
- Current
- Browse
- Collections
-
For contributors
- For Authors
- Instructions to authors
- Article processing charge
- e-submission
- For Reviewers
- Instructions for reviewers
- How to become a reviewer
- Best reviewers
- For Readers
- Readership
- Subscription
- Permission guidelines
- About
- Editorial policy
Articles
- Page Path
- HOME > Diabetes Metab J > Volume 40(4); 2016 > Article
-
ReviewObesity and Metabolic Syndrome The Effect of Regular Exercise on Insulin Sensitivity in Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis
-
Kimberley L. Way1,2,3
 , Daniel A. Hackett1, Michael K. Baker3,4, Nathan A. Johnson1,2,3
, Daniel A. Hackett1, Michael K. Baker3,4, Nathan A. Johnson1,2,3 -
Diabetes & Metabolism Journal 2016;40(4):253-271.
DOI: https://doi.org/10.4093/dmj.2016.40.4.253
Published online: August 2, 2016
1University of Sydney Faculty of Health Sciences, Lidcombe, Australia.
2Charles Perkins Centre, University of Sydney, Camperdown, Australia.
3Boden Institute of Obesity, Nutrition, Exercise and Eating Disorders, Sydney Medical School University of Sydney, Camperdown, Australia.
4Australian Catholic University School of Exercise Science, Strathfield, Australia.
- Corresponding author: Kimberley L. Way. Charles Perkins Centre, University of Sydney, Camperdown, NSW 2006, Australia. kway2744@uni.sydney.edu.au
- Corresponding author: Nathan A. Johnson. Charles Perkins Centre, University of Sydney, Camperdown, NSW 2006, Australia. nathan.johnson@sydney.edu.au
Copyright © 2016 Korean Diabetes Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
- The purpose of this study was to examine the effect of regular exercise training on insulin sensitivity in adults with type 2 diabetes mellitus (T2DM) using the pooled data available from randomised controlled trials. In addition, we sought to determine whether short-term periods of physical inactivity diminish the exercise-induced improvement in insulin sensitivity. Eligible trials included exercise interventions that involved ≥3 exercise sessions, and reported a dynamic measurement of insulin sensitivity. There was a significant pooled effect size (ES) for the effect of exercise on insulin sensitivity (ES, –0.588; 95% confidence interval [CI], –0.816 to –0.359; P<0.001). Of the 14 studies included for meta-analyses, nine studies reported the time of data collection from the last exercise bout. There was a significant improvement in insulin sensitivity in favour of exercise versus control between 48 and 72 hours after exercise (ES, –0.702; 95% CI, –1.392 to –0.012; P=0.046); and this persisted when insulin sensitivity was measured more than 72 hours after the last exercise session (ES, –0.890; 95% CI, –1.675 to –0.105; P=0.026). Regular exercise has a significant benefit on insulin sensitivity in adults with T2DM and this may persist beyond 72 hours after the last exercise session.
- Exercise is an integral component of the lifestyle management of type 2 diabetes mellitus (T2DM). Current exercise guidelines recommend that adults with T2DM should undertake aerobic-type exercise at moderate and/or vigorous intensity on 3 to 5 days per week, ideally combined with regular vigorous progressive resistance training (PRT) [12]. Meta-analyses have demonstrated that this dose of regular exercise is effective in improving glycaemic control as measured by change in glycosylated hemoglobin (HbA1c) in diabetic cohorts [3].
- Insulin resistance itself has been shown to significantly increase the incidence and prevalence of cardiovascular disease (CVD) in individuals with T2DM [4]. For instance, in a longitudinal study which monitored CVD in individuals with T2DM, each unit increase in homeostasis model of insulin resistance was associated with a 31% greater risk of CVD (odds ratio [OR], 1.48), and a 56% elevated risk of CVD in individuals who were followed-up at 52 months (OR, 2.24) [4]. In a study which examined insulin-stimulated glycaemic control in healthy individuals over a 4 to 11 years period, greater insulin resistance was associated with an increased incidence of age-related chronic conditions including hypertension, coronary heart disease, stroke, and cancer [5]. Thus insulin resistance itself has a significant detrimental impact on health and the development of chronic disease.
- The role of chronic versus acute factors in accounting for the insulin sensitizing benefit of exercise is unclear, and this has implications for the use of exercise in the management of T2DM. For instance, exercise increases insulin-mediated glucose transporter type 4 (GLUT4) translocation to the sarcolemma and subsequent glucose uptake, which may reflect a transient elevation as a consequence of the "last bout" [6]. The underlying increase in GLUT4 transcription and expression of GLUT4 mRNA has been shown to persist for 3 to 24 hours after exercise [78]. In this way, regular exercise translates into a steady-state increase of GLUT4 protein expression, and subsequent improvement in glucose control over time [7]. Similarly, enhanced whole-body insulin sensitivity has been shown to occur in the hours immediately following exercise, and evidence from a limited number of studies using hyperinsulinaemic-euglycaemic clamp and oral glucose tolerance test (OGTT) suggests that this may persist for up to 24 to 72 hours after the last bout [1910]. Current guidelines reflect this concept of a transient benefit that may be "lost," by recommending that consecutive days of physical inactivity should be avoided [12].
- However, while there is evidence that supports the use of exercise as a management strategy to control HbA1c and fasting insulin in T2DM, these static measurements do not directly evaluate the underlying insulin sensitivity [11]. To our knowledge, there is limited data concerning the effect of regular exercise on dynamically measured insulin sensitivity in people with T2DM [112], and no systematic examination and meta-analysis of the pooled evidence has been undertaken.
- The purpose of this study was to examine the effect of regular exercise training on insulin sensitivity in people with T2DM using the collective data available from randomised controlled trials (RCTs). In addition, we sought to determine whether short-term (days) periods of physical inactivity diminish the exercise-induced improvement in insulin sensitivity in adults with T2DM.
INTRODUCTION
- Design
- Electronic database searches were performed in AMED, MEDLINE, SPORTDiscus, CINAHL, EMBASE, and Web of Science Core Collections from earliest record to December 2014. The search strategy combined terms covering the areas of aerobic exercise training, strength training, and insulin sensitivity. Specifically, the database searches were performed using the keywords: strength training, weight training, resistance training, progressive training, progressive resistance, weight lifting; or aerobic exercise, endurance exercise, aerobic training, endurance training, cardio training, exercise, physical endurance, physical exertion; and insulin sensitivity, insulin resistance, tolerance test, OGTT, ITT, IVGTT, MTT, IST, clamp. The latter terms refer to oral glucose tolerance test (OGTT), insulin tolerance test (ITT), intravenous glucose tolerance test (IVGTT), meal tolerance test (MTT), and insulin secretion test (IST), respectively.
- Reference lists of all retrieved papers were manually searched for potentially eligible papers. RCTs published in all languages were included while non-RCTs, uncontrolled trials, cross-sectional studies, and theses were excluded from review.
- Interventions
- Studies were included if the exercise training intervention involved three or more exercise sessions. Trials where participants were randomised to an intervention involving either aerobic exercise (i.e., continuous, intermittent, or high intensity interval training [HIIT]) (aerobic exercise training [AEx]) or PRT, or combined (AEx+PRT), were included. Studies involving dietary interventions were included only if the diet was the same in the exercise and control groups.
- Participants
- Trials that were completed with individuals with T2DM, who were of 18 years or older, were included in the review.
- Outcome measures
- Trials that were eligible for the review reported measurements that assessed dynamic insulin sensitivity. Measures that were considered as dynamic assessments of insulin sensitivity evaluated the glucose response to insulin/glucose stimulation. To be eligible for review, studies needed to report the change in glucose based on the dynamic insulin sensitivity assessment.
- Glucose levels are clamped and titrated at a predetermined level, in conjunction with continuous insulin infusion at a fixed rate. It is considered the gold standard measure for insulin resistance [13]. Blood concentrations are measured every 3 to 5 minutes. Insulin resistance is determined by the rate/amount of glucose that is necessary to maintain the predetermined blood glucose concentration [13].
- This measurement also involves clamping glucose at a predetermined hyperglycaemic level by intravenously infusing glucose into the blood. Insulin sensitivity is calculated by dividing the glucose infusion rate needed to maintain a hyperglycaemic state by the mean insulin concentration over the last 20 to 30 minutes of the clamp [13].
- Insulin infusion testing is similar to clamping methods, but without the intensive blood sampling that is used in the clamping methodology. Somatostatin may also be infused in these tests to suppress endogenous insulin secretion, glucagon, growth hormone, and gluconeogenesis. Glucose, insulin, and somatostatin are infused continuously for 150 to 180 minutes at predetermined constant rates. The steady state plasma glucose, the mean glucose over the last 30 minutes of the test, reflects insulin sensitivity/resistance [13].
- Insulin resistance in this assessment is estimated by the rate of decline in glucose levels following an intravenous bolus of insulin. Blood samples are taken every 2 minutes for 15 minutes and reflect the suppression of hepatic glucose output and stimulation of peripheral glucose uptake. The rate, expressed as a percentage decline in glucose per minute, is calculated by the rate of decline of the log transformed glucose concentrations by linear regression. This calculation reflects insulin sensitivity [13].
- OGTT assesses insulin resistance and secretion by sampling the plasma glucose concentrations typically every 15 to 30 minutes for 2 hours following a 75 g oral glucose load [13]. The individual must be in a fasted state (8 to 14 hours) prior to completing the test. There are several surrogate markers of insulin resistance that can be obtained from an OGTT, such as the Matsuda index, Gutt index, Stumvoll index, Avignon index, and oral glucose sensitivity index [11]. The OGTT has been shown to correlate with the hyperglycaemic clamp as a measure of insulin resistance [14].
- Selection of studies
- After eliminating duplications the search results were screened by two investigators (KLW, DAH) against the eligibility criteria, and those references that could not be eliminated by title or abstract were retrieved and independently reviewed by two reviewers (KLW, DAH) in an unblinded manner. Disagreements were resolved by discussion or by a third and forth researcher (MKB, NAJ). In cases where journal articles contained insufficient information, attempts were made to contact authors to obtain missing details (KLW, DAH).
- Data extraction and calculations
- Data relating to participant characteristics (age, sex, body mass index [BMI]), exercise intervention (mode of exercise, exercise frequency, intensity, duration, and intervention duration) and measures of insulin sensitivity were extracted independently by two researchers (KLW, DAH), with disagreements resolved by discussion or by two researchers (MKB, NAJ).
- Assessment of methodological quality
- Two researchers (KLW, DAH) assessed the methodological quality of the included studies (in a blinded manner) using a modified Downs and Black [15] checklist recommended by the Cochrane Handbook for Systematic Reviews of Interventions [16]. The tool consists of 27 items rated as 'no, 0; unable to determine, 0; and yes, 1' and includes criteria such as: clear description of the aims, interventions, outcome measurements and participants, representativeness of participant groups, appropriateness of statistical analyses, and correct reporting. The checklist was slightly modified so that the final item (number 27) relating to statistical power was consistent with the scoring used for the other items (i.e., from the original score of 0 to 5 to 'no, 0; unable to determine, 0; and yes, 1'). Additionally, two extra criteria were added to the checklist; these were exercise supervision, and monitoring the adherence of participants during the intervention (Supplementary Table 1).
- The within trial standardised mean difference, or effect size (ES), and 95% confidence intervals (CIs) were calculated. Between-study variability was examined using the I2 measure of inconsistency. This statistic, expressed as a percentage between 0 to 100, provides a measure of how much of the variability between studies is due to heterogeneity rather than chance. Publication bias was assessed by using Egger's test. Subsequently this resulted in two studies [17,18] being excluded from the analyses due to unrealistic large positive effects.
- Meta-analyses
- Pooled estimates of the effect of exercise on insulin sensitivity, using ES, were obtained using a random-effects model. Subanalyses were also undertaken to examine the effect of: (1) exercise versus control on insulin sensitivity measured <48 hours after the last exercise bout; (2) exercise versus control on insulin sensitivity measured 48 to 72 hours after the last exercise bout and; and (3) exercise versus control on insulin sensitivity measured >72 hours after the last exercise bout. All analyses were conducted using Comprehensive Meta-Analysis version 2 (Biostat Inc., Englewood, NJ, USA).
METHODS
Clamps: euglycaemic clamp
Clamps: hyperglycaemic clamp
Insulin infusion sensitivity tests
Insulin tolerance test
Oral glucose tolerance test
Analyses
- Identification and selection of studies
- The original search yielded 27,041 studies. One study was found from the reference lists of the manuscripts retrieved. After removal of duplicates and elimination of papers based on the eligibility criteria, 16 studies remained (Supplementary Fig. 1).
- Cohort characteristics
- Participant characteristics for included studies are shown in Table 1. Of the studies examined, the majority were conducted in previously inactive T2DM populations, predominantly with male cohorts. When combined, 479 individuals (193 male; 166 female; 120 not reported) participated in the trials. One study exclusively recruited female participants [19], two studies exclusively recruited male participants [2021], nine studies recruited both males and females [171822232425262728], and sex was not reported in four studies [29303132]. The reported mean age of participants ranged from 45.0 to 69.5 years. Based on BMI classification [33], seven studies had participants who were classified on average as overweight [17,18,21,22,23,24,25], six as obese class I [192627282930], and two as obese class II [2032]. There was one study that did not report mean BMI [31].
- Exercise characteristics
- Exercise intervention characteristics are displayed in Table 2. Walking was the most common mode of AEx, while exercises with weight machines were most commonly used for PRT. For the AEx training interventions, 10 studies used continuous training [17,182124272829303132], two studies used a combination of continuous and HIIT [2130], and one study compared continuous training with HIIT [24]. AEx training was most commonly performed 3 days per week [1721282930] with sessions lasting 25 to 60 minutes for 1 to 26 weeks. Aerobic exercise intensity, expressed as a percentage of maximal heart rate (HRmax), percentage of heart rate reserve, percentage or peak of maximal rate of oxygen consumption, or percentage of peak energy expenditure, ranged from 35% to 95% [21718192124,2526282931]. PRT was combined with AEx training in five studies [1922232526], whilst PRT was performed alone in two studies [2022]. PRT was most commonly performed 3 days per week, involving two sets per exercise for eight to 12 repetitions, for 10 to 24 weeks. The intensity of PRT, quantified as a percentage of one-repetition maximum (1 RM) in three studies, ranged between 50% to 70% 1 RM [222526]. One study prescribed intensity as 10 to 15 of RM [20].
- Four studies included a dietary or supplement intervention in conjunction with exercise and control [17183032]. Omega 3 polyunsaturated fatty acid supplementation as fish meal was implemented in one of the studies [17], and branched chain amino acid supplementation in another study [30]. Two studies used diet interventions aimed at energy restriction of either 27.9 kcal/kg of ideal body weight [18] or body weight reduction (1 kg/week) [32]. In all of these studies, the same dietary intervention was given to both exercise and control groups.
- Methodological quality
- All included studies specified their hypotheses, main outcomes, participant characteristics, interventions, main findings, variability estimates, representative participants, statistical tests, and accuracy of measures (Supplementary Table 1). The majority of studies provided supervision for the intervention groups [17192024252627282930,32] and reported adherence to exercise training during the intervention [171920222325262728293032]. There were eight studies that did not report adverse events during the intervention [1819212224263132], five studies did not report participants lost to follow-up [1819202132], and 10 studies did not report P values from statistical analysis [18192023252627283032]. The total score for methodological quality ranged from 16 to 24, out of a possible 29 points, indicating generally moderate study quality.
- Study outcomes (ineligible for meta-analysis)
- Table 3 shows the extracted outcome measures of all studies included. Two studies were excluded from the meta-analyses due to publication bias, as identified via visual inspection of funnel plot analyses and Egger's test [1718] (Y intercept, –5.287; standard error [SE], 0.895; 95% CI, –7.166 to –3.407; P<0.000). Upon exclusion, publication bias was improved (Y intercept, –2.942; SE, 0.816; 95% CI, –4.692 to –1.192; P=0.003). Three studies were excluded from the time effect subgroup analyses because they did not report timing of data collection postintervention [232631]. These studies found regular exercise therapy to have a positive effect on glucose uptake as measured by clamp [23] and OGTT [2631] (Okada et al. [23]: pre, 11.1±5.3 mmol/L, post, 9.7±4.2 mmol/L; Ronnemaa et al. [31]: pre, 19.7±4.9 mmol/L, post, 16.5±7.6 mmol/L; Tessier et al. [26]: pre, 16.6±3.8, post, 15.3±3.1 area under the curve). Only one of these studies was found to have a statistically significant effect (P=0.04) [23].
- Study outcomes (meta-analyses)
- The meta-analysis was conducted with 14 studies involving a total of 411 adult participants. For the time effect subgroup analyses, nine studies reported the time of data collection from the last exercise bout. This included three studies which assessed insulin sensitivity less than 48 hours after the last exercise bout [202729], three studies which assessed insulin sensitivity between 48 and 72 hours after exercise [192532], and three studies which assessed insulin sensitivity more than 72 hours after the last exercise bout [212430]. All eligible studies had sufficient data for calculation of ES and 95% CIs for the purpose of meta-analysis.
- Pooled analysis: exercise versus control
- For the effect of exercise on insulin sensitivity, all 14 studies showed an ES favouring exercise therapy, ranging from –0.080 to –1.428. Seven of these studies reached statistical significance for a benefit of exercise versus control [19212223273032]. There was a significant pooled ES for the effect of exercise on insulin sensitivity via random effects model (ES, –0.588; 95% CI, –0.816 to –0.359; P<0.000) (Fig. 1). Low (non-significant) heterogeneity among studies was observed (I2= 16.723%, P=0.271).
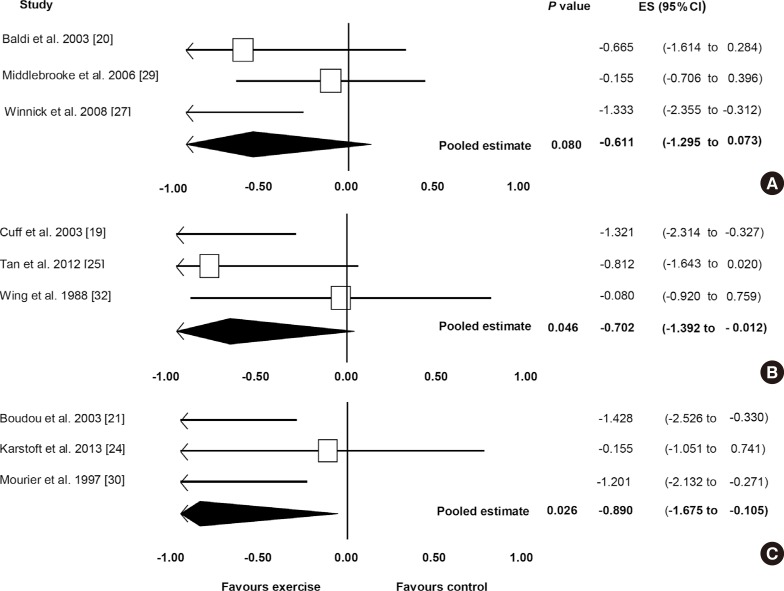
- Subanalysis: exercise versus control (<48 hours)
- Fig. 2A shows the pooled ES for studies for the effect of exercise on insulin sensitivity for <48 hours after the last exercise bout for the comparison of exercise and control. All three studies [202729] showed an ES favouring exercise therapy, ranging from –1.333 to –0.155. One of these studies reached statistical significance of a benefit of exercise therapy (P=0.011) [27]. The pooled ES showed an improvement in insulin sensitivity in favour of exercise therapy (ES, –0.611; 95% CI, –1.295 to 0.073), although this did not reach statistical significance (P=0.080). Low (non-significant) heterogeneity among studies was observed (I2=39.735%, P=0.103).
- Subanalysis: exercise versus control (48 to 72 hours)
- Fig. 2B shows the pooled ES for the effect of exercise on insulin sensitivity measured between 48 and 72 hours after the last exercise bout, for the comparison between exercise and control. There was a significant effect favouring exercise versus control (ES, –0.702; 95% CI, –1.392 to –0.012; P=0.046). All three studies [192532] showed an ES favouring exercise therapy, ranging from –1.321 to –0.080, with one of the studies showing a statistically significant improvement with exercise therapy [19]. Low (non-significant) heterogeneity among studies was observed (I2=45.258%, P=0.161).
- Subanalysis: exercise versus control (>72 hours)
- Fig. 2C displays the pooled ES for effect of exercise on insulin sensitivity measured more than 72 hours after the last exercise bout. A significant effect was observed favouring exercise therapy (ES, –0.890; 95% CI, –1.675 to –0.105; P=0.026). All three studies [212430] showed an ES favouring exercise therapy, ranging from –1.428 to –0.155. Two of the analysed studies reached statistical significance for the benefit of exercise on insulin sensitivity [2130]. Low (non-significant) heterogeneity among studies was observed (I2=49.0578%, P=0.140).
RESULTS
- Insulin resistance contributes significantly to the pathophysiology of T2DM and increases the risk of heart disease and cancer. To our knowledge, this is the first systematic review with meta-analyses to examine the effect of regular exercise training on dynamic measures of insulin sensitivity in adults with T2DM. The results suggest that, when compared with a control intervention, regular exercise improves insulin sensitivity in T2DM, and this may persist for more than 72 hours after the last exercise bout.
- It is generally accepted that regular exercise improves blood glucose control and enhances insulin sensitivity. A previous review and meta-analysis found that structured exercise training had a positive effect on HbA1c levels in adults with T2DM [3], when compared with control. As reported by Umpierre et al. [3], individuals who exercised ≥150 minutes per week showed a significant reduction in HbA1c (–0.89%) compared with those who participated in less than 150 minutes. Another systematic review and meta-analysis which investigated the effect of short-term exercise training (≤2 weeks) on glycaemic control, as measured with continuous glucose monitoring in T2DM, showed that exercise significantly reduced the daily time spent in hyperglycaemia (>10.0 mmol/L), but did not significantly change fasting blood glucose levels [34]. Statistical analysis of longer-term interventions could not be undertaken in this study due to the heterogeneity in the timing of the continuous glucose monitoring measures. Thus whilst regular exercise improves HbA1c and appears to reduce hyperglycaemic incidence, this evidence is based on static measures of glycaemic control and not insulin sensitivity per se. HbA1c is predominately used as a tool for assessing long-term glycaemic control and is considered a representation of fasting and postprandial glycaemia. Fasting glucose and insulin measures are more representative of glycaemic control and basal hyperinsulinemia; however, they do not necessarily reflect glycaemic response to insulin (insulin sensitivity/resistance).
- Insulin resistance is marked by a decreased responsiveness to metabolic actions of insulin such as insulin-stimulated glucose disposal and inhibition of hepatic glucose output [35]. Dynamic measures of insulin sensitivity mimic stimulated insulin action, and reflect the peripheral insulin-mediated glucose uptake, making these more sensitive measures than static techniques. Due to the major role of insulin resistance in T2DM, it is therefore important that dynamic measures are considered as assessment strategies to assess the efficacy of interventions [35]. Our study highlights that currently there is a relative lack of evidence from exercise training interventions that have used outcome measures that are valid indices of insulin sensitivity.
- Exercise is one of the first management strategies suggested by health professionals for glycaemic control in individuals with T2DM. The American College of Sports Medicine and American Diabetes Association joint position statement [1], and the American Heart Association [2] exercise guidelines recommend that individuals with T2DM should undertake exercise no less than every 48 hours to manage blood glucose levels and insulin resistance [127], and it has been suggested that the insulin sensitizing effect of exercise may be lost after 48 to 72 hours [3637]. However, it is generally acknowledged that the improvements seen in insulin sensitivity are not just attributable to acute exercise benefits (repeated regularly via training), but also chronic physiological changes (adaptations) in glucose/insulin metabolism [6]. Namely, an acute bout of exercise has been shown to improve insulin sensitivity in both diabetic [37] and healthy [63637] cohorts, but this effect is transient and diminishes during subsequent days without training [63637]. Yet, cross-sectional data show that endurance athletes; for instance, have a higher insulin responsiveness and greater peripheral glucose uptake than untrained healthy individuals even when the "last bout effect" is removed [3839]. Similarly, our results from the limited available data provide support for this at the whole body level by showing that regular exercise enhances insulin sensitivity in individuals with T2DM and the magnitude is greater than pre-training levels irrespective of whether there is a short (<48 hours) or longer (>72 hours) period of interspersed inactivity. From a clinical perspective, this may imply that with adherence to chronic/regular exercise training, improved insulin sensitivity can be maintained in people receiving exercise for T2DM management, despite periods of inactivity.
- Despite the general consensus that regular exercise is effective for the management of insulin resistance in T2DM, our review highlights a relative lack of data available from high quality studies (14 studies for the pooled analysis in our study) to support this. It does however provide phenotypic support that chronic regular exercise does have a persisting effect that appears to be diminished with acute exercise alone. It is still unclear what dosage and types of exercise result in persisting insulin sensitivity because different exercise modalities, intensities, and durations were used in the eligible studies. Only nine studies reported the time point that insulin sensitivity measures were collected post-intervention. Of these nine studies, only three studies were eligible to be grouped into each time-point subanalyses. While this provides some evidence that chronic exercise has a persisting effect on insulin sensitivity, it is clear that future research needs to investigate this lasting effect. In the time-point subanalyses, only one study implemented PRT [20] and one study used combined exercise therapy (AEx and PRT) [25]. The American College of Sports Medicine and American Diabetes Association joint position statement [1] and the American Heart Association [2] exercise guidelines recommend that individuals with T2DM should partake in combined exercise therapy to manage blood glucose levels and insulin resistance. However, it is clear from our analyses that there is a lack of data available concerning the effect of combined exercise therapy on insulin sensitivity. It is important to note that the eligible studies adhered to the current exercise guidelines (mode, frequency, duration, and intensity) for T2DM glycaemic control [12]. Our study reinforces the importance of regular exercise, as suggested by the current exercise guidelines, and its enhancement of insulin sensitivity. The exercise-induced increase in insulin sensitivity is believed to reflect adaptations in muscle insulin signaling [4041], GLUT4 protein expression, content and action [67] and associated improvement in insulin-stimulated glucose disposal and glycogen synthesis [4041]. This is accompanied and influenced by enhanced intramyocellular oxidative enzyme capacity and possibly changes in muscle architecture from fast-type to slow-type fibres [4243]. Our analysis supports evidence showing that regular exercise training can produce persistent physiological adaptations that improve insulin sensitivity, which may not just be as a result of transient physiologic responses.
- There are some limitations of the current study that should be considered when interpreting the results. Only nine studies met the inclusion criteria and were eligible for the conducted subanalyses, and these were limited by small sample sizes [192021242527293032]. Given the potential efficacy of exercise and the generally positive findings of existing studies, there is a clear need for further research examining the effectiveness of exercise interventions on insulin sensitivity, using dynamic measurements. Furthermore, differences in exercise prescription (intensity, duration, frequency, and intervention length) contributed to heterogeneity in the available research. Similarly, the differences in dynamic measurement techniques could further contribute to heterogeneity (clamp, OGTT, and ITT). Evaluating the quality of studies using the Down and Black scale found all of the analyzed studies to be of moderate quality. This may have also contributed to the heterogeneity of the results. There has been a limited investigation of the effect of interval aerobic exercise training on insulin sensitivity in T2DM, despite its known benefit in improving glucose uptake in healthy populations. Further research needs to be conducted to investigate optimal exercise prescription and the treatment of insulin sensitivity in T2DM.
- This systematic review with meta-analyses provides useful information for the clinical application of exercise in the management of T2DM. The results show clear evidence for the effectiveness of exercise therapy for improving insulin sensitivity for at least 72 hours after the final bout. However, it cannot be determined whether exercise training frequency may be reduced to this extent, or if more frequent training, as performed in the included studies, is required for the insulin sensitizing effect to become apparent. The results have implications for clinicians in regards to advice pertaining to unexpected breaks from exercise training: a trained individual with T2DM may have a 24- to 72-hour gap in between training sessions due to injury, personal or family reasons. Our results indicate that within this time frame the insulin sensitizing effect is not lost; thus, there may be no increased risk of hyperglycemia or need to adjust medication within this period.
DISCUSSION
- This is the first study to collectively pool data assessing the effect of regular exercise on dynamic measures of insulin sensitivity in people with T2DM. Our study found that regular exercise has a significant benefit on insulin sensitivity, which may persist for 72 hours or longer after the last training bout. While current exercise guidelines for T2DM highlight the importance of avoiding consecutive days of physical inactivity, there is very limited data from high quality RCTs to corroborate this. Our findings suggest that short periods of inactivity (e.g., 72 hours) may not result in a loss of insulin sensitivity, and this may reflect chronic adaptations to the underlying pathophysiology. Therefore, clinicians should reinforce the importance of regular exercise to manage insulin sensitivity as these chronic benefits may ensure that short-term periods of inactivity will not negate the therapeutic effect from generally regular exercise participation. This study also highlights the relative lack of evidence investigating the effect of insulin sensitivity after prolonged physical inactivity (beyond 72 hours) making it difficult to conclude on the lasting insulin sensitizing effect.
CONCLUSIONS
-
Acknowledgements
- Miss Kimberley L. Way is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Miss Way would like to thank her co-authors for their continuous work and contribution in the development of this manuscript.
ACKNOWLEDGMENTS
-
CONFLICTS OF INTEREST: No potential conflict of interest relevant to this article was reported.
NOTES
Supplementary Material
Supplementary Table 1
- 1. Colberg SR, Albright AL, Blissmer BJ, Braun B, Chasan-Taber L, Fernhall B, Regensteiner JG, Rubin RR, Sigal RJ. American College of Sports Medicine. American Diabetes Association. Exercise and type 2 diabetes: American College of Sports Medicine and the American Diabetes Association: joint position statement. Exercise and type 2 diabetes. Med Sci Sports Exerc 2010;42:2282-2303. PubMed
- 2. Marwick TH, Hordern MD, Miller T, Chyun DA, Bertoni AG, Blumenthal RS, Philippides G, Rocchini A. Council on Clinical Cardiology, American Heart Association Exercise, Cardiac Rehabilitation, and Prevention Committee. Council on Cardiovascular Disease in the Young; Council on Cardiovascular Nursing. Council on Nutrition, Physical Activity, and Metabolism. Interdisciplinary Council on Quality of Care and Outcomes Research. Exercise training for type 2 diabetes mellitus: impact on cardiovascular risk: a scientific statement from the American Heart Association. Circulation 2009;119:3244-3262. ArticlePubMed
- 3. Umpierre D, Ribeiro PA, Kramer CK, Leitao CB, Zucatti AT, Azevedo MJ, Gross JL, Ribeiro JP, Schaan BD. Physical activity advice only or structured exercise training and association with HbA1c levels in type 2 diabetes: a systematic review and meta-analysis. JAMA 2011;305:1790-1799. ArticlePubMed
- 4. Bonora E, Formentini G, Calcaterra F, Lombardi S, Marini F, Zenari L, Saggiani F, Poli M, Perbellini S, Raffaelli A, Cacciatori V, Santi L, Targher G, Bonadonna R, Muggeo M. HOMA-estimated insulin resistance is an independent predictor of cardiovascular disease in type 2 diabetic subjects: prospective data from the Verona Diabetes Complications Study. Diabetes Care 2002;25:1135-1141. PubMed
- 5. Facchini FS, Hua N, Abbasi F, Reaven GM. Insulin resistance as a predictor of age-related diseases. J Clin Endocrinol Metab 2001;86:3574-3578. ArticlePubMedPDF
- 6. Borghouts LB, Keizer HA. Exercise and insulin sensitivity: a review. Int J Sports Med 2000;21:1-12. ArticlePubMed
- 7. Richter EA, Hargreaves M. Exercise, GLUT4, and skeletal muscle glucose uptake. Physiol Rev 2013;93:993-1017. ArticlePubMed
- 8. Kraniou GN, Cameron-Smith D, Hargreaves M. Acute exercise and GLUT4 expression in human skeletal muscle: influence of exercise intensity. J Appl Physiol (1985) 2006;101:934-937. ArticlePubMed
- 9. Praet SF, van Loon LJ. Optimizing the therapeutic benefits of exercise in type 2 diabetes. J Appl Physiol (1985) 2007;103:1113-1120. ArticlePubMed
- 10. O'Gorman DJ, Karlsson HK, McQuaid S, Yousif O, Rahman Y, Gasparro D, Glund S, Chibalin AV, Zierath JR, Nolan JJ. Exercise training increases insulin-stimulated glucose disposal and GLUT4 (SLC2A4) protein content in patients with type 2 diabetes. Diabetologia 2006;49:2983-2992. ArticlePubMedPDF
- 11. Singh B, Saxena A. Surrogate markers of insulin resistance: a review. World J Diabetes 2010;1:36-47. ArticlePubMedPMC
- 12. Conn VS, Koopman RJ, Ruppar TM, Phillips LJ, Mehr DR, Hafdahl AR. Insulin sensitivity following exercise interventions: systematic review and meta-analysis of outcomes among healthy adults. J Prim Care Community Health 2014;5:211-222. ArticlePubMedPMCPDF
- 13. Wallace TM, Matthews DR. The assessment of insulin resistance in man. Diabet Med 2002;19:527-534. ArticlePubMed
- 14. Nijpels G, van der Wal PS, Bouter LM, Heine RJ. Comparison of three methods for the quantification of beta-cell function and insulin sensitivity. Diabetes Res Clin Pract 1994;26:189-195. PubMed
- 15. Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health 1998;52:377-384. ArticlePubMedPMC
- 16. Higgins JP, Green S. Cochrane Collaboration. Cochrane handbook for systematic reviews of interventions. Chichester: Wiley-Blackwell; 2008.
- 17. Dunstan DW, Mori TA, Puddey IB, Beilin LJ, Burke V, Morton AR, Stanton KG. The independent and combined effects of aerobic exercise and dietary fish intake on serum lipids and glycemic control in NIDDM. A randomized controlled study. Diabetes Care 1997;20:913-921. ArticlePubMedPDF
- 18. Tamura Y, Tanaka Y, Sato F, Choi JB, Watada H, Niwa M, Kinoshita J, Ooka A, Kumashiro N, Igarashi Y, Kyogoku S, Maehara T, Kawasumi M, Hirose T, Kawamori R. Effects of diet and exercise on muscle and liver intracellular lipid contents and insulin sensitivity in type 2 diabetic patients. J Clin Endocrinol Metab 2005;90:3191-3196. ArticlePubMed
- 19. Cuff DJ, Meneilly GS, Martin A, Ignaszewski A, Tildesley HD, Frohlich JJ. Effective exercise modality to reduce insulin resistance in women with type 2 diabetes. Diabetes Care 2003;26:2977-2982. ArticlePubMedPDF
- 20. Baldi JC, Snowling N. Resistance training improves glycaemic control in obese type 2 diabetic men. Int J Sports Med 2003;24:419-423. ArticlePubMed
- 21. Boudou P, Sobngwi E, Mauvais-Jarvis F, Vexiau P, Gautier JF. Absence of exercise-induced variations in adiponectin levels despite decreased abdominal adiposity and improved insulin sensitivity in type 2 diabetic men. Eur J Endocrinol 2003;149:421-424. ArticlePubMed
- 22. Dunstan DW, Puddey IB, Beilin LJ, Burke V, Morton AR, Stanton KG. Effects of a short-term circuit weight training program on glycaemic control in NIDDM. Diabetes Res Clin Pract 1998;40:53-61. ArticlePubMed
- 23. Okada S, Hiuge A, Makino H, Nagumo A, Takaki H, Konishi H, Goto Y, Yoshimasa Y, Miyamoto Y. Effect of exercise intervention on endothelial function and incidence of cardiovascular disease in patients with type 2 diabetes. J Atheroscler Thromb 2010;17:828-833. ArticlePubMed
- 24. Karstoft K, Winding K, Knudsen SH, Nielsen JS, Thomsen C, Pedersen BK, Solomon TP. The effects of free-living interval-walking training on glycemic control, body composition, and physical fitness in type 2 diabetic patients: a randomized, controlled trial. Diabetes Care 2013;36:228-236. PubMedPMC
- 25. Tan S, Li W, Wang J. Effects of six months of combined aerobic and resistance training for elderly patients with a long history of type 2 diabetes. J Sports Sci Med 2012;11:495-501. PubMedPMC
- 26. Tessier D, Menard J, Fulop T, Ardilouze J, Roy M, Dubuc N, Dubois M, Gauthier P. Effects of aerobic physical exercise in the elderly with type 2 diabetes mellitus. Arch Gerontol Geriatr 2000;31:121-132. ArticlePubMed
- 27. Winnick JJ, Sherman WM, Habash DL, Stout MB, Failla ML, Belury MA, Schuster DP. Short-term aerobic exercise training in obese humans with type 2 diabetes mellitus improves whole-body insulin sensitivity through gains in peripheral, not hepatic insulin sensitivity. J Clin Endocrinol Metab 2008;93:771-778. ArticlePubMed
- 28. Ligtenberg PC, Hoekstra JB, Bol E, Zonderland ML, Erkelens DW. Effects of physical training on metabolic control in elderly type 2 diabetes mellitus patients. Clin Sci (Lond) 1997;93:127-135. ArticlePubMedPDF
- 29. Middlebrooke AR, Elston LM, Macleod KM, Mawson DM, Ball CI, Shore AC, Tooke JE. Six months of aerobic exercise does not improve microvascular function in type 2 diabetes mellitus. Diabetologia 2006;49:2263-2271. ArticlePubMedPDF
- 30. Mourier A, Gautier JF, De Kerviler E, Bigard AX, Villette JM, Garnier JP, Duvallet A, Guezennec CY, Cathelineau G. Mobilization of visceral adipose tissue related to the improvement in insulin sensitivity in response to physical training in NIDDM. Effects of branched-chain amino acid supplements. Diabetes Care 1997;20:385-391. ArticlePubMedPDF
- 31. Ronnemaa T, Mattila K, Lehtonen A, Kallio V. A controlled randomized study on the effect of long-term physical exercise on the metabolic control in type 2 diabetic patients. Acta Med Scand 1986;220:219-224. ArticlePubMed
- 32. Wing RR, Epstein LH, Paternostro-Bayles M, Kriska A, Nowalk MP, Gooding W. Exercise in a behavioural weight control programme for obese patients with type 2 (non-insulin-dependent) diabetes. Diabetologia 1988;31:902-909. ArticlePubMedPDF
- 33. Seidell JC, Flegal KM. Assessing obesity: classification and epidemiology. Br Med Bull 1997;53:238-252. ArticlePubMed
- 34. MacLeod SF, Terada T, Chahal BS, Boule NG. Exercise lowers postprandial glucose but not fasting glucose in type 2 diabetes: a meta-analysis of studies using continuous glucose monitoring. Diabetes Metab Res Rev 2013;29:593-603. ArticlePubMed
- 35. Muniyappa R, Lee S, Chen H, Quon MJ. Current approaches for assessing insulin sensitivity and resistance in vivo: advantages, limitations, and appropriate usage. Am J Physiol Endocrinol Metab 2008;294:E15-E26. ArticlePubMed
- 36. Bogardus C, Thuillez P, Ravussin E, Vasquez B, Narimiga M, Azhar S. Effect of muscle glycogen depletion on in vivo insulin action in man. J Clin Invest 1983;72:1605-1610. ArticlePubMedPMC
- 37. Devlin JT, Hirshman M, Horton ED, Horton ES. Enhanced peripheral and splanchnic insulin sensitivity in NIDDM men after single bout of exercise. Diabetes 1987;36:434-439. ArticlePubMed
- 38. McCoy M, Proietto J, Hargreves M. Effect of detraining on GLUT-4 protein in human skeletal muscle. J Appl Physiol (1985) 1994;77:1532-1536. ArticlePubMed
- 39. Mikines KJ, Sonne B, Farrell PA, Tronier B, Galbo H. Effect of training on the dose-response relationship for insulin action in men. J Appl Physiol (1985) 1989;66:695-703. ArticlePubMed
- 40. Christ-Roberts CY, Pratipanawatr T, Pratipanawatr W, Berria R, Belfort R, Kashyap S, Mandarino LJ. Exercise training increases glycogen synthase activity and GLUT4 expression but not insulin signaling in overweight nondiabetic and type 2 diabetic subjects. Metabolism 2004;53:1233-1242. ArticlePubMed
- 41. Holten MK, Zacho M, Gaster M, Juel C, Wojtaszewski JF, Dela F. Strength training increases insulin-mediated glucose uptake, GLUT4 content, and insulin signaling in skeletal muscle in patients with type 2 diabetes. Diabetes 2004;53:294-305. ArticlePubMedPDF
- 42. Holloszy JO, Coyle EF. Adaptations of skeletal muscle to endurance exercise and their metabolic consequences. J Appl Physiol Respir Environ Exerc Physiol 1984;56:831-838. ArticlePubMed
- 43. Bruce CR, Kriketos AD, Cooney GJ, Hawley JA. Disassociation of muscle triglyceride content and insulin sensitivity after exercise training in patients with type 2 diabetes. Diabetologia 2004;47:23-30. ArticlePubMedPDF
REFERENCES

The effect of exercise on insulin sensitivity (A) <48 hours, (B) 48 to 72 hours, and (C) >72 hours after the last bout of exercise. ES, effect size; CI, confidence interval.
Participant characteristics
| Author | Subject, n | Male sex, % | Age, yr | BMI | Medication, n |
|---|---|---|---|---|---|
| Baldi et al. (2003) [20]a |
C, 9 PRT, 9 |
100 |
C, 50.1±3.9 PRT, 46.5±6.3 |
C, 36.4±9.3 PRT, 34.3±9.6 |
Biguanides, 11 Sulfonylureas, 7 |
| Boudou et al. (2003) [21] |
C, 8 AEx, 8 |
100 |
C, 47.9±8.4 AEx, 42.9±5.2 |
C, 30.9±5.2 AEx, 28.3±3.9 |
C: Metformin, 4 Metformin and gliclazide or glibenclamide, 1 AEx: Metformin, 2 Metformin and gliclazide or glibenclamide, 4 |
| Cuff et al. (2003) [19]a |
C, 9 AEx, 9 AEx+PRT, 10 |
0 |
C, 60.0±8.7 AEx, 59.4±5.7 AEx+PRT, 63.4±7.0 |
C, 36.7±6.0 AEx, 32.5±4.2 AEx+PRT, 33.3±4.7 |
Oral hypoglycaemics |
| Dunstan et al. (1997) [17] |
C, 12 AEx, 11 F, 12 AEx+F, 14 |
C, 75 AEx, 72.7 F, 83.3 AEx+F, 71.4 |
C, 53.0±7.0 AEx, 52.3±8.3 F, 54.1±8.2 AEx+F, 52.6±7.2 |
C, 29.7±4.3 AEx, 29.1±2.4 F, 29.8±4.4 AEx+F, 29.9±3.0 |
Antidiabetic and antihyperten- sive medication |
| Dunstan et al. (1998) [22]a |
C, 10 PRT, 11 |
C, 50 PRT, 72.7 |
C, 51.1±7.0 PRT, 50.3±6.6 |
C, 30.1±3.5 PRT, 28.3±2.7 |
Sulfonylureas, 4 Biguanides, 5 Sulfonylureas+biguanides, 10 |
| Karstoft et al. (2013) [24]a |
C, 8 AEx, Continuous, 12 Intermittent, 12 |
C, 62.5 AEx, Continuous, 66.7 Intermittent, 58.3 |
C, 57.1±8.5 AEx, Continuous, 60.8±7.6 Intermittent, 57.5±8.3 |
C, 29.7±5.4 AEx, Continuous, 29.9±5.5 Intermittent, 29.0±4.5 |
Antidiabetic and antihypertensive medication (abstained for 5 days prior to pre-/post-testing) |
| Ligtenberg et al. (1997) [28] |
C, 28 AEx, 30 |
C, 35.7 AEx, 33.3 |
C, 61.0±5.0 AEx, 63.0±5.0 |
C, 31.2±3.3 AEx, 30.8±4.0 |
Oral hypoglycaemics and insulin |
|
Middlebrooke et al. (2006) [29] |
C, 30 AEx, 22 |
At initial recruitment overall, 54.2 |
C, 64.6±6.8 AEx, 61.8±7.7 |
C, 29.9±5.4 AEx, 31.8±4.5 |
Oral hypoglycaemics |
| Mourier et al. (1997) [30]a |
C, 11 AEx, 10 |
At initial recruitment overall, 83.3 |
C, 46.0±10.0 AEx, 45.0±6.3 |
C, 30.1±5.3 AEx, 30.4±2.5 |
Metformin, 14; Sulfonylurea, 3 |
| Okada et al. (2010) [23] |
C, 17 AEx+PRT, 21 |
C, 64.7 AEx, 47.6 |
C, 64.5±5.9 AEx, 61.9±8.6 |
C, 24.5±2.9 AEx, 25.7±3.2 |
Study reported both groups received comparable medical intervention after registration for 3 months |
| Ronnemaa et al. (1986) [31] |
C, 12 AEx, 13 |
At recruitment, 66.7 | At recruitment overall, 52.5 (NR) | NR |
Sulfonylureas, 18 Metformin+sulfonylureas, 10 |
| Tamura et al. (2005) [18]a |
D, 7 AEx+D, 7 |
D, 57.1 AEx+D, 42.8 |
D, 55.0±12.7 AEx+D, 46.3±7.4 |
D, 27.4±8.5 AEx+D, 27.1±7.7 |
D: Sulfonylureas, 3 Metformin+sulfonylureas, 2 α-Glucosidase inhibitor, 2 D+AEx: Sulfonylureas, 3 Metformin+sulfonylureas, 3 α-Glucosidase inhibitor, 1 |
| Tan et al. (2012) [25] |
C, 10 AEx+PRT, 15 |
At recruitment: C, 45.5 AEx+PRT, 44.4 |
C, 64.8±6.8 AEx+PRT, 65.9±4.2 |
C, 25.8±2.5 AEx+PRT, 25.2±2.5 |
Oral hypoglycaemics |
| Tessier et al. (2000) [26] |
C, 20 AEx+PRT, 19 |
C, 55.0 AEx+PRT, 63.2 |
C, 69.5±5.1 AEx+PRT, 69.3±4.2 |
C, 29.4±3.7 AEx+PRT, 30.7±5.4 |
Glyburide: C, 12 AEx+PRT, 10 Metformin: C, 15 AEx, 14 |
| Wing et al. (1988) [32] |
Include study 1: P+D, 12 AEx+D, 10 |
At recruitment: Study 1, 16.0 |
Study 1: P+D, 52.5±8.9 AEx+D, 56.2±7.5 |
Study 1: D+P, 37.2±1.8 AEx+D, 39.5±1.9 |
Study 1: P+D, oral hypogylcaemics, 6 AEx+D, oral hypoglycaemics, 6 |
| Winnick et al. (2008) [27] |
D, 9 AEx+D, 9 |
D, 33.3 AEx+D, 22.2 |
D, 50.9±3.2 AEx+D, 48.4±8.4 |
D, 32.0±5.3 AEx+D, 34.9±3.1 |
At the outset of the study, all participants discontinued diabetic related medication |
Exercise intervention details
| Author | Mode | Nutritional intervention | Frequency | Intensity | Session duration | Intervention duration |
|---|---|---|---|---|---|---|
| Baldi et al. (2003) [20]a |
C: non exercising control PRT: circuit targeting major muscle groups of the upper and lower body |
Nil |
C: NA PRT: 3/7 (supervised) |
C: NA PRT: 10 RM upper body, 15 RM lower body exercises |
C: NA PRT: progressing from one to three sessions/week; multiple sets of 12 reps for 10 exercises (60 seconds recovery between sets) |
10 weeks |
| Boudou et al. (2003) [21] |
C: sham intervention (cycle ergometer) AEx (continuous and HIIT): NR |
Nil |
C: 1/7 (supervised) AEx: 2/7+1/7, respectively (supervised) |
C: 30 W (60 rpm) AEx: Continuous: 75% VO2peak HIIT: 50%–85% VO2peak |
C: 20 minutes AEx: Continuous: 45 minutes HIIT: 5×2 minutes at 85% VO2peak, 3 minutes at 50% VO2peak between exercises |
8 weeks |
| Cuff et al. (2003) [19]a |
C: usual care AEx (continuous): treadmill, stationary cycle ergometers, recumbent steppers, elliptical trainers, and rower ergometer AEx (continuous)+PRT: AEx–treadmills: stationary cycle ergometers, recumbent steppers, elliptical trainers, rowing machines |
Nil |
C: usual care AEx: 3/7 (supervised) AEx+PRT: 3/7 (supervised) |
C: NA AEx: 60%–75% HRR AEx+PRT: AEx: 60%–75% HRR PRT: 2×12 reps |
C: NA AEx: 75 minutes AEx+PRT: 75 minutes |
16 weeks |
| AEx–PRT: stack weight equipment: leg press, leg curl, hip extension, chest press, and latissimus pulldown | ||||||
| Dunstan et al. (1997) [17] |
C: sham exercise (cycle ergometer and stretches) AEx (continuous): cycle ergometer F: sham exercise. Cycle ergometer and stretches AEx (continuous)+F: cycle ergometer |
All participants were advised to reduce their sodium intake <100 mmol/day Fish intake groups were instructed to include one fish meal per day |
C: 3/7 (supervised) AEx: 3/7 (supervised) F: 3/7 (supervised) AEx+F: 3/7 (supervised) |
C: Nil AEx: Week 1: 50%–55% VO2peak Week 2–8: 55%–65% VO2peak F: no workload AEx+F: Week 1: 50%–55% VO2peak Week 2–8: 55%–65% VO2peak |
C: 10 minutes cycling; 30 minutes of stretching AEx: 40 minutes F: 10 minutes cycling; 30 minutes of stretching AEx+F: 40 minutes |
8 weeks |
| Dunstan et al. (1998) [22]a |
C: non-exercising PRT: circuit including leg extension, bench press, leg curl, bicep curls, overhead press, seated row, forearm extension, and abdominal curls |
Nil |
C: NA PRT: 3/7 (supervision NR) |
C: NA PRT: 50%–55% 1 RM |
C: NA PRT: 60 minutes |
8 weeks |
| Karstoft et al. (2013) [24]a |
C: NR AEx: Continuous: walking Intermittent: walking |
Nil |
C: NA AEx: Continuous: 5/7 (unsupervised) Intermittent: 5/7 (unsupervised) |
C: NA AEx: Continuous: 55% of peak energy-expenditure rate Intermittent: 55%–70% of peak energy-expenditure rate |
C: NA AEx: Continuous: 60 minutes Intermittent: 60 minutes (3 minutes at 70% followed by 3 minutes at 55% of peak energy-expenditure rate) |
4 months |
| Ligtenberg et al. (1997) [28] |
C: education program AEx (continuous): Phase 1: cycle ergometer, swimming, treadmill, and rower ergometer Phase 2: exercise at home based on personalised training advice (with contact from investigators) Phase 3: exercise at home without contact from investigators |
Nil |
C: NR AEx: Phase 1: 3/7 supervised for 6 weeks Phase 2: phone calls 1/14 for 6 weeks. NR frequency of exercise Phase 3: NR |
C: NR AEx: Phase 1: 60%–80% VO2peak Phase 2: NR Phase 3: NR |
C: NR AEx: Phase 1: 60 minutes Phase 2: NR Phase 3: NR |
26 weeks |
|
Middlebrooke et al. (2006) [29] |
C: standard care AEx (continuous): NR |
Nil |
C: NA AEx: 3/7 (2/7 supervised; 1/7 unsupervised) |
C: NA AEx: 70%–80% HRmax |
C: NA AEx: 50–60 minutes |
6 months |
| Mourier et al. (1997) [30]a |
C: NR AEx (continuous and HIIT): cycle ergometer |
Branched chain amino acid supplementation (46% leucine, 24% isoleucine, 30% valine) Supplementation did not effect metabolic parameters |
C: NA AEx: 2/7 continuous+1/7 HIIT |
C: NA AEx: Continuous: 75% VO2peak HIIT: 50%–85% VO2peak |
C: NA AEx: 55 minutes HIIT: Continuous: 35 minutes (52 minutes at 85%) HIIT: VO2peak followed by 2 minutes at 50% VO2peak |
8 weeks |
| Okada et al. (2010) [23] |
C: NR AEx (continuous)+PRT: AEx: aerobic dance, and stationary cycle ergometer PRT: NR |
Nil |
C: NA AEx+PRT: 3–5/7 (supervised) |
C: NA AEx+PRT: NR |
C: NA AEx+PRT: AEx: 55 minutes PRT: 20 minutes Overall: 75 minutes |
3 months |
| Ronnemaa et al. (1986) [31] |
C: NA AEx: walking, jogging, or skiing |
Nil |
C: NA AEx: 5–7/7 |
C: NA AEx: 70% VO2peak |
C: NA AEx: 45 minutes |
4 months |
| Tamura et al. (2005) [18]a |
D: Nil AEx (continuous)+D: walking |
Total mean energy intake of 27.9 kcal/kg of ideal body weight for both groups for 2 weeks |
D: NA AEx+D: 2–3/7 (unsupervised) |
D: NA AEx+D: 50%–60% VO2peak |
D: NA AEx+D: 30 minutes per session |
2 weeks |
| Tan et al. (2012) [25] |
C: maintain individual habits of physical activity AEx (continuous)+PRT: AEx: walking, running PRT: knee flexion, knee extension, hip abduction, hip adduction, and standing calf raise |
Nil |
C: NA AEx+PRT: 3/7 (supervised) |
C: NA AEx+PRT: AEx: 55%–70% HRmax PRT: 50%–70% 1 RM |
C: NA AEx+PRT: 60 minutes |
6 months |
| Tessier et al. (2000) [26] |
C: NR AEx (continuous) +PRT: AEx: walking PRT: strength/endurance training of major muscle groups |
Nil |
C: NA AEx+PRT: 3/7 (supervised) |
C: NA AEx+PRT: Initially: 35%–59% HRmax Week 4 onwards: 60%–79% HRmax |
C: NA AEx+PRT: 60 minutes |
16 weeks |
| Wing et al. (1988) [32] |
P+D: sham exercise (light calisthenics and flexibility exercises) AEx+D: walking |
Diet was designed to produce approximately 1 kg/week weight loss |
P+D: 2/7 (unsupervised) AEx+D: 2/7 (unsupervised) |
P+D: low intensity AEx+D: moderate intensity (speed and distance increased until the individual able to walk 3 miles) |
~60 minutes | 10 weeks |
| Winnick et al. (2008) [27] |
D: NA AEx (continuous)+D: treadmill walking |
Diet designed to maintain body weight close to baseline body weight |
D: NA AEx+D: 7/7 |
D: NA AEx+D: Days 1–3, 5–7: 70% VO2peak Day 4: 60% predicted HRmax |
D: NA AEx+D: 2×25 minutes, 10 minutes break between bouts Day 4: 60 minutes |
1 week |
C, control; PRT, progressive resistance training; NA, not applicable; RM, repetition maximum; HIIT, high intensity interval training; NR, not reported; AEx, aerobic training; VO2peak, peak oxygen consumption; HRR, heart rate reserve; F, fish meal; D, diet; HRmax, maximal heart rate; P, placebo.
aConverted from standard error of mean to standard deviation.
Outcomes of intervention studies for change in insulin sensitivity
| Author | Mode, n | Measure | Time post-intervention, hr | Pre, mean±SD | Post, mean±SD | Change score |
|---|---|---|---|---|---|---|
| Baldi et al. (2003) [20]a |
C, 9 PRT, 9 |
OGTT | 36–48 |
2-Hour glucose (mmol/L): C, 16.3±2.7 PRT, 17.0±3.0 |
2-Hour glucose (mmol/L): C, 17.1±2.4 PRT, 16.3±2.1 |
NR |
| Boudou et al. (2003) [21] |
C, 8 AEx, 8 |
ITT | 72–120 |
Constant rate of glucose disappearance (%/min): C, 1.95±1.00 AEx, 2.15±0.65 |
Constant rate of glucose disappearance (%/min): C, 1.80±0.90 AEx, 3.25±0.85 |
NR |
| Cuff et al. (2003) [19]a |
C, 9 AEx, 9 AEx+PRT, 10 |
Clamp | 48–72 |
Glucose infusion rate (mg · kg–1 · min–1): C, 2.29±1.38 AEx, 2.78±1.47 AEx+PRT, 2.36±1.04 |
Glucose infusion rate (mg · kg–1 · min–1): C, NR AEx, NR AEx+PRT, NR |
Glucose infusion rate (mg · kg–1 · min–1): C, 0.07±0.84 AEx, 0.55±1.08 AEx+PRT, 1.82±1.64 |
| Dunstan et al. (1997) [17]b |
C, 12 AEx, 11 F, 12 AEx+F, 14 |
OGTT | >48 |
AUC glucose (mmol/L–1·120 min–1): C, 1,810±340 AEx, 1,916±480 F, 1,787±465 AEx+F, 2,004±500 |
NR |
AUC glucose (mmol/L–1·120 min–1): C, 50±48.5 AEx, –112.5±65.0 F, 87.5±87.5 F+AEx, –87.5±75.0 |
| Dunstan et al. (1998) [22]a |
C, 10 PRT, 11 |
OGTT | >48 | NR | NR |
AUC glucose (mmol/L–1 · 120 min–1): C, 191±265 PRT, –22±205 |
| Karstoft et al. (2013) [24]a |
C, 8 AEx: Continuous, 12 Intermittent, 12 |
OGTT | ≈96 |
2-Hour glucose (mmol/L): C, 14.7±3.96 AEx: Continuous, 14.8±3.46 Intermittent, 16.5±3.12 |
2-Hour glucose (mmol/L): C, 15.7±3.96 AEx: Continuous, 15.0±4.85 Intermittent, 15.4±4.50 |
NR |
| Ligtenberg et al. (1997) [28] |
C, 28 AEx, 30 |
ITT | <72 |
Glucose decline between 4–14 minutes (%·min-1): C, 1.5±1 AEx, 1.8±1.3 |
Glucose decline between 4–14 minutes (%·min-1): C, 1.8±1.1 AEx, 1.8±1.2 |
NR |
| Middlebrooke et al. (2006) [29] |
C, 30 AEx, 22 |
ITT | ≥24 |
ITT slope (mmol/L–1 · min–1): C, –0.17±0.06 AEx, –0.16±0.10 |
ITT slope (mmol/L–1 · min–1): C, –0.17±0.06 AEx, –0.17±0.07 |
NR |
| Mourier et al. (1997) [30]a |
C, 11 AEx, 10 |
ITT | 72–120 |
Constant rate of glucose disappearance (%·min-1): C, 1.86±0.96 AEx, 2.28±0.73 |
Constant rate of glucose disappearance (%·min-1): C, 1.81±0.90 AEx, 3.34±0.95 |
NR |
| Okada et al. (2010) [23] |
C, 17 AEx+PRT, 21 |
SSPG | NR |
SSPG (mmol/L): C, 14.1±3.4 AEx+PRT, 11.1±5.3 |
SSPG (mmol/L): C, 9.7±4.6 AEx+PRT: 9.7±4.2 |
NR |
| Ronnemaa et al. (1986) [31] |
C, 12 AEx, 13 |
OGTT | NR |
2-Hour glucose (mmol/L): C, 19.6±4.1 AEx, 19.7±4.9 |
2-Hour glucose (mmol/L): C, 19.7±2.7 AEx, 16.5±7.6 |
NR |
| Tamura et al. (2005) [18]a |
D, 7 AEx+D, 7 |
Clamp | >24 |
Steady-state glucose infusion rate (mg/kg/min): D, 6.12±2.46 AEx+D, 5.26±0.87 |
Steady-state glucose infusion rate (mg/kg/min): C, 6.49±0.87 AEx+D, 8.22±1.24 |
NR |
| Tan et al. (2012) [25] |
C, 10 AEx+PRT, 15 |
OGTT | 72 |
2-Hour glucose (mmol/L): C, 11.11±5.26 AEx+PRT, 13.9±5.8 |
2-Hour glucose (mmol/L): C, 10.58±4.41 AEx+PRT, 9.83±4.33 |
NR |
| Tessier et al. (2000) [26] |
C, 20 AEx+PRT, 19 |
OGTT | NR |
AUC glucose (mmol/L): C, 16.1±2.9 AEx+PRT, 16.6±3.8 |
AUC glucose (mmol/L): C, 15.9±3.0 AEx+PRT, 15.3±3.1 |
NR |
| Wing et al. (1988) [32] |
P+D, 12 AEx+D, 10 |
OGTT | 72 |
Plasma glucose: 60 minutes (mmol/L): P+D, 14.6±0.9 AEx+D, 14.3±1.2 |
Plasma glucose: 60 minutes (mmol/L): P+D, 11.3±1.2 AEx+D, 10.9±1.3 |
NR |
| Winnick et al. (2008) [27] |
D, 9 AEx+D, 9 |
Clamp | <24 |
Glucose levels (mg/dL): D: 137.0±3.0 (low-dose); 135.0±3.0 (high-dose) AEx+D: 131.0±3.0 (low-dose); 123.0±3.0 (high-dose) |
Glucose levels (mg/dL): D: 131.0±3.0 (low-dose); 119.0±3.0 (high-dose) AEx+D: 129.0±3.0 (low-dose); 124.0±3.0 (high-dose) |
NR |
SD, standard deviation; C, control; PRT, progressive resistance training; OGTT, oral glucose tolerance test; NR, not reported; AEx, aerobic training; ITT, insulin tolerance test; F, fish meal; AUC, area under the curve; SSPG, steady state plasma glucose; D, diet; P, placebo.
aConverted from standard error of mean to standard deviation, bData has been extrapolated from a graph.
Figure & Data
References
Citations
- Exercise Increasing Health-Related Quality of Life in Type 2 Diabetics: A Meta-Analysis
Sohrab Amiri, Mina Fathi-Ashtiani
Physical & Occupational Therapy In Geriatrics.2023; 41(3): 383. CrossRef - Early intervention and intensive management of patients with diabetes, cardiorenal, and metabolic diseases
Yehuda Handelsman, Javed Butler, George L. Bakris, Ralph A. DeFronzo, Gregg C. Fonarow, Jennifer B. Green, George Grunberger, James L. Januzzi, Samuel Klein, Pamela R. Kushner, Darren K. McGuire, Erin D. Michos, Javier Morales, Richard E. Pratley, Matthew
Journal of Diabetes and its Complications.2023; 37(2): 108389. CrossRef - Frequency, intensity and duration of muscle strengthening activity and associations with mental health
Stephen Shannon, Mark Shevlin, Noel Brick, Gavin Breslin
Journal of Affective Disorders.2023; 325: 41. CrossRef - The effects of swimming exercise and detraining on hemorheological parameters and oxidative stress in rats with metabolic syndrome
Busra Emik-Ozdemir, Melek Tunc-Ata, Yasin Ozdemir, Ozgen Kilic-Erkek, Hande Senol, Vural Kucukatay, Melek Bor-Kucukatay
Nutrition Clinique et Métabolisme.2023; 37(2): 94. CrossRef - Exercise and heart disease
Nick Gardner, Christopher Beck
InnovAiT: Education and inspiration for general practice.2023; 16(7): 337. CrossRef - Dietary weight loss-induced improvements in metabolic function are enhanced by exercise in people with obesity and prediabetes
Joseph W. Beals, Brandon D. Kayser, Gordon I. Smith, George G. Schweitzer, Kyleigh Kirbach, Monica L. Kearney, Jun Yoshino, Gibraan Rahman, Rob Knight, Bruce W. Patterson, Samuel Klein
Nature Metabolism.2023; 5(7): 1221. CrossRef - Investigating the Effect of Aerobic and Resistance Training on Insulin Resistance and Some Cardiovascular Disease Risk Factors in Type 2 Diabetes Mellitus Patients: A Systematic Review
Peyman Kaikhosro Doulatyari, Mehran Ghahramani, Kosar Mozaffari
Journal of Clinical Research in Paramedical Sciences.2023;[Epub] CrossRef - Recommendations from Diabetes UK's 2022 diabetes and physical activity workshop
Anna Morris, Chris Bright, Matthew Cocks, Neil Gibson, Louise Goff, Colin Greaves, Simon Griffin, Ben Jane, Florence Kinnafick, Paul Robb, Michelle Roberts, David Salman, John Saxton, Adrian Taylor, Daniel West, Thomas Yates, Rob C. Andrews, Jason M. R. G
Diabetic Medicine.2023;[Epub] CrossRef - Impact of Physical Exercise on Platelets: Focus on Its Effects in Metabolic Chronic Diseases
Cristina Barale, Elena Melchionda, Giulia Tempesta, Alessandro Morotti, Isabella Russo
Antioxidants.2023; 12(8): 1609. CrossRef - Exercise in the Management of Metabolic-Associated Fatty Liver Disease (MAFLD) in Adults: A Position Statement from Exercise and Sport Science Australia
Shelley E. Keating, Angelo Sabag, Kate Hallsworth, Ingrid J. Hickman, Graeme A. Macdonald, Jonathan G. Stine, Jacob George, Nathan A. Johnson
Sports Medicine.2023; 53(12): 2347. CrossRef - Effects of Using the Bioelectrical Impedance Method in Nutritional Guidance for Diabetes
Naoko Nishizaka, Shinichirou Shiozawa, Kohzo Nakayama, Kenichi Hirose
The Japanese Journal of Nutrition and Dietetics.2023; 81(5): 228. CrossRef - Effects of moderate exercise versus light exercise on fasting blood glucose in obese patients with type 2 diabetes mellitus
Manal Kamel Youssef
Physiotherapy Quarterly.2023; 31(3): 101. CrossRef - The Comparison of High-Intensity Interval Training and Moderate-intensity Continuous Training on Inflammatory and Metabolic Variables in Type 2 Diabetes: Study Protocol for A Pilot Randomized Controlled Trial
Sahar Alizadeh, Nahid Mahdieh, Morteza Lotfi Khachak, Mohsen Avandi, Mehdi Hedayati, Camelia Rambod, Hooman Bakhshandeh
Research in Cardiovascular Medicine.2023; 12(4): 117. CrossRef - Acute exercise improves glucose effectiveness but not insulin sensitivity in paraplegia
Gary J. Farkas, Ann M. Swartz, Ashraf S. Gorgey, Arthur S. Berg, David R. Gater
Disability and Rehabilitation.2022; 44(17): 4656. CrossRef - Cultural validation and language translation of the scientific SCI exercise guidelines for use in Indonesia, Japan, Korea, and Thailand
Yukio Mikami, Damayanti Tinduh, KunHo Lee, Chayaporn Chotiyarnwong, Jan W. van der Scheer, Kyung Su Jung, Hiroshi Shinohara, Inggar Narasinta, Seung Hyun Yoon, Napatpaphan Kanjanapanang, Takafumi Sakai, Martha K. Kusumawardhani, Jinho Park, Pannika Prachg
The Journal of Spinal Cord Medicine.2022; 45(6): 821. CrossRef - Effect of Application of Treadmill Training on Metabolic Control and Vitamin D Level in Saudi Patients with Type 2 Diabetes Mellitus
Ahmad El Askary, Alaa Shafie, Mazen Almehmadi, Hatem H. Allam, Lamiaa K. Elsayyad, Asmaa F. Hassan, Bader B. Althobaiti, Mohamed Mansour Khalifa, Tamer Saber, Aisha H. Alharthi, Amal F. Gharib, Deepika Koundal
Computational and Mathematical Methods in Medicine.2022; 2022: 1. CrossRef - Skeletal Muscle Hyperemia: A Potential Bridge Between Post-exercise Hypotension and Glucose Regulation
Thomas K. Pellinger, Chi-An W. Emhoff
Frontiers in Physiology.2022;[Epub] CrossRef - Exercise, Physical Activity, and Cardiometabolic Health
Matthew J. Belanger, Prashant Rao, Jeremy M. Robbins
Cardiology in Review.2022; 30(3): 134. CrossRef - Modeling the effects of physical activity, education, health, and subjective wealth on happiness based on Indonesian national survey data
Bhina Patria
BMC Public Health.2022;[Epub] CrossRef - Effects of time-restricted feeding with different feeding windows on metabolic health: A systematic review of human studies
Zhibo Xie, Zhangyuting He, Yuqian Ye, Yilei Mao
Nutrition.2022; 102: 111764. CrossRef - Effect of Exercise Instructions With Ambulatory Accelerometer in Japanese Patients With Type 2 Diabetes: a Randomized Control Trial
Jin Matsushita, Hiroshi Okada, Yuki Okada, Takashi Sekiyama, Hideto Iida, Atsushi Shindo, Hiroaki Murata, Michiaki Fukui
Frontiers in Endocrinology.2022;[Epub] CrossRef - Resistance Exercise and Cardiovascular Disease in Diabetes Mellitus
Jin-Hwan Yoon
Journal of Obesity & Metabolic Syndrome.2022; 31(2): 97. CrossRef - Inside the diabetic brain: Insulin resistance and molecular mechanism associated with cognitive impairment and its possible therapeutic strategies
Bhaskar Jyoti Dutta, Shamsher Singh, Sanket Seksaria, Ghanshyam Das Gupta, Amrita Singh
Pharmacological Research.2022; 182: 106358. CrossRef - Endurance Training Improves GLP-1 Sensitivity and Glucose Tolerance in Overweight Women
Thorbjörn Åkerström, Malene N Stolpe, Renate Widmer, Thomas F Dejgaard, Jens M Højberg, Kirsten Møller, Jakob S Hansen, Beckey Trinh, Jens J Holst, Carsten Thomsen, Bente K Pedersen, Helga Ellingsgaard
Journal of the Endocrine Society.2022;[Epub] CrossRef - Assessing related factors to fasting blood sugar and glycosylated hemoglobin in patients with type 2 diabetes simultaneously by a multivariate longitudinal marginal model
Samaneh Hosseinzadeh, Zahra Khatirnamani, Enayatollah Bakhshi, Alireza Heidari, Arash Naghipour
Scientific Reports.2022;[Epub] CrossRef - Adherence to aerobic and muscle-strengthening components of the physical activity guidelines and mental health
Stephen Shannon, Angela Carlin, Catherine Woods, Alan M Nevill, Niamh Murphy, Marie H Murphy
Health Promotion International.2022;[Epub] CrossRef - Physical activity interventions for glycaemic control in African adults – A systematic review and meta-analysis
Chythra R. Rao, Baskaran Chandrasekaran, N. Ravishankar, Elizeus Rutebemberwa, David Okello
Diabetes & Metabolic Syndrome: Clinical Research & Reviews.2022; 16(12): 102663. CrossRef - The effect of acute aerobic exercise on central arterial stiffness, wave reflections, and hemodynamics in adults with diabetes: A randomized cross-over design
Kimberley L. Way, Angela S. Lee, Stephen M. Twigg, Nathan A. Johnson
Journal of Sport and Health Science.2021; 10(4): 499. CrossRef - Resistance training attenuates circulating FGF‐21 and myostatin and improves insulin resistance in elderly men with and without type 2 diabetes mellitus: A randomised controlled clinical trial
Fatemeh Shabkhiz, Mousa Khalafi, Sara Rosenkranz, Pouran Karimi, Kamilia Moghadami
European Journal of Sport Science.2021; 21(4): 636. CrossRef - The interaction between metformin and physical activity on postprandial glucose and glucose kinetics: a randomised, clinical trial
Nanna S. Pilmark, Mark Lyngbæk, Laura Oberholzer, Ida Elkjær, Christina Petersen-Bønding, Katja Kofoed, Christoph Siebenmann, Katja Kellenberger, Gerrit van Hall, Julie Abildgaard, Helga Ellingsgaard, Carsten Lauridsen, Mathias Ried-Larsen, Bente K. Peder
Diabetologia.2021; 64(2): 397. CrossRef - Effects of structured Aerobic Exercise on selected clinical profiles of patients with type 2 diabetes mellitus: A systematic review with meta-analysis
NmachukwuIfeoma Ekechukwu, StellaUdumma Anwara, UkamakaGloria Mgbeojedo, OliveU Chijioke, OkechukwuSteven Onwukwe, UchechukwuAnthonia Ezugwu, EchezonaNelson Dominic Ekechukwu, IjeomaL Okoronkwo
International Journal of Medicine and Health Development.2021; 26(1): 17. CrossRef - Impact of acute exercise on immediate and following early post-exercise FGF-21 concentration in adults: systematic review and meta-analysis
Mousa Khalafi, Karim Azali Alamdari, Michael E. Symonds, Hadi Nobari, Jorge Carlos-Vivas
Hormones.2021; 20(1): 23. CrossRef - Diagnosis, prevention, and treatment of cardiovascular diseases in people with type 2 diabetes and prediabetes: a consensus statement jointly from the Japanese Circulation Society and the Japan Diabetes Society
Eiichi Araki, Atsushi Tanaka, Nobuya Inagaki, Hiroshi Ito, Kohjiro Ueki, Toyoaki Murohara, Kenjiro Imai, Masataka Sata, Takehiro Sugiyama, Hideki Ishii, Shunsuke Yamane, Takashi Kadowaki, Issei Komuro, Koichi Node
Diabetology International.2021; 12(1): 1. CrossRef - In silico study to quantify the effect of exercise on surface GLUT4 translocation in diabetes management
Darshna M. Joshi, Jignesh Patel, Hardik Bhatt
Network Modeling Analysis in Health Informatics and Bioinformatics.2021;[Epub] CrossRef - Stair climbing–descending exercise following meals improves 24-hour glucose excursions in people with type 2 diabetes
Hiroto Honda, Makoto Igaki, Motoaki Komatsu, Shin-ichiro Tanaka, Tetsuo Takaishi, Tatsuya Hayashi
The Journal of Physical Fitness and Sports Medicine.2021; 10(1): 51. CrossRef - Glycemic Control of Diabetes Mellitus Patients in Referral Hospitals of Amhara Region, Ethiopia: A Cross-Sectional Study
Berhanu Elfu Feleke, Teferi Elfu Feleke, Melkamu Beyene Kassahun, Wondemu Gebrekirose Adane, Netsanet Fentahun, Abel Girma, Alamirew Alebachew, Eyaya Misgan, Hanna Demelash Desyibelew, Mulat Tirfie Bayih, Omer Seid, Daniel Diaz
BioMed Research International.2021; 2021: 1. CrossRef - Influences of Recreational Tennis-Playing Exercise Time on Cardiometabolic Health Parameters in Healthy Elderly: The ExAMIN AGE Study
Hsiao-Han Chao, Yi-Hung Liao, Chun-Chung Chou
International Journal of Environmental Research and Public Health.2021; 18(3): 1255. CrossRef - Hyperinsulinemia Induced Altered Insulin Signaling Pathway in Muscle of High Fat- and Carbohydrate-Fed Rats: Effect of Exercise
Anu Joseph, S. Parvathy, Koyikkal Karthikeya Varma, Raffaella Mastrocola
Journal of Diabetes Research.2021; 2021: 1. CrossRef - Metabolically healthy obese vs. Metabolic syndrome – The crosslink between nutritional exposure to bisphenols and physical exercise
Jessica Jones, Paul Reneau, Julia Matzenbacher dos Santos
Medical Hypotheses.2021; 149: 110542. CrossRef - The effects of different doses of exercise on pancreatic β-cell function in patients with newly diagnosed type 2 diabetes: study protocol for and rationale behind the “DOSE-EX” multi-arm parallel-group randomised clinical trial
Mark P. P. Lyngbaek, Grit E. Legaard, Sebastian L. Bennetsen, Camilla S. Feineis, Villads Rasmussen, Nana Moegelberg, Cecilie F. Brinkløv, Anette B. Nielsen, Katja S. Kofoed, Carsten A. Lauridsen, Caroline Ewertsen, Henrik E. Poulsen, Robin Christensen, G
Trials.2021;[Epub] CrossRef - Skeletal Muscle–Adipose Tissue–Tumor Axis: Molecular Mechanisms Linking Exercise Training in Prostate Cancer
Sílvia Rocha-Rodrigues, Andreia Matos, José Afonso, Miguel Mendes-Ferreira, Eduardo Abade, Eduardo Teixeira, Bruno Silva, Eugenia Murawska-Ciałowicz, Maria José Oliveira, Ricardo Ribeiro
International Journal of Molecular Sciences.2021; 22(9): 4469. CrossRef - Comparison between different types of exercise training in patients with type 2 diabetes mellitus: A systematic review and network metanalysis of randomized controlled trials
Edoardo Mannucci, Allegra Bonifazi, Matteo Monami
Nutrition, Metabolism and Cardiovascular Diseases.2021; 31(7): 1985. CrossRef - Effect of exercise on cardiometabolic health of adults with overweight or obesity: Focus on blood pressure, insulin resistance, and intrahepatic fat—A systematic review and meta‐analysis
Francesca Battista, Andrea Ermolao, Marleen A. van Baak, Kristine Beaulieu, John E. Blundell, Luca Busetto, Eliana V. Carraça, Jorge Encantado, Dror Dicker, Nathalie Farpour‐Lambert, Adriyan Pramono, Alice Bellicha, Jean‐Michel Oppert
Obesity Reviews.2021;[Epub] CrossRef - The Multi-Domain Intervention Trial in Older Adults With Diabetes Mellitus for Prevention of Dementia in Japan: Study Protocol for a Multi-Center, Randomized, 18-Month Controlled Trial
Taiki Sugimoto, Atsushi Araki, Hiroki Fujita, Keiko Honda, Nobuya Inagaki, Takeshi Ishida, Junichi Kato, Minoru Kishi, Kazuki Kobayashi, Kunichi Kouyama, Hisashi Noma, Mitsuru Ohishi, Noriko Satoh-Asahara, Hiroyuki Shimada, Kazuhiro Sugimoto, Susumu Suzuk
Frontiers in Aging Neuroscience.2021;[Epub] CrossRef - Interactive effects of acute exercise and carbohydrate-energy replacement on insulin sensitivity in healthy adults
Drusus A. Johnson-Bonson, Benjamin J. Narang, Russell G. Davies, Aaron Hengist, Harry A. Smith, Jonathan D. Watkins, Harry Taylor, Jean-Philippe Walhin, Javier T. Gonzalez, James A. Betts
Applied Physiology, Nutrition, and Metabolism.2021; 46(10): 1207. CrossRef - The importance of physical activity in management of type 2 diabetes and COVID-19
Samuel Seidu, Kamlesh Khunti, Tom Yates, Abdullah Almaqhawi, M.J. Davies, Jack Sargeant
Therapeutic Advances in Endocrinology and Metabolism.2021; 12: 204201882110546. CrossRef - Appraisal of Triglyceride-Related Markers as Early Predictors of Metabolic Outcomes in the PREVIEW Lifestyle Intervention: A Controlled Post-hoc Trial
Santiago Navas-Carretero, Rodrigo San-Cristobal, Pia Siig Vestentoft, Jennie C. Brand-Miller, Elli Jalo, Margriet Westerterp-Plantenga, Elizabeth J. Simpson, Teodora Handjieva-Darlenska, Gareth Stratton, Maija Huttunen-Lenz, Tony Lam, Roslyn Muirhead, Sal
Frontiers in Nutrition.2021;[Epub] CrossRef - Insulin Resistance Remission Following Laparoscopic Roux-en-Y Gastric Bypass and Laparoscopic Sleeve Gastrectomy in Chinese Type 2 Diabetes Mellitus Patients With a Body Mass Index of 27.5–32.5 kg/m2
Ping Luo, Yaoquan Cao, Pengzhou Li, Guohui Wang, Zhi Song, Weizheng Li, Zhihong Su, Hui Zhou, Xianhao Yi, Zhibing Fu, Xulong Sun, Haibo Tang, Beibei Cui, Qianqian Yu, Liyong Zhu, Shaihong Zhu
Frontiers in Physiology.2021;[Epub] CrossRef - Effects of Metronidazole as an Adjunct to Non-Surgical Periodontal Therapy on Insulin Resistance in Type 2 Diabetics
Ambrina Qureshi, Zeba Haque, Hina Qureshi, Waqas Ahmed Farooqui
Antibiotics.2021; 10(11): 1400. CrossRef - Exercise Training Combined with Calanus Oil Supplementation Improves the Central Cardiodynamic Function in Older Women
Marek Štěpán, Klára Daďová, Miloš Matouš, Eva Krauzová, Lenka Sontáková, Michal Koc, Terje Larsen, Ondrej Kuda, Vladimír Štich, Lenka Rossmeislová, Michaela Šiklová
Nutrients.2021; 14(1): 149. CrossRef - Effectiveness of combined exercise in people with type 2 diabetes and concurrent overweight/obesity: a systematic review and meta-analysis
Xiaoyan Zhao, Qianyu He, Yongmei Zeng, Li Cheng
BMJ Open.2021; 11(10): e046252. CrossRef - Type 2 Diabetes Remission and Lifestyle Medicine: A Position Statement From the American College of Lifestyle Medicine
John Kelly, Micaela Karlsen, Gregory Steinke
American Journal of Lifestyle Medicine.2020; 14(4): 406. CrossRef - Combined Aerobic and Resistance Exercise Training Reduces Circulating Apolipoprotein J Levels and Improves Insulin Resistance in Postmenopausal Diabetic Women
Yun Kyung Jeon, Sang Soo Kim, Jong Ho Kim, Hyun Jeong Kim, Hyun Jun Kim, Jang Jun Park, Yuen Suk Cho, So Hee Joung, Ji Ryang Kim, Bo Hyun Kim, Sang Heon Song, In Joo Kim, Yong Ki Kim, Young-Bum Kim
Diabetes & Metabolism Journal.2020; 44(1): 103. CrossRef - The effect of low-volume high-intensity interval training on cardiovascular health outcomes in type 2 diabetes: A randomised controlled trial
Kimberley L. Way, Angelo Sabag, Rachelle N. Sultana, Michael K. Baker, Shelley E. Keating, Sean Lanting, James Gerofi, Vivienne H. Chuter, Ian D. Caterson, Stephen M. Twigg, Nathan A. Johnson
International Journal of Cardiology.2020; 320: 148. CrossRef - Effects of IL-6 Signaling Pathway Inhibition on Weight and BMI: A Systematic Review and Meta-Analysis
Olivia Patsalos, Bethan Dalton, Hubertus Himmerich
International Journal of Molecular Sciences.2020; 21(17): 6290. CrossRef - Non-Dietary Factors Associated with Glycemic Status among Adults Diagnosed with Type 2 Diabetes Mellitus in Malawi
Getrude Mphwanthe, Dave Weatherspoon, Alexander Kalimbira, Lorraine Weatherspoon
Social Work in Public Health.2020; 35(6): 380. CrossRef - The impact of high‐intensity interval training on inflammatory markers in metabolic disorders: A meta‐analysis
Mousa Khalafi, Michael E. Symonds
Scandinavian Journal of Medicine & Science in Sports.2020; 30(11): 2020. CrossRef - Effectiveness of martial arts exercise on anthropometric and body composition parameters of overweight and obese subjects: a systematic review and meta-analysis
Fabricio de Souza, Felipe Nunes Lanzendorf, Márcia Mendonça Marcos de Souza, Fabiana Schuelter-Trevisol, Daisson José Trevisol
BMC Public Health.2020;[Epub] CrossRef - Optimal Human Functioning Requires Exercise Across the Lifespan: Mobility in a 1g Environment Is Intrinsic to the Integrity of Multiple Biological Systems
David A. Hart, Ronald F. Zernicke
Frontiers in Physiology.2020;[Epub] CrossRef - Managing NAFLD in Type 2 Diabetes: The Effect of Lifestyle Interventions, a Narrative Review
Siôn A. Parry, Leanne Hodson
Advances in Therapy.2020; 37(4): 1381. CrossRef - Excess Accumulation of Lipid Impairs Insulin Sensitivity in Skeletal Muscle
Sung Sup Park, Young-Kyo Seo
International Journal of Molecular Sciences.2020; 21(6): 1949. CrossRef - The Effect of Resistance Exercise Intensity on Acute Hyperglycemia in Young Adult Males
Evan E. Schick, Luis E. Segura, Shayán Emamjomeh, Joshua A. Cotter
Sports.2020; 8(9): 121. CrossRef - Drop-out ratio between moderate to high-intensity physical exercise treatment by patients with, or at risk of, type 2 diabetes mellitus: A systematic review and meta-analysis
Guillem Jabardo-Camprubí, Rafel Donat-Roca, Mercè Sitjà-Rabert, Raimon Milà-Villarroel, Judit Bort-Roig
Physiology & Behavior.2020; 215: 112786. CrossRef - Effects of an intensive lifestyle intervention on the underlying mechanisms of improved glycaemic control in individuals with type 2 diabetes: a secondary analysis of a randomised clinical trial
Mette Y. Johansen, Kristian Karstoft, Christopher S. MacDonald, Katrine B. Hansen, Helga Ellingsgaard, Bolette Hartmann, Nicolai J. Wewer Albrechtsen, Allan A. Vaag, Jens J. Holst, Bente K. Pedersen, Mathias Ried-Larsen
Diabetologia.2020; 63(11): 2410. CrossRef - The effect of BPA exposure on insulin resistance and type 2 diabetes – The impact of muscle contraction
Madison Wade, Virginia Delawder, Paul Reneau, Julia M. dos Santos
Medical Hypotheses.2020; 140: 109675. CrossRef - Dynamic glucose disposal is driven by reduced endogenous glucose production in response to voluntary wheel running: a stable isotope approach
Timothy D. Allerton, Greg M. Kowalski, Hardy Hang, Jacqueline Stephens
American Journal of Physiology-Endocrinology and Metabolism.2020; 319(1): E2. CrossRef Antidiabetic Effects of Physical Activity: How It Helps to Control Type 2 Diabetes
Addisu Dabi Wake
Diabetes, Metabolic Syndrome and Obesity: Targets and Therapy.2020; Volume 13: 2909. CrossRef- The effect of endurance training with crocin consumption on the levels of MFN2 and DRP1 gene expression and glucose and insulin indices in the muscle tissue of diabetic rats
Abdolnabi Peyravi, Nasrin Yazdanpanahi, Hashem Nayeri, Seyyed Ali Hosseini
Journal of Food Biochemistry.2020;[Epub] CrossRef - Evidence for Training-Induced Changes in miRNA Levels in the Skeletal Muscle of Patients With Type 2 Diabetes Mellitus
Sarah Simaitis, Benedikt Schulte-Körne, Thorsten Schiffer, Wilhelm Bloch, Hans-Georg Predel, Klara Brixius, Christian Brinkmann
Frontiers in Physiology.2020;[Epub] CrossRef - Metabolic diseases affect male reproduction and induce signatures in gametes that may compromise the offspring health
Sara C Pereira, Luís Crisóstomo, Mário Sousa, Pedro F Oliveira, Marco G Alves, Caroline Burson
Environmental Epigenetics.2020;[Epub] CrossRef - Different mr-proANP-release in High Volume High Intensity Interval Exercise and Continuous Exercise Regimens with Matched Mean Intensity: A Cross-over Design Study
Julian Eigendorf
Exercise Medicine.2020; 4: 5. CrossRef - Diagnosis, Prevention, and Treatment of Cardiovascular Diseases in People With Type 2 Diabetes and Prediabetes ― A Consensus Statement Jointly From the Japanese Circulation Society and the Japan Diabetes Society ―
Eiichi Araki, Atsushi Tanaka, Nobuya Inagaki, Hiroshi Ito, Kohjiro Ueki, Toyoaki Murohara, Kenjiro Imai, Masataka Sata, Takehiro Sugiyama, Hideki Ishii, Shunsuke Yamane, Takashi Kadowaki, Issei Komuro, Koichi Node
Circulation Journal.2020; 85(1): 82. CrossRef - Aerobic training reduces immune cell recruitment and cytokine levels in adipose tissue in obese mice
Débora Romualdo Lacerda, Michele Macedo Moraes, Albená Nunes-Silva, Kátia Anunciação Costa, Débora Fernandes Rodrigues, Josiana Lopes Sabino, Letícia Maria de Souza Cordeiro, Vanessa Pinho, Mauro Martins Teixeira, Samuel Penna Wanner, Danusa Dias Soares,
Applied Physiology, Nutrition, and Metabolism.2019; 44(5): 512. CrossRef - Pharmacologic and Exercise Considerations in Older Adults With Diabetes
Susan L. Wenker, Denise L. Walbrandt Pigarelli
Topics in Geriatric Rehabilitation.2019; 35(1): 31. CrossRef - Human skeletal muscle macrophages increase following cycle training and are associated with adaptations that may facilitate growth
R. Grace Walton, Kate Kosmac, Jyothi Mula, Christopher S. Fry, Bailey D. Peck, Jason S. Groshong, Brian S. Finlin, Beibei Zhu, Philip A. Kern, Charlotte A. Peterson
Scientific Reports.2019;[Epub] CrossRef - An evidence‐based approach to developing low‐carbohydrate diets for type 2 diabetes management: A systematic review of interventions and methods
Jessica Turton, Grant D. Brinkworth, Rowena Field, Helen Parker, Kieron Rooney
Diabetes, Obesity and Metabolism.2019; 21(11): 2513. CrossRef - Evaluation of the effect of insulin sensitivity-enhancing lifestyle- and dietary-related adjuncts on antidepressant treatment response: protocol for a systematic review and meta-analysis
Olaitan J. Jeremiah, Gráinne Cousins, Finbarr P. Leacy, Brian P. Kirby, Benedict K. Ryan
Systematic Reviews.2019;[Epub] CrossRef - Association Between Exercise and Treatment with Liraglutide in Obese Rats by Cafeteria Diet
Daiane Didek, Maiara Mikuska Cordeiro, João Lucas de Paula Xavier, Paulo Roberto Ribeiro, Thiago Rentz, Gilson Cesar Nobre Franco, Carla Cristine Kanunfre, Henriette Rosa de Oliveira Emilio, Dionízia Xavier Scomparin
Brazilian Archives of Biology and Technology.2019;[Epub] CrossRef - Long-term moderate intensity exercise alleviates myocardial fibrosis in type 2 diabetic rats via inhibitions of oxidative stress and TGF-β1/Smad pathway
Shi-Qiang Wang, Dan Li, Yang Yuan
The Journal of Physiological Sciences.2019; 69(6): 861. CrossRef - Low-Intensity Running and High-Intensity Swimming Exercises Differentially Improve Energy Metabolism in Mice With Mild Spinal Muscular Atrophy
Léo Houdebine, Domenico D’Amico, Jean Bastin, Farah Chali, Céline Desseille, Valentin Rumeau, Judy Soukkari, Carole Oudot, Thaïs Rouquet, Bruno Bariohay, Julien Roux, Delphine Sapaly, Laure Weill, Philippe Lopes, Fatima Djouadi, Cynthia Bezier, Frédéric C
Frontiers in Physiology.2019;[Epub] CrossRef - Moderate-to-Vigorous-Intensity Physical Activity Observed in People With Diabetes-Related Foot Ulcers Over a One-Week Period
Maggie Lee, Jaap J. van Netten, Helen Sheahan, Peter A. Lazzarini
Journal of Diabetes Science and Technology.2019; 13(5): 827. CrossRef - The effect of high Intensity interval training versus moderate intensity continuous training on arterial stiffness and 24 h blood pressure responses: A systematic review and meta-analysis
Kimberley L. Way, Rachelle N. Sultana, Angelo Sabag, Michael K. Baker, Nathan A. Johnson
Journal of Science and Medicine in Sport.2019; 22(4): 385. CrossRef - PPARG Pro12Ala Ala carriers exhibit greater improvements in peripheral insulin sensitivity in response to 12 weeks of aerobic exercise training
Martin Bæk Blond, Theresia Maria Schnurr, Mads Rosenkilde, Jonas Salling Quist, Anne Sofie Gram, Michala Holm Reichkendler, Pernille Landrock Auerbach, Pernille Nordby, Lene Theil Skovgaard, Rasmus Ribel-Madsen, Johanne Marie Justesen, Tuomas Oskari Kilpe
Physiological Genomics.2019; 51(6): 254. CrossRef - Physical Activity and Sports—Real Health Benefits: A Review with Insight into the Public Health of Sweden
Christer Malm, Johan Jakobsson, Andreas Isaksson
Sports.2019; 7(5): 127. CrossRef - Exercise and Inflammation
Llion Roberts, Katsuhiko Suzuki
Antioxidants.2019; 8(6): 155. CrossRef - Effects of a 12-week moderate-intensity exercise training on blood glucose response in patients with type 2 diabetes
Shang-Lin Chiang, Margaret McLean Heitkemper, Yi-Jen Hung, Wen-Chii Tzeng, Meei-Shyuan Lee, Chia-Huei Lin
Medicine.2019; 98(36): e16860. CrossRef - A influência do exercício físico na captação de glicose independente de insulina
Leonardo Soares de Albuquerque Barros, Camila da Cunha Nunes
HU Revista.2019; 45(1): 59. CrossRef - A pilot randomized controlled trial of 6-week combined exercise program on fasting insulin and fitness levels in individuals with spinal cord injury
Dong-Il Kim, J. Andrew Taylor, Can Ozan Tan, Hyuna Park, Ji Young Kim, Sang-Yong Park, Kyong-Mee Chung, Young-Hee Lee, Bum-Suk Lee, Justin Y. Jeon
European Spine Journal.2019; 28(5): 1082. CrossRef - Association between physical activity and diabetic complications among Bangladeshi type 2 diabetic patients
Mohammad Sadaat Bukht, Kazi Rumana Ahmed, Sahadat Hossain, Parisha Masud, Shuhana Sultana, Rasheda Khanam
Diabetes & Metabolic Syndrome: Clinical Research & Reviews.2019; 13(1): 806. CrossRef - Exercise and insulin resistance in type 2 diabetes mellitus: A systematic review and meta-analysis
A. Sampath Kumar, Arun G. Maiya, B.A. Shastry, K. Vaishali, N. Ravishankar, Animesh Hazari, Shubha Gundmi, Radhika Jadhav
Annals of Physical and Rehabilitation Medicine.2019; 62(2): 98. CrossRef - Ultra-performance liquid chromatography-mass spectrometry-based metabolomics reveals Huangqiliuyi decoction attenuates abnormal metabolism as a novel therapeutic opportunity for type 2 diabetes
Jiao Xu, Zhe-hui Jiang, Xiu-bo Liu, Yan Ma, Wei Ma, Ling Ma
RSC Advances.2019; 9(68): 39858. CrossRef - Importance of the Madras Diabetes Research Foundation-Indian Diabetes Risk Score (MDRF-IDRS) for mass screening of type 2 diabetes and its complications at primary health care centers of North India
Mohammad Mustufa Khan, Gyanendra Kumar Sonkar, Sangeeta Singh, Satyendra Kumar Sonkar
International Journal of Diabetes in Developing Countries.2019; 39(3): 419. CrossRef - Sugar in mind: Untangling a sweet and sour relationship beyond type 2 diabetes
Nicolas Cherbuin, Erin I. Walsh
Frontiers in Neuroendocrinology.2019; 54: 100769. CrossRef - Aerobic exercise training may improve nerve function in type 2 diabetes and pre‐diabetes: A systematic review
Yu Gu, Sarah M. Dennis, Matthew C. Kiernan, Alison R. Harmer
Diabetes/Metabolism Research and Reviews.2019;[Epub] CrossRef - Air Pollution Has a Significant Negative Impact on Intentional Efforts to Lose Weight: A Global Scale Analysis
Morena Ustulin, So Young Park, Sang Ouk Chin, Suk Chon, Jeong-taek Woo, Sang Youl Rhee
Diabetes & Metabolism Journal.2018; 42(4): 320. CrossRef - Non-pharmacological Treatment Options in the Management of Diabetes Mellitus
Arkiath V Raveendran
European Endocrinology.2018; 14(2): 31. CrossRef - Adaptation of Skeletal Muscles to Contractile Activity of Varying Duration and Intensity: The Role of PGC-1α
D. V. Popov
Biochemistry (Moscow).2018; 83(6): 613. CrossRef - High-intensity interval training versus continuous training on physiological and metabolic variables in prediabetes and type 2 diabetes: A meta-analysis
Angélica Trevisan De Nardi, Tainara Tolves, Thatiane Larissa Lenzi, Luis Ulisses Signori, Antônio Marcos Vargas da Silva
Diabetes Research and Clinical Practice.2018; 137: 149. CrossRef - Obstructive Sleep Apnea Syndrome, Objectively Measured Physical Activity and Exercise Training Interventions: A Systematic Review and Meta-Analysis
Monique Mendelson, Sébastien Bailly, Mathieu Marillier, Patrice Flore, Jean Christian Borel, Isabelle Vivodtzev, Stéphane Doutreleau, Samuel Verges, Renaud Tamisier, Jean-Louis Pépin
Frontiers in Neurology.2018;[Epub] CrossRef - Affective Adaptation to Repeated SIT and MICT Protocols in Insulin-Resistant Subjects
TIINA SAANIJOKI, LAURI NUMMENMAA, MIKKO KOIVUMÄKI, ELIISA LÖYTTYNIEMI, KARI K. KALLIOKOSKI, JARNA C. HANNUKAINEN
Medicine & Science in Sports & Exercise.2018; 50(1): 18. CrossRef - Aerobic training improves platelet function in type 2 diabetic patients: role of microRNA-130a and GPIIb
Atousa Akbarinia, Mehdi Kargarfard, Mahmood Naderi
Acta Diabetologica.2018; 55(9): 893. CrossRef - Physical activity: the key to cardiometabolic risk reduction in obstructive sleep apnoea
Monique Mendelson, Patrice Flore
European Respiratory Journal.2018; 52(4): 1801775. CrossRef - Potential effect of exercise in ameliorating insulin resistance at transcriptome level
Zhigang Hu, Lei Zhou, Tingting He
The Journal of Sports Medicine and Physical Fitness.2018;[Epub] CrossRef - The influence of physical activity on risk of cardiovascular disease in people who are obese but metabolically healthy
Shinje Moon, Chang-Myung Oh, Moon-Ki Choi, Yoo-Kyung Park, Sukyung Chun, Minkyung Choi, Jae Myung Yu, Hyung Joon Yoo, Pedro Tauler
PLOS ONE.2017; 12(9): e0185127. CrossRef - Exercise Metabolism in Nonobese Patients with Type 2 Diabetes Following the Acute Restoration of Normoglycaemia
Christopher J. Gaffney, Peter Mansell, Francis B. Stephens, Ian A. Macdonald, Kostas Tsintzas
Journal of Diabetes Research.2017; 2017: 1. CrossRef - Glucose effectiveness, but not insulin sensitivity, is improved after short-term interval training in individuals with type 2 diabetes mellitus: a controlled, randomised, crossover trial
Kristian Karstoft, Margaret A. Clark, Ida Jakobsen, Sine H. Knudsen, Gerrit van Hall, Bente K. Pedersen, Thomas P. J. Solomon
Diabetologia.2017; 60(12): 2432. CrossRef - Protectin DX ameliorates palmitate- or high-fat diet-induced insulin resistance and inflammation through an AMPK-PPARα-dependent pathway in mice
Tae Woo Jung, Hyoung-Chun Kim, A. M. Abd El-Aty, Ji Hoon Jeong
Scientific Reports.2017;[Epub] CrossRef - Arginine and aerobic training prevent endothelial and metabolic alterations in rats at high risk for the development of the metabolic syndrome
Renata F. Medeiros, Thaiane G. Gaique, Thais Bento-Bernardes, Raquel Kindlovits, Tamiris M. B. Gomes, Nadia Alice V. Motta, Fernanda Carla Brito, Caroline Fernandes-Santos, Karen J. Oliveira, Antonio Claudio L. Nóbrega
British Journal of Nutrition.2017; 118(1): 1. CrossRef - Effects of Exercise on Type 2 Diabetes Mellitus-Related Cognitive Impairment and Dementia
Michele Callisaya, Kazunori Nosaka
Journal of Alzheimer's Disease.2017; 59(2): 503. CrossRef - Study of Insulin Resistance in Women with Preeclampsia
Amit D Sonagra, Asmabi Makandar, Shivaleela M Biradar, Zahoorunissa Deba
Indian journal of Medical Biochemistry.2017; 21(2): 127. CrossRef
 PubReader
PubReader Cite
Cite- Figure
-
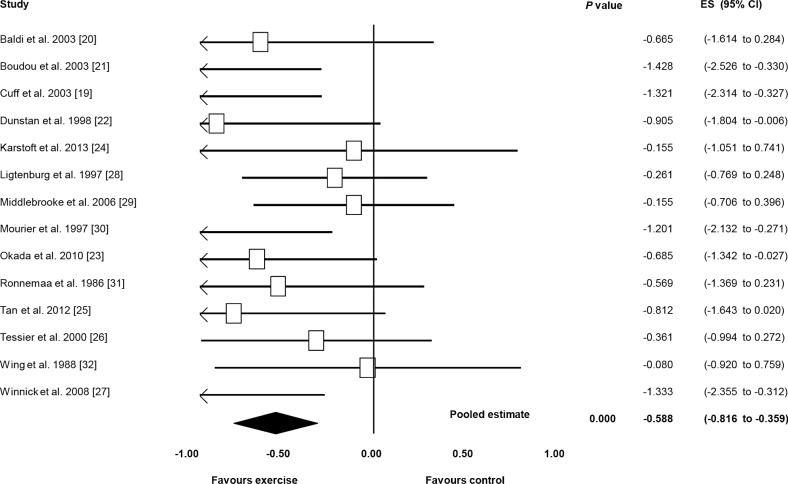
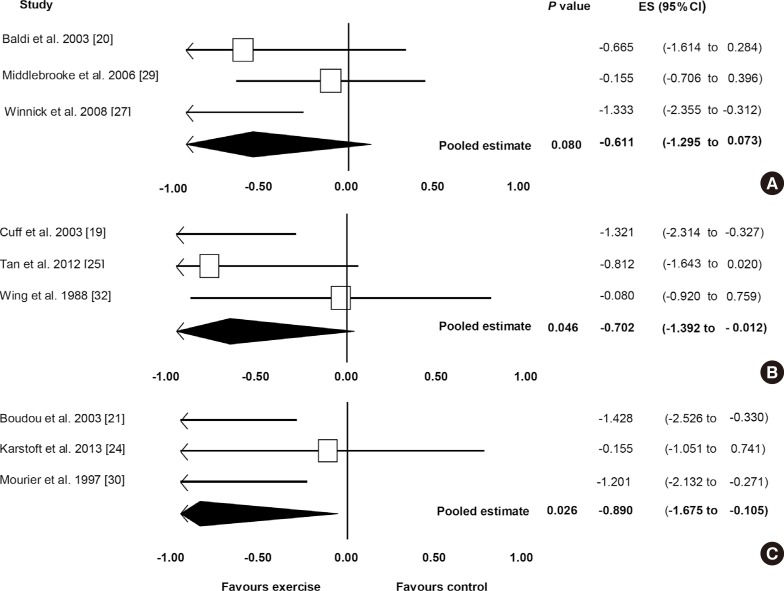
- Related articles
-
- Comparative Effect of Glucose-Lowering Drugs for Type 2 Diabetes Mellitus on Stroke Prevention: A Systematic Review and Network Meta-Analysis
- The Beneficial Effect of Glycemic Control against Adverse Outcomes in Patients with Type 2 Diabetes Mellitus and Chronic Kidney Disease
- Clinical Effects of a Home Care Pilot Program for Patients with Type 1 Diabetes Mellitus: A Retrospective Cohort Study
- Safety of COVID-19 Vaccines among Patients with Type 2 Diabetes Mellitus: Real-World Data Analysis
- Performance of Fast-Acting Aspart Insulin as Compared to Aspart Insulin in Insulin Pump for Managing Type 1 Diabetes Mellitus: A Meta-Analysis



