
- Current
- Browse
- Collections
-
For contributors
- For Authors
- Instructions to authors
- Article processing charge
- e-submission
- For Reviewers
- Instructions for reviewers
- How to become a reviewer
- Best reviewers
- For Readers
- Readership
- Subscription
- Permission guidelines
- About
- Editorial policy
Articles
- Page Path
- HOME > Diabetes Metab J > Volume 48(2); 2024 > Article
-
Original ArticleComplications Risk of Depression according to Cumulative Exposure to a Low-Household Income Status in Individuals with Type 2 Diabetes Mellitus: A Nationwide Population- Based Study
-
So Hee Park1*
 , You-Bin Lee1*, Kyu-na Lee2, Bongsung Kim3, So Hyun Cho4, So Yoon Kwon1, Jiyun Park5, Gyuri Kim1, Sang-Man Jin1, Kyu Yeon Hur1, Kyungdo Han3, Jae Hyeon Kim1,6
, You-Bin Lee1*, Kyu-na Lee2, Bongsung Kim3, So Hyun Cho4, So Yoon Kwon1, Jiyun Park5, Gyuri Kim1, Sang-Man Jin1, Kyu Yeon Hur1, Kyungdo Han3, Jae Hyeon Kim1,6 -
Diabetes & Metabolism Journal 2024;48(2):290-301.
DOI: https://doi.org/10.4093/dmj.2022.0299
Published online: January 3, 2024
- 951 Views
- 142 Download
1Division of Endocrinology and Metabolism, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
2Department of Biomedicine & Health Sciences, College of Medicine, The Catholic University of Korea, Seoul, Korea
3Department of Statistics and Actuarial Science, Soongsil University, Seoul, Korea
4Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
5Division of Endocrinology and Metabolism, Department of Internal Medicine, CHA Bundang Medical Center, CHA University School of Medicine, Seongnam, Korea
6Department of Clinical Research Design and Evaluation, Samsung Advanced Institute for Health Sciences & Technology, Sungkyunkwan University, Seoul, Korea
- Corresponding authors: Jae Hyeon Kim https://orcid.org/0000-0001-5001-963X Division of Endocrinology and Metabolism, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, 81 Irwon-ro, Gangnam-gu, Seoul 06351, Korea E-mail: jaehyeon@skku.edu
-
Kyungdo Han Department of Statistics and Actuarial Science, Soongsil University, 369 Sangdo-ro, Dongjak-gu, Seoul 06978, Korea E-mail: hkd917@naver.com
- *So Hee Park and You-Bin Lee contributed equally to this study as first authors.
Copyright © 2024 Korean Diabetes Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Background
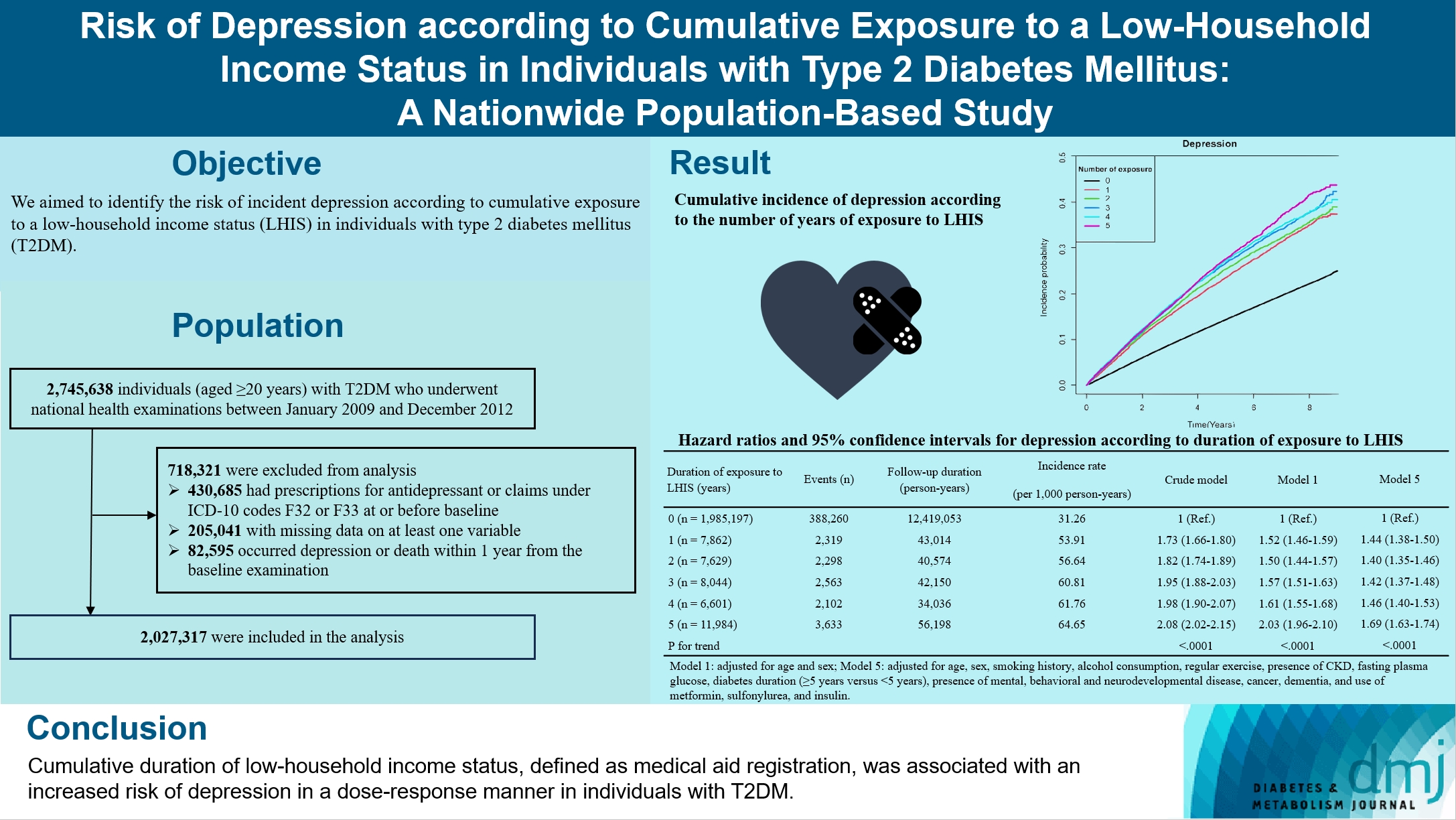
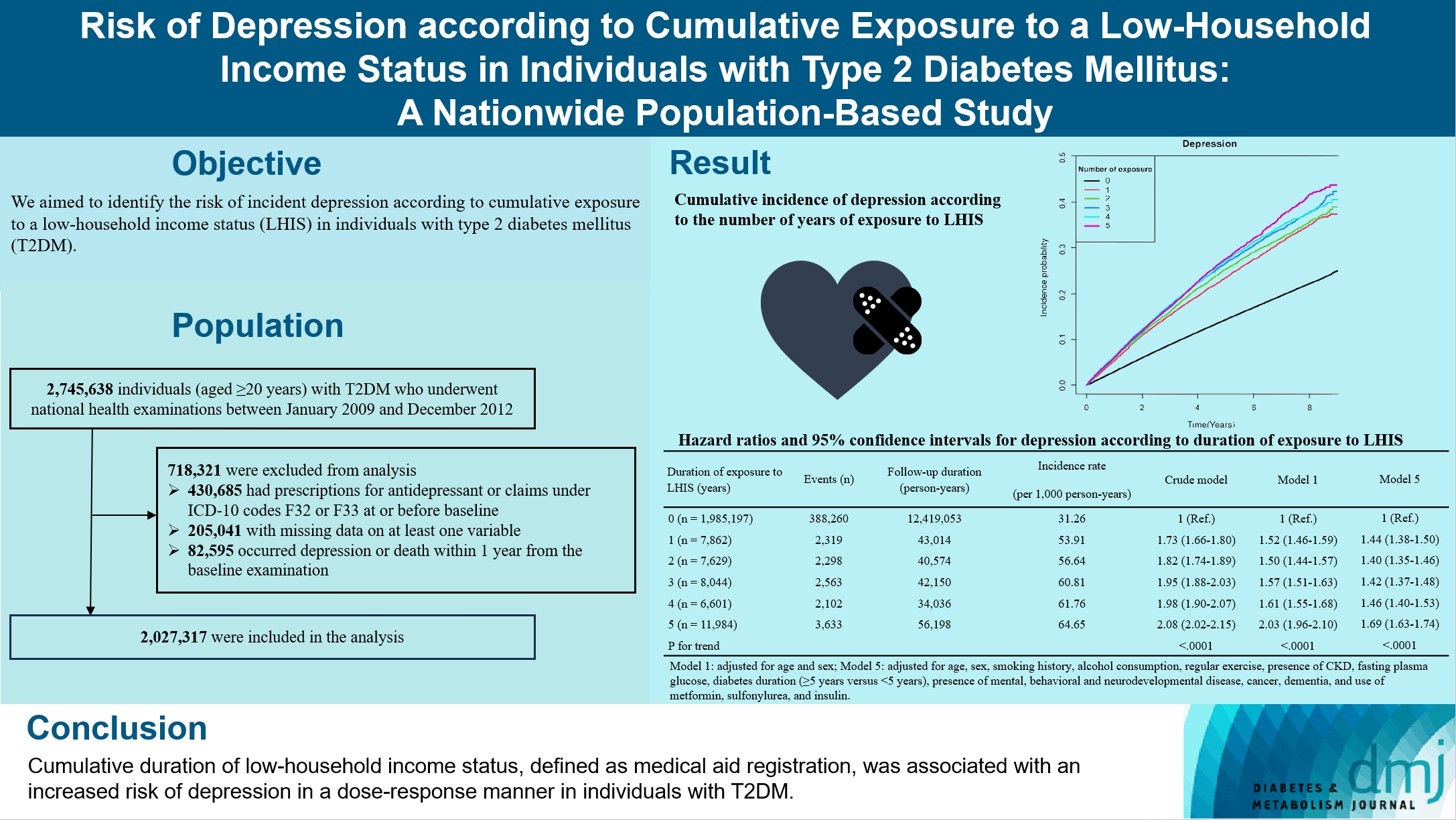
- We aimed to identify the risk of incident depression according to cumulative exposure to a low-household income status in individuals with type 2 diabetes mellitus (T2DM).
-
Methods
- For this retrospective longitudinal population-based cohort study, we used Korean National Health Insurance Service data from 2002 to 2018. Risk of depression was assessed according to cumulative exposure to low-household income status (defined as Medical Aid registration) during the previous 5 years among adults (aged ≥20 years) with T2DM and without baseline depression who underwent health examinations from 2009 to 2012 (n=2,027,317).
-
Results
- During an average 6.23 years of follow-up, 401,175 incident depression cases occurred. Advance in cumulative number of years registered for medical aid during the previous 5 years from baseline was associated with an increased risk of depression in a dose-dependent manner (hazard ratio [HR], 1.44 [95% confidence interval (CI), 1.38 to 1.50]; HR, 1.40 [95% CI, 1.35 to 1.46]; HR, 1.42, [95% CI, 1.37 to 1.48]; HR, 1.46, [95% CI, 1.40 to 1.53]; HR, 1.69, [95% CI, 1.63 to 1.74] in groups with 1 to 5 exposed years, respectively). Insulin users exposed for 5 years to a low-household income state had the highest risk of depression among groups categorized by insulin use and duration of low-household income status.
-
Conclusion
- Cumulative duration of low-household income status, defined as medical aid registration, was associated with an increased risk of depression in a dose-response manner in individuals with T2DM.
- • This is a nationwide, longitudinal, population-based study in adults with T2DM.
- • Low income was associated with depression risk in this group.
- • Duration of low-income states showed a dose-response relation to depression risk.
- • Insulin users in low-income states are particularly susceptible to depression.
Highlights
- Major depression is a severe recurrent disorder associated with reduced role functioning and quality of life, medical morbidity, and mortality [1]. In individuals with type 2 diabetes mellitus (T2DM), the prevalence of depression has been estimated to be almost double that in individuals without diabetes [2,3]. Furthermore, increased risks of psychiatric disorders, including depression and suicide attempts, have been reported in emerging adults with diabetes [4]. In people with diabetes, presence of depression has been associated with decreased quality of life, poor glycemic control, and higher risk of diabetes-related complications [5]. Therefore, for appropriate management of diabetes, it is necessary to identify risk factors for depression and provide preventive measures to susceptible populations [6].
- Association between socioeconomic status (SES), including income, and depression is controversial, but in a meta-analysis of 51 studies, individuals with a low level of education or low income had a higher risk of depression [7]. The occurrence of depression has been associated with lower SES including income, even in individuals with diabetes [8]. However, most studies of the relationships between depression and income in people with diabetes used only cross-sectional data and prevalence instead of incidence to evaluate associations with depression [6,9-11]. These previous studies could therefore not clarify if there is a temporal relationship between exposure and outcome, and income status was only considered at a single time point. Therefore, the risk of incident depression in people with T2DM needs to be evaluated according to cumulative duration of exposure to a low-household income status in a representative cohort with repeated evaluation of household income and longer follow-up using a longitudinal study design.
- Moreover, the requirement for insulin treatment might also affect the risk of depression among people with T2DM. More demanding diabetes care and increased responsibility of patients and their caregivers for treatment decisions associated with insulin treatment could theoretically increase psychological burden in patients with diabetes [12]. Also, requiring insulin treatment may reflect a more advanced disease in people with T2DM in the real world, which might be associated with increased risk of depression. A meta-analysis by Bai et al. [13] showed that patients with T2DM treated with insulin had more depressive syndromes than those who did not receive insulin therap.
- Therefore, we aimed to identify the risk of incident depression according to cumulative exposure to low-household income status (defined as medical aid registration) in individuals with T2DM. The incidence of depression was also investigated according to groups categorized by cumulative exposure to low-household income status and the use of insulin to explore the combined effects of these two factors.
INTRODUCTION
- Data sources
- We used Korean National Health Insurance Service (KNHIS) data from January 2002 to December 2018. KNHIS is the single nationwide insurance provider controlled by the Korean government. It includes the entire population of Korea and comprises two major health care programs: National Health Insurance (NHI) and Medical Aid (MA) [14]. Approximately 97% of the population are covered by NHI, and the remaining 3% of the population with the lowest income are covered by MA [14]. From these anonymized KNHIS data, demographics, monthly household income, date of death, primary and secondary diagnoses classified by the International Classification of Diseases-10th Revision (ICD-10), prescriptions, procedures, and dates of hospital visits and hospitalizations for all Korean residents are available. Furthermore, the KNHIS recommends standardized health examinations at least every 2 years for its enrollees. The results of these examinations are compiled into preventive health screening datasets. These health examination results include smoking history, alcohol consumption, physical activity, anthropometric measurements such as height, weight, and waist circumference, blood pressure, and laboratory information, including lipid profiles, fasting plasma glucose level, and estimated glomerular filtration rate.
- The Institutional Review Board (IRB) of Soongsil University approved this study (file number: SSU-202003-HR-201-01). An informed consent exemption was granted by the IRB because the researchers were provided anonymous, de-identified data from the KNHIS.
- Study cohort, outcomes, and follow-up
- In this retrospective, longitudinal, population-based cohort study, we included adults aged ≥20 years with T2DM who underwent at least one health examination between 2009 and 2012. T2DM was defined as having ≥one claim per year for the prescription of oral anti-diabetic medication under ICD-10 codes E11–14 or having a fasting plasma glucose level ≥126mg/dL, as in previous studies [15-17]. The time point of the last examination between 2009 and 2012 was considered to be the baseline. Individuals with missing data for at least one variable and those who had prescriptions for antidepressant or claims under ICD-10 codes F32–33 at or before baseline were excluded.
- The primary endpoint of this study was newly diagnosed depression that was defined as a patient being diagnosed by a psychiatrist with a specific ICD-10 code (F32 [major depressive disorder, single episode] or F33 [major depressive disorder, recurrent]) [18]. The study population was followed from baseline until the date of death, onset of depression, or December 31, 2018, whichever came first.
- Exposure to low-household income
- Every year, the KNHIS evaluates the household income status of all registrants and decides whether to register for MA for the lowest income individuals (the lowest 3%). MA beneficiaries for a given year were considered to have been exposed to low-household income status. Individuals in the current study were categorized into six groups according to the number of years registered to MA beneficiaries during the 5 years prior to baseline (from 0 to 5 years).
- Measurements and definitions
- Questionnaires were used to collect information on smoking history, alcohol consumption, and regular exercise. Definition of heavy alcohol consumption [19], regular exercise [20], body mass index (BMI), hypertension [21], dyslipidemia [21], chronic kidney disease (CKD) [22], insulin use [23], and dementia [24] are summarized in Supplementary Table 1. Mental, behavioral, and neurodevelopmental disease and cancer were defined based on the corresponding ICD-10 diagnostic codes (Supplementary Table 1). The unawareness of diabetes was defined as having a fasting plasma glucose level ≥126mg/dL and having no claim for the prescription of oral anti-diabetic medication under ICD-10 codes E11–14. Lipid-lowering agents included statins, ezetimibe, and fibrates [25]. Blood tests, including plasma glucose and lipid profiles, were performed using intravenous samples collected after an overnight fast.
- Statistical analysis
- We used SAS software version 9.3 (SAS Institute, Cary, NC, USA) for statistical analyses. Baseline characteristics of the study population were assessed in six groups stratified by number of years exposed to a low-household income status during the 5 years prior to baseline. Continuous variables with normal distributions are presented as means±standard deviations and categorical data are presented as frequencies and percentages.
- Incidence rate of depression was derived from the number of incident cases divided by the total follow-up duration (person-years). Kaplan-Meier curves were used to compare the cumulative incidence of depression according to duration of exposure to low-household income status in the six groups; the significance of differences among the six groups was evaluated using the log-rank test. Multivariable Cox regression analysis was performed to calculate hazard ratios (HRs) and 95% confidence intervals (CIs) for outcome incidence rates according to duration of exposure to low-household income status: unadjusted in model 1, adjusted for age and sex in model 2, adjusted for age, sex, smoking history, alcohol consumption, regular exercise, and presence of CKD in model 3, additionally adjusted for fasting plasma glucose level, and diabetes duration (≥5 years vs. <5 years) in model 4, and additionally adjusted for presence of mental, behavioral and neurodevelopmental disease, cancer, dementia, and use of metformin (MFM), sulfonylurea (SU), and insulin in model 5. In constructing these regression models, various risk factors for depression identified in previous studies were included as potential confounders [26,27].
- HRs (95% CIs) for outcome incidence rates in participants with 1 or more years of exposure to low-household income status were compared with those with no exposure (reference) in subgroups classified by age (<65 years vs. ≥65 years), sex, current smoking, heavy alcohol consumption, regular exercise, presence of obesity (defied as a BMI ≥25 kg/m2 referring to obesity guidelines for the Korean population [28]), use of insulin, whether taking three or more oral anti-diabetic agents or not, diabetes duration (≥5 years vs. <5 years), the awareness of diabetes, fasting plasma glucose level (<140 mg/dL vs. ≥140 mg/dL), and the type of oral anti-diabetic agents. We evaluated the potential effect modification by these factors determining the subgroups and calculated P values for interactions.
- To explore the potential effect modification by insulin use more thoroughly, HRs and 95% CIs for outcome incidence rates according to duration of exposure to low-household income status were calculated after stratifying the study population-based on insulin use, and P values for interactions were calculated. The study population was also divided into 12 groups according to insulin use and exposure duration to lowhousehold income status during the 5 years prior to baseline. To assess the combined effects of insulin use and cumulative exposure to low-household income status, HRs (95% CIs) for outcome incidence rates according to these 12 groups were calculated.
- Sensitivity analyses
- Sensitivity analysis was performed by excluding individuals who developed depression within 2 years after baseline.
METHODS
- Baseline characteristics of the study population
- The study participants comprised a total of 2,027,317 adults (aged ≥20 years) with T2DM (Supplementary Fig. 1). Among them, 1,985,197 (97.92%) were never exposed to a low-household income state during the 5 years prior to baseline. The remaining 42,120 (2.08%) were exposed to a low-household income state for at least 1 year during the 5 years prior to baseline. Baseline characteristics are presented according to years exposed to a low-household income state (Table 1). Participants with a longer exposure to a low-household income status were more likely to have a higher prevalence of dyslipidemia, mental, behavioral, and neurodevelopmental disease, a higher proportion of insulin use, use of three or more oral anti-diabetic agents, MFM, dipeptidyl peptidase-4 inhibitor, lipid-lowering agents, longer-standing diabetes (diabetes duration ≥5 years), and be non-drinkers. In addition, this population was characterized by a lower proportion of the unawareness of diabetes in conjunction with a higher proportion of use of three or more oral anti-diabetic agents and decreasing trends in total and low-density lipoprotein cholesterol in conjunction with the use of lipid-lowering agents for dyslipidemia.
- Risk of incident depression according to duration of exposure to a low-household income status
- During the median 6.77 years of follow-up (12,635,025.87 person-years), 401,175 incident depression cases occurred. Cumulative incidence of depression according to duration of exposure to a low-household income state was expressed in the form of Kaplan-Meier curves (Fig. 1). When individuals who had never been exposed to a low-household income status were set as a reference, an increase in cumulative duration of exposure to a low-household income state during the 5 years prior to baseline was associated with an increased risk of depression in a dose-dependent manner (HR, 1.44 [95% CI, 1.38 to 1.50]; HR, 1.40 [95% CI, 1.35 to 1.46]; HR, 1.42 [95% CI, 1.37 to 1.48]; HR, 1.46 [95% CI, 1.40 to 1.53]; HR, 1.69 [95% CI, 1.63 to 1.74] in groups with 1 to 5 years of exposure, respectively, in the fully-adjusted model 5) (Table 2).
- Subgroup analysis
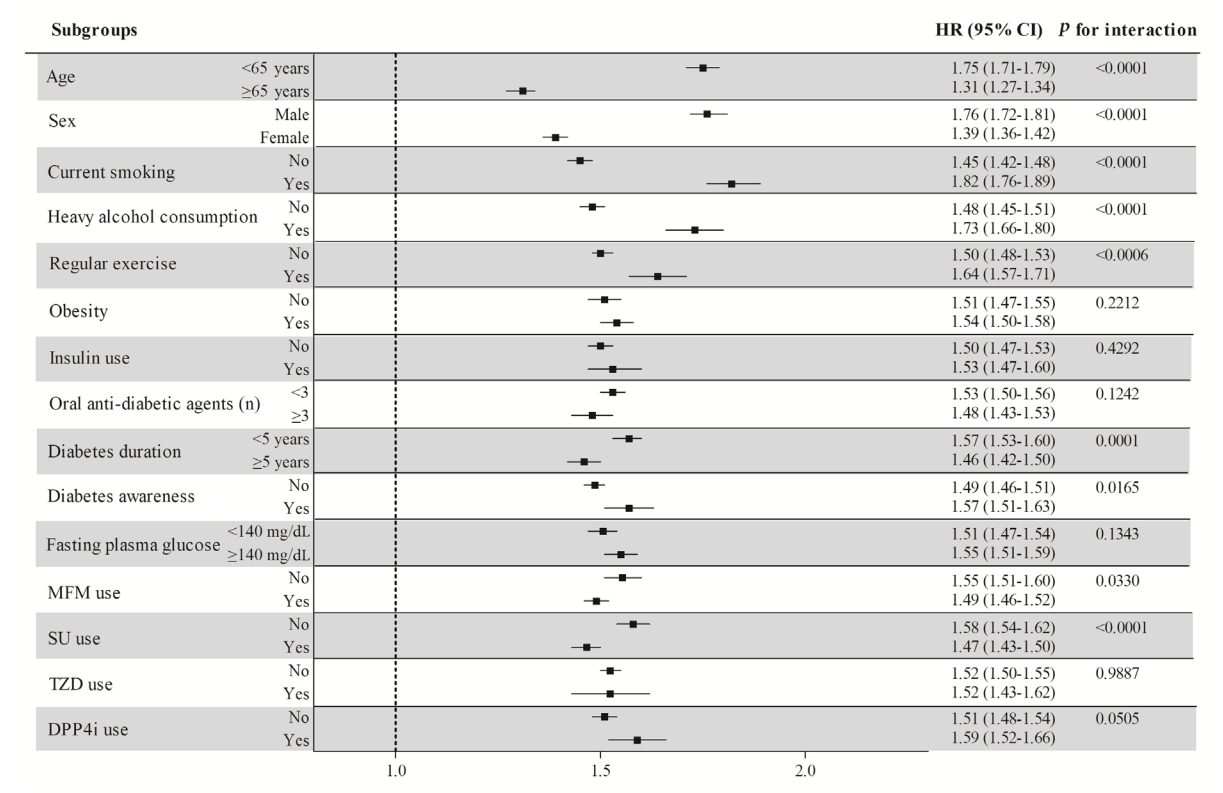
- HRs (95% CIs) for depression in participants with at least one exposure to a low-household income status were calculated in subgroups stratified by age (<65 years vs. ≥65 years), sex, current smoking, heavy alcohol consumption, regular exercise, obesity, insulin use, use of three or more oral anti-diabetic agents, diabetes duration (≥5 years vs. <5 years), the awareness of diabetes, fasting plasma glucose level (<140 mg/dL vs. ≥140 mg/dL), and the type of oral anti-diabetic agents, and compared with those of participants with no exposure to these conditions (Table 3, Fig. 2). Participants in all subgroups with at least 1 year of exposure to a low-household income status had a higher risk of depression than those without exposure. These associations were more prominent in people younger than 65 years of age, males, current smokers, heavy alcohol consumers, SU non-users (P for interaction <0.0001 for all of the above), and those with a diabetes duration of less than 5 years (P for interaction=0.0001).
- Stratified analyses according to insulin use
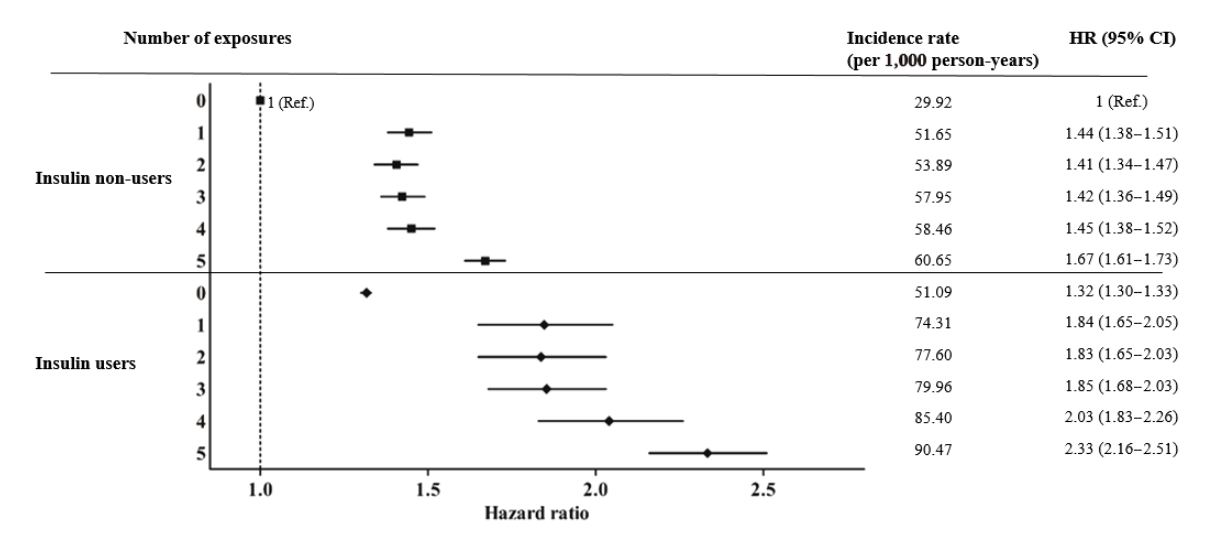
- After dividing study subjects into insulin users and insulin non-users, the HRs (95% CIs) of depression were analyzed according to duration of low-household income status (Supplementary Table 2). Regardless of insulin use, HRs were higher among those exposed to a low-household income status than those without exposure. Except for unadjusted model 1, other models demonstrated no significant effect modifications by insulin use (P for interaction 0.6320 in model 5). When we calculated the hazards of depression in 12 groups categorized by insulin use and years exposed to a low-household income state, HRs were the highest in insulin users with 5 years of exposure to a low-household income state (HR, 2.33; 95% CI, 2.16 to 2.51), followed by insulin users with 1 to 4 years of exposure compared to insulin non-users without exposure (reference) (Fig. 3). Insulin users without exposure to a low-household income state (HR, 1.32; 95% CI, 1.30 to 1.33) and insulin non-users with one year of exposure (HR, 1.44; 95% CI, 1.38 to 1.51) also had higher hazards of the primary outcome than the reference group.
- Sensitivity analyses
- Exclusion of individuals who developed depression within 2 years of baseline resulted in findings consistent with the main results (Supplementary Table 3).
RESULTS
- This large-scale longitudinal study involving 2,027,317 adults with T2DM revealed a dose-response relationship between cumulative exposure to a low-household income state and the incidence of newly diagnosed depression. This result was consistent even after adjusting for potential confounders including demographic and lifestyle factors as well as category of diabetes duration, presence of mental, behavioral and neurodevelopmental disease, cancer, dementia, and use of MFM, SU, and insulin. Furthermore, consistent results were obtained in subgroup analyses after stratification by age, sex, current smoking, heavy alcohol consumption, regular exercise, presence of obesity, insulin use, taking three or more oral anti-diabetic agents, diabetes duration (≥5 years vs. <5 years), the awareness of diabetes, fasting glucose level, and the type of oral anti-diabetic agents. When study subjects were classified according to insulin use and duration of exposure to a low-household income state, insulin users with the most sustained exposure to a low-household income state had the highest risk of developing depression.
- Previous studies have also suggested an association between low-household income and depression in adults with diabetes [6,11,29]. However, most of these previous studies were small cross-sectional studies that investigated the prevalence of depression in low-household income patient with diabetes [6,9-11]. In contrast to these cross-sectional studies, we performed a longitudinal study and demonstrated that the risk of incident depression in people with T2DM increased according to cumulative duration of exposure to a low-household income status. Our large-scale longitudinal study of the incidence of depression, rather than its prevalence, according to duration of exposure to a low-household income status in patients with T2DM allowed us to establish temporal relationship and demonstrate dose-response relationship between exposure and outcome.
- In subgroup analysis, participants with at least 1 year of exposure to a low-household income status had a higher risk of depression in all subgroups than those without low income exposure. However, the excess hazard of depression from exposure to a low-household income state among adults with T2DM was more prominent in those under 65 years of age, males, current smokers, heavy alcohol consumers, and those with a diabetes duration of less than 5 years, SU non-users. Although underlying mechanisms cannot be exactly clarified in the current study, there are several possible explanations for these findings. First, regarding more prominent associations among adults under 65 years, older adults appear to react less to stressors [30] and they might be more protective against depression than younger adults after experiencing stressful conditions [31]. Second, with respect to the interaction by sex, males may be more vulnerable to low income than females. Similarly, a study from Denmark suggested that SES proxied by low income, unskilled blue-collar work, non-specific wage work and unemployment, increased suicide risk more prominently for men than for women [32]. Third, current smoking and heavy drinking, both of which are maladaptive health behaviors, may cause cumulative biopsychosocial vulnerability [33], and chronic stress associated with low-household income might have greater effects on the mental health of current smokers and heavy alcohol consumers. Fourth, with respect to interaction by diabetes duration, individuals with a diabetes duration of less than 5 years may have been affected more vulnerably by low-household income in a state of high distress and anxiety after recent diagnosis of diabetes. In a previous study that found substantially higher risks of psychiatric disorders and suicide attempts in adolescents and emerging adults with diabetes compared to those without diabetes, excess risk was most prominent in those individuals recently diagnosed with diabetes (duration of ≤2 years), indicating the possibility of elevated psychological distress in individuals with a recent diagnosis of diabetes [4]. Similarly, another study found an increased risk of psychiatric disorders and suicide attempts in children and adolescents with type 1 diabetes mellitus (T1DM) compared with their healthy siblings, and the highest risk of psychiatric disorders was noted within the first 6 months after being diagnosed with T1DM and declined with time [12]. Finally, consistent to a previous study that reported an association between high dose of SU and higher risk of depression [34], SU users non-exposed to low-household income status in our study had a higher incidence rate of depression than SU non-users. Excess risk of depression from exposure to low-household income status in SU users might be relatively less than SU non-users.
- With regard to the baseline characteristic of the study subjects, the proportion of insulin use increased as duration of exposure to a low-household income state increased. Interestingly, at the same time, insulin users exposed to a low-household income state for the longest duration had the highest risk of incident depression. These results indicate that careful psychiatric evaluation and appropriate interventions to prevent and detect depression early should be provided to insulin users with low-household income. Severe depression unrecognized and untreated in individuals with diabetes is associated with lower adherence to medication, poor glycemic control, increased risk of complication, increased healthcare costs, and higher mortality rate [35]. Therefore, it is important that vulnerable individuals with diabetes in low-household income status, especially insulin users should be screened for depression, incorporating psychiatric healthcare for prevention and early detection of depression into diabetes care.
- The strengths of this study are as follows. This is the first large-scale longitudinal study (n=2,027,317) to report the incidence of depression according to exposure to a low-household income state in adults with T2DM. By examining exposure as cumulative duration of exposure to a low-household income state over 5 years and not simply cross-sectional income status at a single time point, we were able to demonstrate a dose-response relationship between exposure and risk of depression. We used a representative nationwide cohort database managed by the Korean government that contains diverse demographic information, claims data, lifestyle factors, and laboratory results for large, nationwide population of Korea, which enabled adjustment for various potential confounders. Furthermore, consistent results were obtained in sensitivity and subgroup analyses.
- This study also had several limitations. First, this was an observational study, making it inevitably impossible to determine causal relationships. However, at least, to maintain temporal relationship, those individuals who obtained prescriptions for antidepressants or had claims under depression codes at or before baseline were excluded. Furthermore, we examined duration of exposure to a low-household income state for the 5 years prior to baseline as opposed to after baseline. Second, even after adjusting for possible confounding factors, residual effects of unmeasured confounders may still have been present. For example, we could not adjust for glycated hemoglobin or other indicators of SES such as education because these factors were not available in the KNHIS dataset. Third, generalization of our findings to individuals with T1DM or those without diabetes or individuals of different ethnicities should be done with caution as we included only Korean adults with T2DM in this study.
- In conclusion, cumulative duration of exposure to a low-household income status, defined as medical aid registration, was associated with an increased risk of depression in a dosedependent manner in individuals with T2DM. The requirement for insulin treatment was associated with an additional increase in the risk of depression in conjunction with advanced duration of exposure to a low-household income state. In particular, insulin users with sustained exposure to a low-household income state were most susceptible to incident depression. These findings suggest that strategies to prevent and detect depression early, including psychiatric evaluation and monitoring systems, should be provided more intensively to individuals with T2DM and a low income status, especially those using insulin.
DISCUSSION
SUPPLEMENTARY MATERIALS
Supplementary Table 2.
Supplementary Table 3.
Supplementary Fig. 1.
-
CONFLICTS OF INTEREST
Sang-Man Jin has been associate editor of the Diabetes & Metabolism Journal since 2022. He was not involved in the review process of this article. Otherwise, there was no conflict of interest.
-
AUTHOR CONTRIBUTIONS
Conception or design: S.H.P., Y.B.L., K.H., J.H.K.
Acquisition, analysis, or interpretation of data: K.L., B.K., K.H.
Drafting the work or revising: S.H.P., Y.B.L., J.H.K.
Final approval of the manuscript: S.H.P., Y.B.L., K.L., B.K., S.H.C., S.Y.K., J.P., G.K., S.M.J., K.Y.H., K.H., J.H.K.
-
FUNDING
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT) (No. 2019R1I1A1A0106118813) to Prof. Kyungdo Han. The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
NOTES
-
Acknowledgements
- This work was performed using data from the Korean National Health Insurance Service (KNHIS). We used the National Health Information Database constructed by the KNHIS, and the study results do not necessarily represent the opinion of the KNHIS.

| Characteristic |
Duration of exposure to low-household income, yr |
|||||||
|---|---|---|---|---|---|---|---|---|
| 0 (n=1,985,197) | 1 (n=7,862) | 2 (n=7,629) | 3 (n=8,044) | 4 (n=6,601) | 5 (n=11,984) | P value | P for trend | |
| Age, yr | 56.3±12.33 | 58.15±13.3 | 59.63±13.37 | 60.13±12.67 | 59.79±12.58 | 56.31±8.96 | <0.0001 | <0.0001 |
| Male sex | 1,282,720 (64.61) | 3,906 (49.68) | 3,471 (45.5) | 3,563 (44.29) | 2,894 (43.84) | 5,860 (48.9) | <0.0001 | <0.0001 |
| Current smoker | 556,739 (28.04) | 2,128 (27.07) | 1,872 (24.54) | 1,920 (23.87) | 1,607 (24.34) | 3,331 (27.8) | <0.0001 | <0.0001 |
| Heavy alcohol consumption | 219,216 (11.04) | 651 (8.28) | 543 (7.12) | 560 (6.96) | 451 (6.83) | 840 (7.01) | <0.0001 | <0.0001 |
| Regular exercise | 415,454 (20.93) | 1,237 (15.73) | 1,207 (15.82) | 1,309 (16.27) | 1,080 (16.36) | 1,925 (16.06) | <0.0001 | <0.0001 |
| Body mass index, kg/m2 | 25.1±3.39 | 24.96±3.8 | 25±3.86 | 25.04±3.91 | 24.99±3.92 | 25.29±4.11 | <0.0001 | <0.0001 |
| Waist circumference, cm | 85.53±8.83 | 85±9.43 | 85.19±9.46 | 85.21±9.51 | 85.02±9.55 | 85.85±9.98 | <0.0001 | <0.0001 |
| Systolic BP, mm Hg | 129.22±15.79 | 128.95±16.76 | 128.94±16.53 | 128.87±16.71 | 128.59±16.63 | 126.91±16.53 | <0.0001 | <0.0001 |
| Diastolic BP, mm Hg | 79.34±10.29 | 78.79±10.5 | 78.65±10.33 | 78.57±10.38 | 78.38±10.5 | 77.95±10.4 | <0.0001 | <0.0001 |
| Fasting plasma glucose, mg/dL | 146.23±46.73 | 147.41±53.32 | 146.25±53.43 | 145.6±54.79 | 146.37±56.67 | 142.56±53.27 | <0.0001 | <0.0001 |
| Insulin usea | 140,139 (7.06) | 897 (11.41) | 1,008 (13.21) | 1,170 (14.55) | 921 (13.95) | 1,800 (15.02) | <0.0001 | <0.0001 |
| Diabetes duration ≥5 years | 565,984 (28.51) | 2,408 (30.63) | 2,604 (34.13) | 3,111 (38.67) | 2,359 (35.74) | 5,006 (41.77) | <0.0001 | <0.0001 |
| Diabetes unawareness | 848,952 (42.76) | 2,549 (32.42) | 2,270 (29.75) | 1,909 (23.73) | 1,495 (22.65) | 2,427 (20.25) | <0.0001 | <0.0001 |
| Oral anti-diabetic agents ≥3 | 266,013 (13.40) | 1,399 (17.79) | 1,458 (19.11) | 1,825 (22.69) | 1,548 (23.45) | 2,858 (23.85) | <0.0001 | <0.0001 |
| Type of oral anti-diabetic agents | ||||||||
| MFM | 895,859 (45.13) | 4,163 (52.95) | 4,233 (55.49) | 4,848 (60.27) | 4,038 (61.17) | 7,961 (66.43) | <0.0001 | <0.0001 |
| SU | 782,992 (39.44) | 3,744 (47.62) | 3,718 (48.74) | 4,434 (55.12) | 3,644 (55.20) | 6,210 (51.82) | <0.0001 | <0.0001 |
| TZD | 122,299 (6.16) | 519 (6.60) | 510 (6.69) | 624 (7.76) | 559 (8.47) | 853 (7.12) | <0.0001 | <0.0001 |
| DPP4i | 161,049 (8.11) | 776 (9.87) | 810 (10.62) | 1,008 (12.53) | 886 (13.42) | 2,397 (20.00) | <0.0001 | <0.0001 |
| Dyslipidemia | 785,882 (39.59) | 3,378 (42.97) | 3,329 (43.64) | 3,782 (47.02) | 3,191 (48.34) | 6,217 (51.88) | <0.0001 | <0.0001 |
| Lipid-lowering agents | 589,342 (29.69) | 2,678 (34.06) | 2,687 (35.22) | 3,178 (39.51) | 2,689 (40.74) | 5,519 (46.05) | <0.0001 | <0.0001 |
| Total cholesterol, mg/dL | 197.68±46.15 | 195.28±44.54 | 193.47±50.63 | 191.66±43.68 | 191.95±52.92 | 188.51±45.37 | <0.0001 | <0.0001 |
| HDL-C, mg/dL | 52.18±29.68 | 52.32±27.05 | 51.66±19.31 | 52.22±57.87 | 51.71±23.82 | 51.02±21.1 | 0.0005 | 0.0005 |
| LDL-C, mg/dL | 113.13±86.12 | 110.16±49.72 | 109.7±55.81 | 111±160.01 | 107.62±51.18 | 105.35±43.12 | <0.0001 | <0.0001 |
| eGFR, mL/min/1.73 m2 | 85.68±36.5 | 84.11±34.03 | 83.37±39.21 | 82.97±34.64 | 83.55±35.22 | 86.96±34.81 | <0.0001 | <0.0001 |
| CKD (eGFR <60 mL/min/1·73 m2) | 202,864 (10.22) | 1,183 (15.05) | 1,309 (17.16) | 1,345 (16.72) | 1,147 (17.38) | 1,624 (13.55) | <0.0001 | <0.0001 |
| Mental, behavioral and neurodevelopmental disease | 295,144 (14.87) | 1,925 (24.48) | 2,016 (26.43) | 2,359 (29.33) | 1,979 (29.98) | 4,561 (38.06) | <0.0001 | <0.0001 |
| Cancer | 92,747 (4.67) | 541 (6.88) | 499 (6.54) | 559 (6.95) | 412 (6.24) | 733 (6.12) | <0.0001 | <0.0001 |
| Dementia | 21,735 (1.09) | 190 (2.42) | 245 (3.21) | 272 (3.38) | 220 (3.33) | 383 (3.20) | <0.0001 | <0.0001 |
Values are presented as mean±standard deviation or number (%).
BP, blood pressure; MFM, metformin; SU, sulfonylurea; TZD, thiazolidinedione; DPP4i, dipeptidyl peptidase-4 inhibitor; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; eGFR, estimated glomerular filtration rate; CKD, chronic kidney disease.
a Insulin use: A total of three or more prescriptions of insulin in the outpatient setting, and at least one prescription of insulin per year.
Model 1: unadjusted; Model 2: adjusted for age and sex; Model 3: adjusted for age, sex, smoking history, alcohol consumption, regular exercise, and presence of chronic kidney disease (CKD); Model 4: adjusted for age, sex, smoking history, alcohol consumption, regular exercise, and presence of CKD, fasting plasma glucose, and diabetes duration (≥5 years vs. <5 years); Model 5: adjusted for age, sex, smoking history, alcohol consumption, regular exercise, and presence of CKD, fasting plasma glucose, diabetes duration (≥5 years vs. <5 years), presence of mental, behavioral and neurodevelopmental disease, cancer, dementia, and use of metformin, sulfonylurea, and insulin.
Adjusted for age, sex, smoking history, alcohol consumption, regular exercise, presence of chronic kidney disease, fasting plasma glucose, diabetes duration (≥5 years vs. <5 years), presence of mental, behavioral and neurodevelopmental disease, cancer, and dementia.
HR, hazard ratio; CI, confidence interval; MFM, metformin; SU, sulfonylurea; TZD, thiazolidinedione; DPP4i, dipeptidyl peptidase-4 inhibitor.
- 1. Spijker J, Graaf R, Bijl RV, Beekman AT, Ormel J, Nolen WA. Functional disability and depression in the general population: results from the Netherlands Mental Health Survey and Incidence Study (NEMESIS). Acta Psychiatr Scand 2004;110:208-14.ArticlePubMed
- 2. Anderson RJ, Freedland KE, Clouse RE, Lustman PJ. The prevalence of comorbid depression in adults with diabetes: a metaanalysis. Diabetes Care 2001;24:1069-78.PubMed
- 3. Roy T, Lloyd CE. Epidemiology of depression and diabetes: a systematic review. J Affect Disord 2012;142 Suppl:S8-21.ArticlePubMed
- 4. Robinson ME, Simard M, Larocque I, Shah J, Nakhla M, Rahme E. Risk of psychiatric disorders and suicide attempts in emerging adults with diabetes. Diabetes Care 2020;43:484-6.ArticlePubMedPDF
- 5. Ascher-Svanum H, Zagar A, Jiang D, Schuster D, Schmitt H, Dennehy EB, et al. Associations between glycemic control, depressed mood, clinical depression, and diabetes distress before and after insulin initiation: an exploratory, post hoc analysis. Diabetes Ther 2015;6:303-16.ArticlePubMedPMCPDF
- 6. Park CY, Kim SY, Gil JW, Park MH, Park JH, Kim Y. Depression among Korean adults with type 2 diabetes mellitus: Ansan-Community-Based Epidemiological Study. Osong Public Health Res Perspect 2015;6:224-32.ArticlePubMedPMC
- 7. Lorant V, Deliege D, Eaton W, Robert A, Philippot P, Ansseau M. Socioeconomic inequalities in depression: a meta-analysis. Am J Epidemiol 2003;157:98-112.ArticlePubMed
- 8. Leone T, Coast E, Narayanan S, de Graft Aikins A. Diabetes and depression comorbidity and socio-economic status in low and middle income countries (LMICs): a mapping of the evidence. Global Health 2012;8:39.ArticlePubMedPMC
- 9. Ell K, Katon W, Cabassa LJ, Xie B, Lee PJ, Kapetanovic S, et al. Depression and diabetes among low-income Hispanics: design elements of a socioculturally adapted collaborative care model randomized controlled trial. Int J Psychiatry Med 2009;39:113-32.ArticlePubMedPMCPDF
- 10. Tellez-Zenteno JF, Cardiel MH. Risk factors associated with depression in patients with type 2 diabetes mellitus. Arch Med Res 2002;33:53-60.ArticlePubMed
- 11. Egede LE, Zheng D. Independent factors associated with major depressive disorder in a national sample of individuals with diabetes. Diabetes Care 2003;26:104-11.ArticlePubMedPDF
- 12. Butwicka A, Frisen L, Almqvist C, Zethelius B, Lichtenstein P. Risks of psychiatric disorders and suicide attempts in children and adolescents with type 1 diabetes: a population-based cohort study. Diabetes Care 2015;38:453-9.ArticlePubMedPMCPDF
- 13. Bai X, Liu Z, Li Z, Yan D. The association between insulin therapy and depression in patients with type 2 diabetes mellitus: a meta-analysis. BMJ Open 2018;8:e020062.ArticlePubMedPMC
- 14. Lee YH, Han K, Ko SH, Ko KS, Lee KU; Taskforce Team of Diabetes Fact Sheet of the Korean Diabetes Association. Data analytic process of a nationwide population-based study using National Health Information Database established by National Health Insurance Service. Diabetes Metab J 2016;40:79-82.ArticlePubMedPMCPDF
- 15. Lee YB, Han K, Kim B, Lee SE, Jun JE, Ahn J, et al. Risk of early mortality and cardiovascular disease in type 1 diabetes: a comparison with type 2 diabetes, a nationwide study. Cardiovasc Diabetol 2019;18:157.ArticlePubMedPMCPDF
- 16. Lee YB, Han K, Kim B, Jin SM, Lee SE, Jun JE, et al. High proportion of adult cases and prevalence of metabolic syndrome in type 1 diabetes mellitus population in Korea: a nationwide study. Diabetes Metab J 2019;43:76-89.ArticlePubMedPMCPDF
- 17. Noh J, Han KD, Ko SH, Ko KS, Park CY. Trends in the pervasiveness of type 2 diabetes, impaired fasting glucose and comorbidities during an 8-year-follow-up of nationwide Korean population. Sci Rep 2017;7:46656.ArticlePubMedPMCPDF
- 18. Jin EH, Han K, Lee DH, Shin CM, Lim JH, Yoon H, et al. Increased risk of major depressive disorder after cholecystectomy: a nationwide population-based cohort study in Korea. Clin Transl Gastroenterol 2021;12:e00339.ArticlePubMedPMC
- 19. Stampfer MJ, Kang JH, Chen J, Cherry R, Grodstein F. Effects of moderate alcohol consumption on cognitive function in women. N Engl J Med 2005;352:245-53.ArticlePubMed
- 20. Lee YB, Kim DH, Kim SM, Kim NH, Choi KM, Baik SH, et al. Hospitalization for heart failure incidence according to the transition in metabolic health and obesity status: a nationwide population-based study. Cardiovasc Diabetol 2020;19:77.ArticlePubMedPMCPDF
- 21. Kim MK, Han K, Kim HS, Park YM, Kwon HS, Yoon KH, et al. Cholesterol variability and the risk of mortality, myocardial infarction, and stroke: a nationwide population-based study. Eur Heart J 2017;38:3560-6.ArticlePubMedPMC
- 22. Lee YB, Han K, Kim B, Jun JE, Lee SE, Ahn J, et al. Risk of endstage renal disease from chronic kidney disease defined by decreased glomerular filtration rate in type 1 diabetes: a comparison with type 2 diabetes and the effect of metabolic syndrome. Diabetes Metab Res Rev 2019;35:e3197.ArticlePubMedPDF
- 23. Lee YB, Han K, Kim B, Choi MS, Park J, Kim M, et al. Risk of early mortality and cardiovascular disease according to the presence of recently diagnosed diabetes and requirement for insulin treatment: a nationwide study. J Diabetes Investig 2021;12:1855-63.ArticlePubMedPMCPDF
- 24. Nam GE, Park YG, Han K, Kim MK, Koh ES, Kim ES, et al. BMI, weight change, and dementia risk in patients with newonset type 2 diabetes: a nationwide cohort study. Diabetes Care 2019;42:1217-24.ArticlePubMedPDF
- 25. Kim MK, Han K, Lee SH. Current trends of big data research using the Korean National Health Information Database. Diabetes Metab J 2022;46:552-63.ArticlePubMedPMCPDF
- 26. Katon W, von Korff M, Ciechanowski P, Russo J, Lin E, Simon G, et al. Behavioral and clinical factors associated with depression among individuals with diabetes. Diabetes Care 2004;27:914-20.ArticlePubMedPDF
- 27. Ali S, Stone MA, Peters JL, Davies MJ, Khunti K. The prevalence of co-morbid depression in adults with type 2 diabetes: a systematic review and meta-analysis. Diabet Med 2006;23:1165-73.ArticlePubMed
- 28. Kim MK, Lee WY, Kang JH, Kang JH, Kim BT, Kim SM, et al. 2014 Clinical practice guidelines for overweight and obesity in Korea. Endocrinol Metab (Seoul) 2014;29:405-9.ArticlePubMedPMC
- 29. Mendenhall E, Shivashankar R, Tandon N, Ali MK, Narayan KM, Prabhakaran D. Stress and diabetes in socioeconomic context: a qualitative study of urban Indians. Soc Sci Med 2012;75:2522-9.ArticlePubMedPMC
- 30. Neupert SD, Almeida DM, Charles ST. Age differences in reactivity to daily stressors: the role of personal control. J Gerontol B Psychol Sci Soc Sci 2007;62:P216-25.ArticlePubMed
- 31. Fiske A, Wetherell JL, Gatz M. Depression in older adults. Annu Rev Clin Psychol 2009;5:363-89.ArticlePubMedPMC
- 32. Andres AR, Collings S, Qin P. Sex-specific impact of socioeconomic factors on suicide risk: a population-based case-control study in Denmark. Eur J Public Health 2010;20:265-70.ArticlePubMed
- 33. Ogunwole SM, Golden SH. Social determinants of health and structural inequities: root causes of diabetes disparities. Diabetes Care 2021;44:11-3.ArticlePubMedPDF
- 34. Wium-Andersen IK, Osler M, Jorgensen MB, Rungby J, Wium-Andersen MK. Diabetes, antidiabetic medications and risk of depression: a population-based cohort and nested case-control study. Psychoneuroendocrinology 2022;140:105715.ArticlePubMed
- 35. Khaledi M, Haghighatdoost F, Feizi A, Aminorroaya A. The prevalence of comorbid depression in patients with type 2 diabetes: an updated systematic review and meta-analysis on huge number of observational studies. Acta Diabetol 2019;56:631-50.ArticlePubMedPDF
REFERENCES
Figure & Data
References
Citations
 PubReader
PubReader ePub Link
ePub Link Cite
Cite- Figure
-



- Related articles
-
- The Risk of Shoulder Adhesive Capsulitis in Individuals with Prediabetes and Type 2 Diabetes Mellitus: A Longitudinal Nationwide Population-Based Study
- Low Household Income Status and Death from Pneumonia in People with Type 2 Diabetes Mellitus: A Nationwide Study
- Glycemia according to the Use of Continuous Glucose Monitoring among Adults with Type 1 Diabetes Mellitus in Korea: A Real-World Study



