, Ahreum Jang, Kyeong Jin Kim, Ji Hee Yu, Nam Hoon Kim, Hye Jin Yoo, Ji A. Seo, Sin Gon Kim, Nan Hee Kim, Sei Hyun Baik, Kyung Mook Choi
Metabolism.2023; 148: 155678. CrossRef - Endothelial progenitor cell response to a multicomponent exercise training program in adults with cardiovascular risk factors
Suiane Cavalcante, Manuel Teixeira, Marisol Gouveia, Ana Duarte, Miriam Ferreira, Maria I. Simões, Maria Conceição, Mariana Costa, Ilda P. Ribeiro, Ana Cristina Gonçalves, José Oliveira, Fernando Ribeiro
German Journal of Exercise and Sport Research.2023; 53(2): 225. CrossRef - “Does Physical Exercise Promote Health Benefits for Diabetic Patients during the COVID-19 Pandemic?”: A Systematic Review
Erivaldo de Souza, Daniela Meneses-Santos, Josué Cruz Santos, Felipe J. Aidar, Carla Roberta de Oliveira Carvalho, Jymmys Lopes dos Santos, Anderson Carlos Marçal
Sports.2023; 11(10): 192. CrossRef - Effect of exercise on inflammatory markers in postmenopausal women with overweight and obesity: A systematic review and meta-analysis
Liang Tan, Weihua Yan, Weilin Yang, Agata Kamionka, Mariusz Lipowski, Zijian Zhao, Gang Zhao
Experimental Gerontology.2023; 183: 112310. CrossRef - Resistance Training Improves Beta Cell Glucose Sensing and Survival in Diabetic Models
Gabriela Alves Bronczek, Gabriela Moreira Soares, Carine Marmentini, Antonio Carlos Boschero, José Maria Costa-Júnior
International Journal of Molecular Sciences.2022; 23(16): 9427. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite- Figure
-



- Related articles
-
- Comparative Effect of Glucose-Lowering Drugs for Type 2 Diabetes Mellitus on Stroke Prevention: A Systematic Review and Network Meta-Analysis
- The Beneficial Effect of Glycemic Control against Adverse Outcomes in Patients with Type 2 Diabetes Mellitus and Chronic Kidney Disease
- Clinical Effects of a Home Care Pilot Program for Patients with Type 1 Diabetes Mellitus: A Retrospective Cohort Study
- Safety of COVID-19 Vaccines among Patients with Type 2 Diabetes Mellitus: Real-World Data Analysis
- Efficacy and Safety of Enavogliflozin versus Dapagliflozin as Add-on to Metformin in Patients with Type 2 Diabetes Mellitus: A 24-Week, Double-Blind, Randomized Trial



