- Current
- Browse
- Collections
-
For contributors
- For Authors
- Instructions to authors
- Article processing charge
- e-submission
- For Reviewers
- Instructions for reviewers
- How to become a reviewer
- Best reviewers
- For Readers
- Readership
- Subscription
- Permission guidelines
- About
- Editorial policy
Articles
- Page Path
- HOME > Diabetes Metab J > Volume 39(2); 2015 > Article
-
ReviewComplication New Drugs for Treating Dyslipidemia: Beyond Statins
- Chang Ho Ahn, Sung Hee Choi
-
Diabetes & Metabolism Journal 2015;39(2):87-94.
DOI: https://doi.org/10.4093/dmj.2015.39.2.87
Published online: April 20, 2015
Department of Internal Medicine, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea.
- Corresponding author: Sung Hee Choi. Division of Endocrinology and Metabolism, Department of Internal Medicine, Seoul National University Bundang Hospital, Seoul National University College of Medicine, 82 Gumi-ro 173beon-gil, Bundang-gu, Seongnam 463-707, Korea. drshchoi@snu.ac.kr
Copyright © 2015 Korean Diabetes Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
- Statins have been shown to be very effective and safe in numerous randomized clinical trials, and became the implacable first-line treatment against atherogenic dyslipidemia. However, even with optimal statin treatment, 60% to 80% of residual cardiovascular risk still exists. The patients with familial hypercholesterolemia which results in extremely high level of low density lipoprotein cholesterol (LDL-C) level and the patients who are intolerant or unresponsive to statins are the other hurdles of statin treatment. Recently, new classes of lipid-lowering drugs have been developed and some of them are available for the clinical practice. The pro-protein convertase subtilisin/kexintype 9 (PCSK9) inhibitor increases the expression of low density lipoprotein (LDL) receptor in hepatocytes by enhancing LDL receptor recycling. The microsomal triglyceride transport protein (MTP) inhibitor and antisense oligonucleotide against apolipoprotein B (ApoB) reduce the ApoB containing lipoprotein by blocking the hepatic very low density lipoprotein synthesis pathway. The apolipoprotein A1 (ApoA1) mimetics pursuing the beneficial effect of high density lipoprotein cholesterol and can reverse the course of atherosclerosis. ApoA1 mimetics had many controversial clinical data and need more validation in humans. The PCSK9 inhibitor recently showed promising results of significant LDL-C lowering in familial hypercholesterolemia (FH) patients from the long-term phase III trials. The MTP inhibitor and antisesnse oligonucleotide against ApoB were approved for the treatment of homozygous FH but still needs more consolidated evidences about hepatic safety such as hepatosteatosis. We would discuss the benefits and concerns of these new lipid-lowering drugs anticipating additional benefits beyond statin treatment.
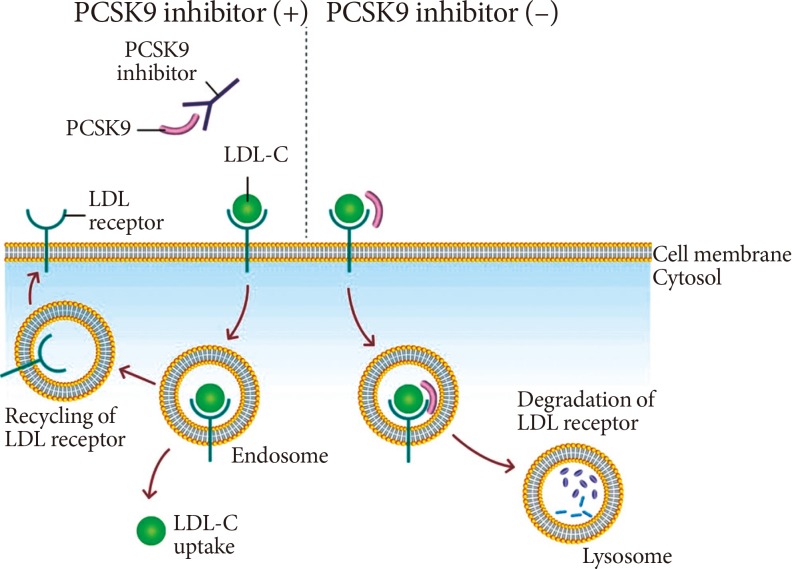
- Atherosclerotic cardiovascular disease (ASCVD) is the leading cause of death and major health care burden in worldwide regardless of different ethnicities. Dyslipidemia, characterized by high levels of atherogenic lipoproteins including low density lipoprotein cholesterol (LDL-C), is known as the major risk factor of ASCVD [1]. Statins, the 3-hydroxy-3-methylglutaryl-coenzyme A reductase inhibitor, efficiently block hepatic cholesterol synthesis and lower LDL-C sufficiently up to 50% from the baseline according to statin potency [2]. During the past few decades, statins have been the corner stone of the medical treatment of dyslipidemia. Statins reduce ASCVD risk by 15% to 37% (Fig. 1), but residual 60% to 80% of ASCVD risk still remains [3]. These remaining ASCVD risk has been considered as causing the major vascular event in about 20% of patients with coronary heart disease even under the optimal statin treatment [4].
- Familial hypercholesterolemia is a genetic disorder caused by a mutation in low density lipoprotein (LDL) receptor (LDLR) gene, apolipoprotein B (ApoB) gene or pro-protein convertase subtilisin/kexintype 9 (PCSK9) gene with the prevalence of 1 in 300 to 500 people for heterozygous form and 1 in 1,000,000 people for the more severe homozygous form [5]. These genetic defects cause the significant elevation of blood LDL-C levels, which result in the early development of ASCVD and in higher mortality [5]. High dose statins are the first choice of treatment for these patients, but even with maximal intensity of statin treatment only 20% of patients with familial hypercholesterolemia achieve optimal LDL-C goal [5]. Furthermore, a subset of patients is intolerant to high dose statin therapy due to adverse effects including myotoxicity or hepatotoxicity.
- Bile acid-binding resins, fibrates, niacin, and ezetimibe has been approved as non-statin agents for treating dyslipidemia [6]. Each class of non-statin drugs showed meaningful improvement of lipid profiles and especially has distinct effect in subtractions of blood lipoprotein composition such as elevating high density lipoprotein cholesterol (HDL-C) particles. However, none of these agents showed additional risk reduction of ASCVD when it is adding to the statin treatment. Only ezetimibe showed significant decrease of cardiovascular events from the recent randomized clinical trial: IMPROVE-IT, comparing simvastatin monotherapy and simvastatin plus ezetimibe combination [7].
- There have been consistent needs how we could optimize the treatment for patients with higher risk of ASCVD. Because there are still many percentage of patients exist to request new drug combination beyond statin treatment. In this review, we will discuss four newly developed drugs for treating dyslipidemia, PCSK9 inhibitor, microsomal triglyceride transport protein (MTP) inhibitor, apolipoprotein A1 (ApoA1) mimetics, and antisense oligonucleotide against ApoB including their mode of actions and the results of preclinical and clinical studies.
INTRODUCTION
- Mode of action
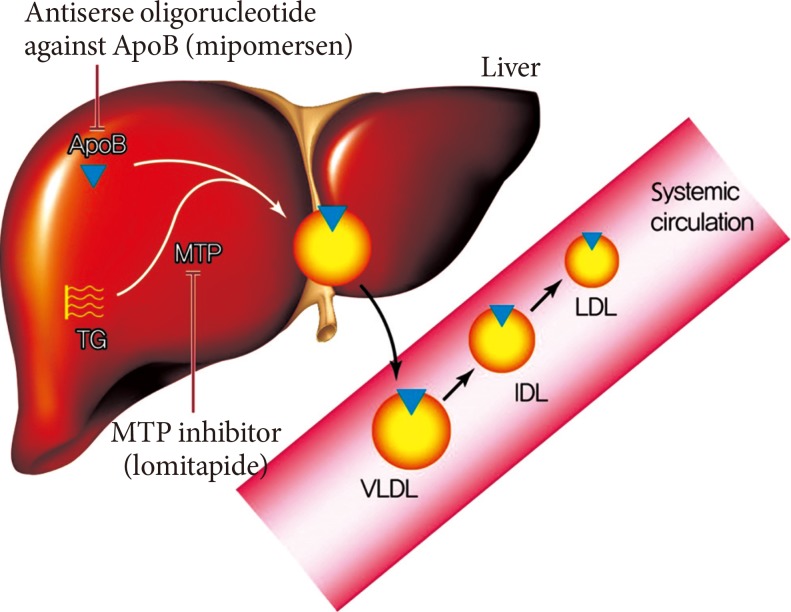
- PCSK9 is a serine protease that plays a central role in cholesterol metabolism in the liver by enhancing the degradation of LDLRs [8]. LDLR can be recycled or degraded in the lysosomal process after internalization. Circulating PCSK9 binds to the LDLRs directing the LDLRs to the lysosome, enhancing their clearance in the hepatocyte for degradation, and preventing the recycling of LDLRs back to the cell surface after internalization [9]. By blocking PCSK9, PCSK9 inhibitors can reduce LDLRs degradation and increase the surface expression of the LDLRs, which in turn enhances LDLRs recycling and reduces the LDL-C level (Fig. 2) [10]. Several approaches to inhibit PCSK9 have been proposed, including monoclonal antibody, small interfering RNA, antisense oligonucleotide, and mimetic peptides (Table 1) [11]. Among them, the fully humanized monoclonal antibody against PCSK9 showed successful human data by far [11].
- Preclinical study
- In mice with lacking PCSK9, the accumulation of cholesteryl esters in the lesion of aortic atherosclerosis was markedly reduced. By comparison, overexpression of PCSK9 induced an excess burden of atherosclerosis [12]. But in LDLR deficient mice, knock down or overexpression of PCSK9 had no significant effects on the cholesteryl ester accumulation and the size of atheromatous plaque. This study strongly suggests that the process by which PCSK9 enhances atherosclerosis is primarily mediated by its action on the LDLR [12]. Cloned guinea pigs created by transposition of a gain of function mutation of human PCSK9, a model for familial hypercholesterolemia, had a significant increase in aortic atherosclerosis compared with wild-type counterparts [13].
- Clinical study
- Among the various approaches to PCSK9 inhibition, the data for human studies are only available for monoclonal antibody against PCSK9. In phase II studies, the two most advanced monoclonal antibodies in development (alirocumab and evolocumab) decreased atherogenic lipoproteins very effectively and these drugs were well tolerated in human. In the clinical trial of 77 patients with heterozygous familial hypercholesterolemia, alirocumab reduced LDL-C by 29% to 43% for 150 to 300 mg injection at every 4 weeks and by 68% for 150 mg injection at every 2 weeks [14]. In addition, the higher dose of alirocumab, 150 mg every 2 weeks, showed significant increase in HDL-C and ApoA1 by 6.5% and 8.8%, respectively, as well as decrease in ApoB and non-HDL-C [14]. In the GAUSS trial which investigated the efficacy and safety of evolocumab in 160 statin-intolerant patients, evolocumab induced a significant dose-dependent decrease in LDL-C levels from 40.8% to 50.7% compared to baseline [15]. Furthermore, the combination of evolocumab and ezetimibe showed an almost 63% reduction in LDL-C. The result of a large phase III trial of alirocumab has been recently reported. In the trial involving 2,341 patients who were receiving maximum tolerated dose of statins, alirocumab reduced LDL-C by 62% compare to the baseline and the effect was maintained over 78 weeks of extended treatment [16]. Furthermore, in the post hoc analysis, alirocumab showed reduced rate of major adverse cardiovascular events compare to the placebo (hazard ratio, 0.52; 95% confidence interval, 0.31 to 0.90) [16]. The result of the long-term extension study of evolocumab trials also showed the consistent LDL-C reduction until 48 weeks of treatment and reduced cardiovascular events at approximately 1 year of treatment (hazard ratio, 0.47; 95% confidence interval, 0.28 to 0.78) [17].
PCSK9 INHIBITORS
- Mode of action
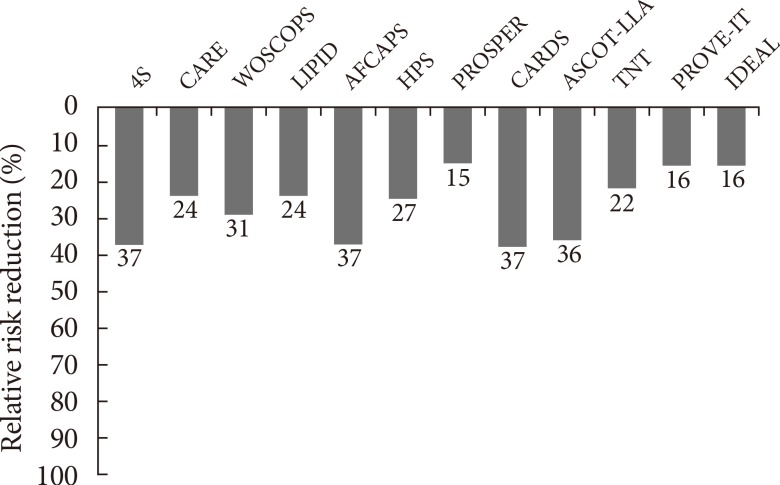
- MTP is predominantly expressed in hepatocytes and enterocytes, whose action is required in the synthesis of ApoB-containing lipoproteins. MTP transfers triglyceride (TG), phospholipids and cholesteryl esters to the ApoB in endoplasmic reticulum and has a critical role in the synthesis of very low density lipoprotein (VLDL) and chylomicrons in liver and intestine [18,19]. Inhibition of MTP results in the decreased synthesis and secretion of VLDL in the liver by inhibiting the lipidation of ApoB (Fig. 3) [20]. MTP inhibition can reverse the increased hepatic production and secretion of VLDLs caused by insulin resistance. Moreover, inhibition of MTP in enterocytes can contribute to the reduction in plasma TG level by reducing dietary fat absorption through chylomicron. An orally active small molecule inhibitor of MTP, lomitapide, was developed and it has been approved for the treatment of homozygous familial hypercholesterolemia [21].
- Preclinical study
- In an early study, treatment of hamsters with lomitapide for 7 days resulted in a dose-dependent reduction in both VLDL and LDL-C in the range of 19% to 89% and TGs in the range of 8% to 49% [22]. However, a concomitant decrease in HDL-C levels, particularly at higher doses, was noticed. The same study also investigated the efficacy of lomitapide in homozygous Watanabe-heritable hyperlipidemic rabbits as an atypical model of homozygous familial hypercholesterolemia. After the administration of lomitapide for 2 weeks, the ApoB-containing lipoprotein level was normalized [22]. The single-dose administration of lomitapide to the Zucker fatty rat, a genetic model of diabetic dyslipidemia and metabolic syndrome, reduced the serum level of TG by 35% and 47% at 0.3 and 1 mg/kg doses. Longer duration of treatment also showed significant decrease in the serum level of TG (71% to 87%), nonesterified fatty acids (33% to 40%), and LDL-C (26% to 29%) [23].
- Clinical study
- In a phase III trial of 29 homozygous familial hypercholesterolemia with mean baseline LDL-C of 336 mg/dL despite the previous lipid-lowering therapy, lomitapide decreased LDL-C by 50% at 26 weeks of treatment and 38% at 52 weeks of treatment [24]. The HDL-C levels were significantly reduced by 12% at 26 weeks, but returned to the pretreatment levels at 78 weeks [24]. Common adverse effects include diarrhea, nausea, and abdominal pain [4]. In the early phase clinical studies, lomitapide increased hepatic TG content in a dose dependent manner, presumably due to hepatic MTP inhibition [6] and trapping VLDLs in the liver. In the phase III trial, 10 patients showed elevation of hepatic enzyme and resolved with dose modification. Results from this study showed acceptable risk-to-benefit profile and lomitapide was approved for the treatment for homozygous familial hypercholesterolemia by US Food and Drug Administration (FDA) [21].
MTP INHIBITOR
- Mode of action
- ApoB is the major structural protein of atherogenic lipoproteins (APO-B containing lipoproteins). It has a key role in the assembly and secretion of VLDL from the liver [25]. Plasma ApoB concentration is a reliable index of the total number of atherogenic lipoproteins such as small dense LDL-C [25]. Mipomersen is a synthetic 20 nucleotide antisense oligonucleotide which can bind to ApoB mRNA via complementary sequence interactions [21]. Hybridization of mipomersen to the target ApoB mRNA creates a substrate for RNase H1, which results in the decrease of the ApoB mRNA level and the production of ApoB protein (Fig. 3) [21]. Two chemical modifications were made to the nucleotide structure of mipomersen. First, the internucleotide linkage was chemically modified as a phosphorothioated ester, which results in the resistance to the hydrolysis or degradation by nucleases and increase of binding to plasma protein to facilitate drug distribution and absorption. The second modification, insertion of methoxyethyl sugar residues into the first and last five positions made the mipomersen gave more stability and increased affinity [21,25].
- Preclinical study
- Including various animal studies such as mouse, hamster, rabbit, and monkey, the species-specific antisense oligonucleotide against ApoB reduced hepatic ApoB-100 mRNA and protein level, as well as serum levels of ApoB, LDL-C, and total cholesterol, in a dosedependent manner [21]. After subcutaneous injection, mipomersen is readily absorbed and distributed to tissues with highest drug concentrations in the liver and kidney. Mipomersen is metabolized by nucleases and the plasma elimination half-life ranges from 1 to 2 months, which allows relatively infrequent dosing. The clinical dosing regimen for mipomersen is weekly [21].
- Clinical study
- For the subjects with mild dyslipidemia, 12 weeks treatment with mipomersen with doses of 50 to 400 mg every 3 weeks resulted in a dose-dependent reduction in ApoB and LDL-C by a maximum of 50% and 35%, respectively [26]. The efficacy of mipomersen therapy in patients with familial hypercholesterolemia was confirmed in several phase II and III trials. The phase III trial in 44 heterozygous familial hypercholesterolemia patients showed significant reductions in ApoB and LDL-C with maximum reduction of 33% and 34%. In another phase III trial in homozygous familial hypercholesterolemia patients who is already receiving maximum tolerated dose of lipid-lowering therapy, 26 weeks treatment of mipomersen resulted in placebo adjusted reduction of ApoB and LDL-C by 24% and 21% [27]. From the result of this trial, mipomersen approved by US FDA for the treatment of homozygous familial hypercholesterolemia. Other clinical trials in patients with primary hypercholesterolemia also showed dose-dependent and consistent reduction of ApoB and LDL-C with treatment of mipomersen [28]. Frequent adverse effects associated with mipomersen are injection site reactions, flu-like symptoms and hepatic enzyme elevation. The major safety concern is increased hepatic accumulation of TG presumably due to impaired VLDLs secretion, which is very similar mechanism of TG trapping as in MTP inhibitor. The transaminase elevations are reversible with dose adjustment or even transient with continued treatment, and the hepatic fat increases occur early and are stable over time [21]. The long-term clinical consequences of increased hepatic TG are unknown. There is still concern for regular monitoring of hepatic function is requested in the patients receiving mipomersen [6].
ANTISENSE OLIGONUCLEOTIDE AGAINST APOLIPOPROTEIN B
- Mode of action
- The high serum level of HDL-C is a well-known protective factor of ASCVD [29]. ApoA1 is the major apolipoprotein component of mature HDL. ApoA1 took cholesterol from macrophages in atherosclerotic lesions via ATP-binding cassette A1 (ABCA1), triggering reverse cholesterol transport. The central role of ApoA1 in comprising HDL-C makes it as an attractive target for modifying ASCVD risk. ApoA1 mimetics are a class of drugs that is designed to mimic the effect of ApoA1 and HDL-C to reverse the progression of atherosclerosis [30].
- Preclinical study
- Several investigators have tested the effect of direct infusion of HDL or recombinant HDL with different ApoA1 preparations on atherosclerosis [31]. In the study of animal models, the infusion of HDL or recombinant HDL showed beneficial effect and even reversal of atherosclerosis, but they were difficult to be developed as a form of administrable drug [31].
- In 1980, Franceschini et al. [32] presented an ApoA1 variant called ApoA1 Milano among three Italian individuals with long lifespans and low atherosclerotic burden, despite low HDL levels and increased TGs. This genetic variant has a characteristic arginine to cysteine substitution, which allows for the formation of ApoA1 dimers [33]. The recombinant ApoA1 Milano, ETC-216, was created by combining the mutant HDL with phospholipids to create an HDL-like particle. The efficacy of ETC-216 was tested in cholesterol-fed carotid artery-injured rabbits. After two treatments, the lower doses of ETC-216 led to reduced lesion progression and the higher doses led to lesion regression and a significant reduction in markers associated with plaque instability [34].
- The preliminary success of ApoA1 Milano and recombinant HDL led to the development of a small ApoA1 mimetic peptide capable of oral administration without the need for weekly infusion therapy. This mimetic peptide, called D-4F, was synthesized from D-amino acids and was shown to decrease atherosclerotic lesion volume by 79% in LDLR-null mice, despite no change in plasma HDL [35]. Since its discovery, D-4F and its optical isomer L-4F have been shown to alter measures of cardiovascular disease in numerous animal models [36,37]. In vitro studies have shown that the mechanisms by which D-4F decreases atherosclerosis include increased cholesterol efflux from macrophages via ABCA1, increased transport of cholesterol to the liver via SR-B1, decreased monocyte chemotaxis and adhesion, and binding of oxidized lipids [38].
- Clinical study
- In a clinical study in patients with acute coronary syndrome, 5 weeks infusion of recombinant ApoA1 Milano decreased 4.2% of atheroma volume from baseline as measured by intravascular ultrasound [39]. Recombinant HDL containing normal human ApoA1 combined with phospholipid were also tested. In the ERASE (Effect of rHDL on Atherosclerosis Safety and Efficacy) study, patients with ACS received recombinant HDL (CSL-112) for 4 weeks, which resulted in no significant effect on atheroma or plaque volume compared with placebo [40]. However, compare to the baseline, the atheroma volume was significantly reduced by 3.4% [40]. In a phase I trial of small ApoA1 mimetic peptide, patients with coronary heart diseases received a single dose of D-4F, which resulted in a significantly improved HDL-inflammatory index relative to placebo [41]. L-4F showed the equal efficacy to D-4F when injected intravenously. However, Watson et al. [42] demonstrated that patients with CHD received intravenous L-4F over 7 days, showed no significant reduction in HDL-inflammatory index. Clearly, more preclinical and clinical studies including clinical trials of advanced phases are needed for ApoA1 mimetics. It is too early to make a conclusion on whether ApoA1 mimetics can be a clinically meaningful part of lipid-lowering treatment.
APOLIPOPROTEIN A1 MIMETICS
- Statin therapy is a touchstone in the treatment of dyslipidemia. From numerous randomized clinical trials, it has been shown to be safe and efficacious for preventing future cardiovascular events. However, still, significant amount of residual ASCVD risk is remaining even under optimal statin treatment and significant portion of patients are intolerant or unresponsive to statin therapy. Many researchers and pharmaceutical companies are involved in this field of fighting for atherogenic dyslipidemia and it have been many promising results coming to apply in real clinical settings.
- The PCSK9 inhibitor facilitates the uptake of LDL-C by enhancing LDLR recycling. It showed favorable effects for additional lowering of LDL-C when adding on to statin and nice safety profile with consistent long-term efficacy in large phase III trials. The MTP inhibitor and antisense oligonucleotide against ApoB are reducing ApoB-containing lipoprotein, the major atherogenic lipoprotein. Lomitapide, the MTP inhibitor, and mipomersen, the antisense oligonucleotides against ApoB, have shown their efficacy in lowering LDL-C in recent phase III trials and they were already approved for treating patients with homozygous familial hypercholesterolemia. Those two drugs are still in a major safety concern, which is increased hepatic fat accumulation as trapping TG due to their pharmacologic effect of inhibiting hepatic VLDL secretion. The long term safety profiles need to be evaluated in a near future. The ApoA1 mimetic is the most experimental class of drugs among four different classes in this review. It has been shown to alter or reverse the natural course of atherosclerosis despite the range of LDL-C level in preclinical studies. However, their efficacy seems to be modest and the results are not consistent from previous studies. It awaits further validation through various human studies.
- The new classes of drugs beyond statin could enlighten the improvement for anti-atherosclerosis therapy. Clinicians should keep their eyes on the results of upcoming studies using new class of drugs to find the best and the optimal treatment modality for patients with dyslipidemia.
CONCLUSIONS
-
CONFLICTS OF INTEREST: No potential conflict of interest relevant to this article was reported.
NOTES
- 1. Roh E, Ko SH, Kwon HS, Kim NH, Kim JH, Kim CS, Song KH, Won JC, Kim DJ, Choi SH, Lim S, Cha BY. Prevalence and Management of Dyslipidemia in Korea: Korea National Health and Nutrition Examination Survey during 1998 to 2010. Diabetes Metab J 2013;37:433-449. ArticlePubMedPMC
- 2. Koo BK. Statin for the primary prevention of cardiovascular disease in patients with diabetes mellitus. Diabetes Metab J 2014;38:32-34. ArticlePubMedPMC
- 3. Lim S, Park YM, Sakuma I, Koh KK. How to control residual cardiovascular risk despite statin treatment: focusing on HDL-cholesterol. Int J Cardiol 2013;166:8-14. ArticlePubMed
- 4. Sampson UK, Fazio S, Linton MF. Residual cardiovascular risk despite optimal LDL cholesterol reduction with statins: the evidence, etiology, and therapeutic challenges. Curr Atheroscler Rep 2012;14:1-10. ArticlePubMedPMCPDF
- 5. Hovingh GK, Davidson MH, Kastelein JJ, O'Connor AM. Diagnosis and treatment of familial hypercholesterolaemia. Eur Heart J 2013;34:962-971. ArticlePubMed
- 6. Ridker PM. LDL cholesterol: controversies and future therapeutic directions. Lancet 2014;384:607-617. ArticlePubMed
- 7. DiNicolantonio JJ, Chatterjee S, Lavie CJ, Bangalore S, O'Keefe JH. Ezetimibe plus moderate dose simvastatin after acute coronary syndrome: what are we IMPROVEing on? Am J Med Epub 2015 Feb 27. DOI: http://dx.doi.org/10.1016/j.amjmed.2015.01.034.Article
- 8. Abifadel M, Varret M, Rabes JP, Allard D, Ouguerram K, Devillers M, Cruaud C, Benjannet S, Wickham L, Erlich D, Derre A, Villeger L, Farnier M, Beucler I, Bruckert E, Chambaz J, Chanu B, Lecerf JM, Luc G, Moulin P, Weissenbach J, Prat A, Krempf M, Junien C, Seidah NG, Boileau C. Mutations in PCSK9 cause autosomal dominant hypercholesterolemia. Nat Genet 2003;34:154-156. ArticlePubMedPDF
- 9. Horton JD, Cohen JC, Hobbs HH. Molecular biology of PCSK9: its role in LDL metabolism. Trends Biochem Sci 2007;32:71-77. ArticlePubMedPMC
- 10. Do RQ, Vogel RA, Schwartz GG. PCSK9 Inhibitors: potential in cardiovascular therapeutics. Curr Cardiol Rep 2013;15:345ArticlePubMedPDF
- 11. Noto D, Cefalu AB, Averna MR. Beyond statins: new lipid lowering strategies to reduce cardiovascular risk. Curr Atheroscler Rep 2014;16:414ArticlePubMedPDF
- 12. Denis M, Marcinkiewicz J, Zaid A, Gauthier D, Poirier S, Lazure C, Seidah NG, Prat A. Gene inactivation of proprotein convertase subtilisin/kexin type 9 reduces atherosclerosis in mice. Circulation 2012;125:894-901. ArticlePubMed
- 13. Al-Mashhadi RH, Sorensen CB, Kragh PM, Christoffersen C, Mortensen MB, Tolbod LP, Thim T, Du Y, Li J, Liu Y, Moldt B, Schmidt M, Vajta G, Larsen T, Purup S, Bolund L, Nielsen LB, Callesen H, Falk E, Mikkelsen JG, Bentzon JF. Familial hypercholesterolemia and atherosclerosis in cloned minipigs created by DNA transposition of a human PCSK9 gain-of-function mutant. Sci Transl Med 2013;5:166ra1.ArticlePubMed
- 14. Stein EA, Gipe D, Bergeron J, Gaudet D, Weiss R, Dufour R, Wu R, Pordy R. Effect of a monoclonal antibody to PCSK9, REGN727/SAR236553, to reduce low-density lipoprotein cholesterol in patients with heterozygous familial hypercholesterolaemia on stable statin dose with or without ezetimibe therapy: a phase 2 randomised controlled trial. Lancet 2012;380:29-36. ArticlePubMed
- 15. Sullivan D, Olsson AG, Scott R, Kim JB, Xue A, Gebski V, Wasserman SM, Stein EA. Effect of a monoclonal antibody to PCSK9 on low-density lipoprotein cholesterol levels in statin-intolerant patients: the GAUSS randomized trial. JAMA 2012;308:2497-2506. ArticlePubMed
- 16. Robinson JG, Farnier M, Krempf M, Bergeron J, Luc G, Averna M, Stroes ES, Langslet G, Raal FJ, Shahawy ME, Koren MJ, Lepor NE, Lorenzato C, Pordy R, Chaudhari U, Kastelein JJ. Efficacy and Safety of Alirocumab in Reducing Lipids and Cardiovascular Events. N Engl J Med 2015.Article
- 17. Sabatine MS, Giugliano RP, Wiviott SD, Raal FJ, Blom DJ, Robinson J, Ballantyne CM, Somaratne R, Legg J, Wasserman SM, Scott R, Koren MJ, Stein EA. Efficacy and Safety of Evolocumab in Reducing Lipids and Cardiovascular Events. N Engl J Med 2015.Article
- 18. Choi SH, Ginsberg HN. Increased very low density lipoprotein (VLDL) secretion, hepatic steatosis, and insulin resistance. Trends Endocrinol Metab 2011;22:353-363. ArticlePubMedPMC
- 19. Wetterau JR, Aggerbeck LP, Bouma ME, Eisenberg C, Munck A, Hermier M, Schmitz J, Gay G, Rader DJ, Gregg RE. Absence of microsomal triglyceride transfer protein in individuals with abetalipoproteinemia. Science 1992;258:999-1001. ArticlePubMed
- 20. Cuchel M, Bloedon LT, Szapary PO, Kolansky DM, Wolfe ML, Sarkis A, Millar JS, Ikewaki K, Siegelman ES, Gregg RE, Rader DJ. Inhibition of microsomal triglyceride transfer protein in familial hypercholesterolemia. N Engl J Med 2007;356:148-156. ArticlePubMed
- 21. Rader DJ, Kastelein JJ. Lomitapide and mipomersen: two first-in-class drugs for reducing low-density lipoprotein cholesterol in patients with homozygous familial hypercholesterolemia. Circulation 2014;129:1022-1032. ArticlePubMed
- 22. Wetterau JR, Gregg RE, Harrity TW, Arbeeny C, Cap M, Connolly F, Chu CH, George RJ, Gordon DA, Jamil H, Jolibois KG, Kunselman LK, Lan SJ, Maccagnan TJ, Ricci B, Yan M, Young D, Chen Y, Fryszman OM, Logan JV, Musial CL, Poss MA, Robl JA, Simpkins LM, Slusarchyk WA, Sulsky R, Taunk P, Magnin DR, Tino JA, Lawrence RM, Dickson JK Jr, Biller SA. An MTP inhibitor that normalizes atherogenic lipoprotein levels in WHHL rabbits. Science 1998;282:751-754. ArticlePubMed
- 23. Dhote V, Joharapurkar A, Kshirsagar S, Dhanesha N, Patel V, Patel A, Raval S, Jain M. Inhibition of microsomal triglyceride transfer protein improves insulin sensitivity and reduces atherogenic risk in Zucker fatty rats. Clin Exp Pharmacol Physiol 2011;38:338-344. ArticlePubMed
- 24. Cuchel M, Meagher EA, du Toit, Blom DJ, Marais AD, Hegele RA, Averna MR, Sirtori CR, Shah PK, Gaudet D, Stefanutti C, Vigna GB, Du Plessis AM, Propert KJ, Sasiela WJ, Bloedon LT, Rader DJ. Phase 3 HoFH Lomitapide Study investigators. Efficacy and safety of a microsomal triglyceride transfer protein inhibitor in patients with homozygous familial hypercholesterolaemia: a single-arm, open-label, phase 3 study. Lancet 2013;381:40-46. ArticlePubMed
- 25. Sahebkar A, Watts GF. New therapies targeting apoB metabolism for high-risk patients with inherited dyslipidaemias: what can the clinician expect? Cardiovasc Drugs Ther 2013;27:559-567. ArticlePubMedPDF
- 26. Kastelein JJ, Wedel MK, Baker BF, Su J, Bradley JD, Yu RZ, Chuang E, Graham MJ, Crooke RM. Potent reduction of apolipoprotein B and low-density lipoprotein cholesterol by short-term administration of an antisense inhibitor of apolipoprotein B. Circulation 2006;114:1729-1735. ArticlePubMed
- 27. Akdim F, Visser ME, Tribble DL, Baker BF, Stroes ES, Yu R, Flaim JD, Su J, Stein EA, Kastelein JJ. Effect of mipomersen, an apolipoprotein B synthesis inhibitor, on low-density lipoprotein cholesterol in patients with familial hypercholesterolemia. Am J Cardiol 2010;105:1413-1419. ArticlePubMed
- 28. Akdim F, Tribble DL, Flaim JD, Yu R, Su J, Geary RS, Baker BF, Fuhr R, Wedel MK, Kastelein JJ. Efficacy of apolipoprotein B synthesis inhibition in subjects with mild-to-moderate hyperlipidaemia. Eur Heart J 2011;32:2650-2659. ArticlePubMed
- 29. Gordon T, Castelli WP, Hjortland MC, Kannel WB, Dawber TR. High density lipoprotein as a protective factor against coronary heart disease. The Framingham Study. Am J Med 1977;62:707-714. ArticlePubMed
- 30. Sherman CB, Peterson SJ, Frishman WH. Apolipoprotein A-I mimetic peptides: a potential new therapy for the prevention of atherosclerosis. Cardiol Rev 2010;18:141-147. PubMed
- 31. Smith JD. Apolipoprotein A-I and its mimetics for the treatment of atherosclerosis. Curr Opin Investig Drugs 2010;11:989-996.PubMedPMC
- 32. Franceschini G, Sirtori CR, Capurso A 2nd, Weisgraber KH, Mahley RW. A-IMilano apoprotein. Decreased high density lipoprotein cholesterol levels with significant lipoprotein modifications and without clinical atherosclerosis in an Italian family. J Clin Invest 1980;66:892-900. ArticlePubMedPMC
- 33. Gualandri V, Franceschini G, Sirtori CR, Gianfranceschi G, Orsini GB, Cerrone A, Menotti A. AIMilano apoprotein identification of the complete kindred and evidence of a dominant genetic transmission. Am J Hum Genet 1985;37:1083-1097. PubMedPMC
- 34. Parolini C, Marchesi M, Lorenzon P, Castano M, Balconi E, Miragoli L, Chaabane L, Morisetti A, Lorusso V, Martin BJ, Bisgaier CL, Krause B, Newton RS, Sirtori CR, Chiesa G. Dose-related effects of repeated ETC-216 (recombinant apolipoprotein A-I Milano/1-palmitoyl-2-oleoyl phosphatidylcholine complexes) administrations on rabbit lipid-rich soft plaques: in vivo assessment by intravascular ultrasound and magnetic resonance imaging. J Am Coll Cardiol 2008;51:1098-1103. PubMed
- 35. Navab M, Anantharamaiah GM, Hama S, Garber DW, Chaddha M, Hough G, Lallone R, Fogelman AM. Oral administration of an Apo A-I mimetic peptide synthesized from D-amino acids dramatically reduces atherosclerosis in mice independent of plasma cholesterol. Circulation 2002;105:290-292. ArticlePubMed
- 36. Li X, Chyu KY, Faria Neto JR, Yano J, Nathwani N, Ferreira C, Dimayuga PC, Cercek B, Kaul S, Shah PK. Differential effects of apolipoprotein A-I-mimetic peptide on evolving and established atherosclerosis in apolipoprotein E-null mice. Circulation 2004;110:1701-1705. ArticlePubMed
- 37. Morgantini C, Imaizumi S, Grijalva V, Navab M, Fogelman AM, Reddy ST. Apolipoprotein A-I mimetic peptides prevent atherosclerosis development and reduce plaque inflammation in a murine model of diabetes. Diabetes 2010;59:3223-3228. ArticlePubMedPMCPDF
- 38. Xie Q, Zhao SP, Li F. D-4F, an apolipoprotein A-I mimetic peptide, promotes cholesterol efflux from macrophages via ATP-binding cassette transporter A1. Tohoku J Exp Med 2010;220:223-228. ArticlePubMed
- 39. Nissen SE, Tsunoda T, Tuzcu EM, Schoenhagen P, Cooper CJ, Yasin M, Eaton GM, Lauer MA, Sheldon WS, Grines CL, Halpern S, Crowe T, Blankenship JC, Kerensky R. Effect of recombinant ApoA-I Milano on coronary atherosclerosis in patients with acute coronary syndromes: a randomized controlled trial. JAMA 2003;290:2292-2300. ArticlePubMed
- 40. Tardif JC, Gregoire J, L’Allier PL, Ibrahim R, Lesperance J, Heinonen TM, Kouz S, Berry C, Basser R, Lavoie MA, Guertin MC, Rodes-Cabau J. Effect of rHDL on Atherosclerosis-Safety and Efficacy (ERASE) Investigators. Effects of reconstituted high-density lipoprotein infusions on coronary atherosclerosis: a randomized controlled trial. JAMA 2007;297:1675-1682. ArticlePubMed
- 41. Bloedon LT, Dunbar R, Duffy D, Pinell-Salles P, Norris R, DeGroot BJ, Movva R, Navab M, Fogelman AM, Rader DJ. Safety, pharmacokinetics, and pharmacodynamics of oral apoA-I mimetic peptide D-4F in high-risk cardiovascular patients. J Lipid Res 2008;49:1344-1352. ArticlePubMedPMC
- 42. Watson CE, Weissbach N, Kjems L, Ayalasomayajula S, Zhang Y, Chang I, Navab M, Hama S, Hough G, Reddy ST, Soffer D, Rader DJ, Fogelman AM, Schecter A. Treatment of patients with cardiovascular disease with L-4F, an apo-A1 mimetic, did not improve select biomarkers of HDL function. J Lipid Res 2011;52:361-373. ArticlePubMedPMC
REFERENCES
Fig. 1
Residual risk for developing cardiovascular disease still remains despite proper range of low density lipoprotein cholesterol reduction: Results from many different statin trials. 4S, Scandinavian Simvastatin Survival Study; CARE, Cholesterol and Recurrent Events; WOSCOPS, West of Scotland Coronary Prevention Study; LIPID, Long-term Intervention with Pravastatin in Ischemic Disease; AFCAPS, Air Force/Texas Coronary Atherosclerosis Prevention Study; HPS, Heart Protection Study; PROSPER, Prospective Study of Pravastatin Elderly at Risk; CARDS, Collaborative Atorvastatin Diabetes Study; ASCOT-LLA, Anglo-Scandinavian Cardiac Outcomes Trial-Lipid-lowering Arm; TNT, Treating to New Targets; PROVE-IT, Pravastatin or Atorvastatin Evaluation and Infection Therapy; IDEAL, Incremental Decrease in End Points through Aggressive Lipid Lowering. Adapted from Lim et al., with permission from Elsevier [1].
Fig. 2
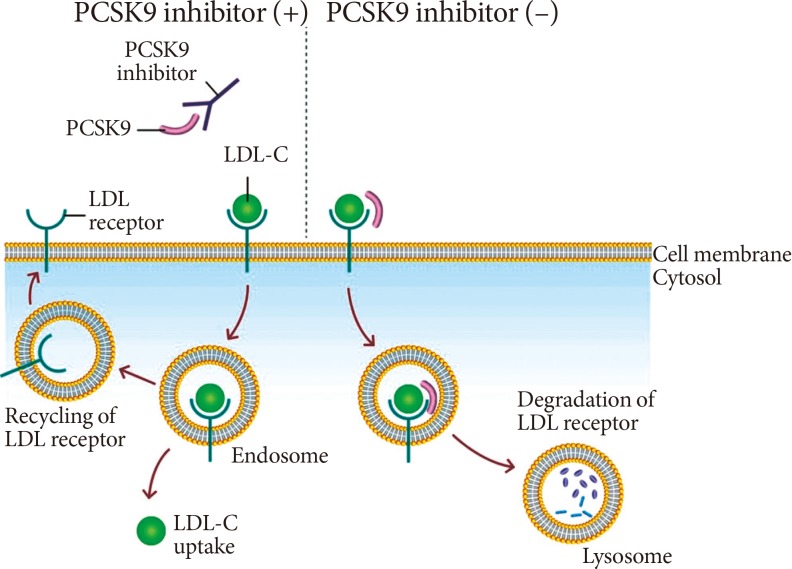
Therapeutic mechanism of pro-protein convertase subtilisin/kexin type 9 (PCSK9) inhibition. Binding of PCSK9 to the low density lipoprotein (LDL) receptor leads to the degradation of LDL receptor at lysosome. PCKS9 inhibitor, a monoclonal antibody against PCKS9, inhibits the binding of PCSK9 and LDL receptor, which results in the recycling of LDL receptor and increased expression of LDL receptor at cell membrane. LDL-C, low density lipoprotein cholesterol.
Fig. 3
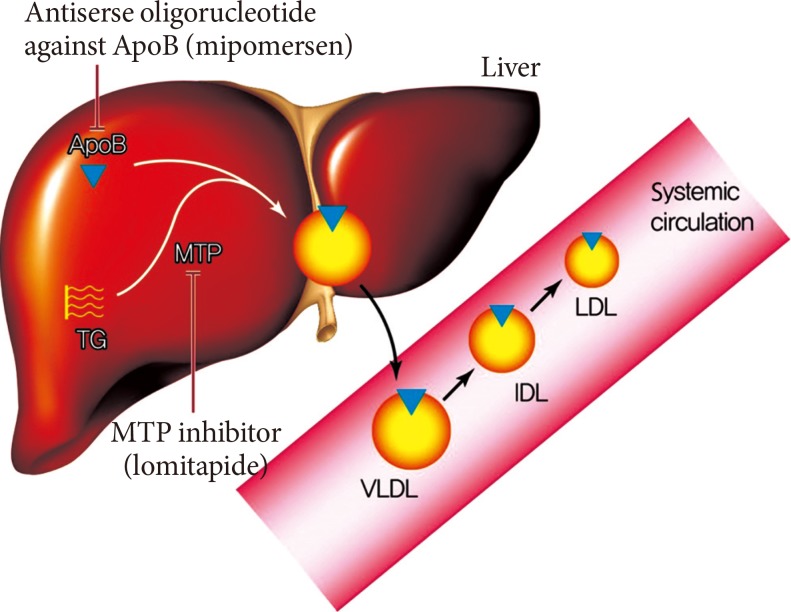
Therapeutic mechanism of lomitapide and mipomersen. The assembly of very low density lipoprotein (VLDL) requires the loading of triglyceride (TG) to the apolipoprotein B (ApoB) in the liver. The microsomal triglyceride transfer protein (MTP) works in this proccess and transfers TG to the ApoB. The secreted VLDL is converted to low density lipoprotein (LDL) in the bloodstream. The lomitapide inhibits the action of MTP and mipomersen inhibits the synthesis of ApoB. These two agents eventually inhibit the assembly of VLDL in the liver, which results in decreased LDL in the bloodstream. IDL, intermediate-density lipoprotein.
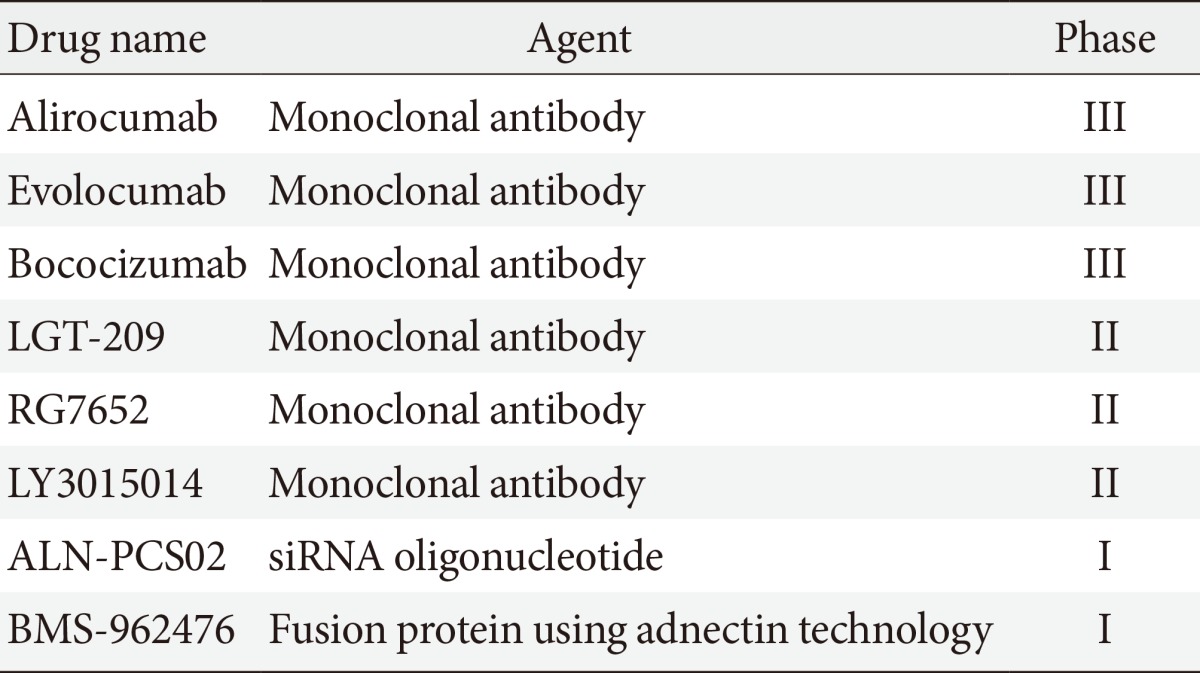
Figure & Data
References
Citations
Citations to this article as recorded by 
- Role of PCSK9 inhibitors in the management of dyslipidaemia
Tiny Nair
Indian Heart Journal.2024; 76: S44. CrossRef - Targeting Lipoprotein(a): Can RNA Therapeutics Provide the Next Step in the Prevention of Cardiovascular Disease?
Henriette Thau, Sebastian Neuber, Maximilian Y. Emmert, Timo Z. Nazari-Shafti
Cardiology and Therapy.2024; 13(1): 39. CrossRef - UHPLC Specific Method for Simultaneous Determination of Probable Impurities of Ezetimibeand Simvastatin in Combined Dosage Form
Anantha Lakshmi Vadivelu, Sathapathy Panduranga Vittal, Duvvuri Suryakala
Oriental Journal Of Chemistry.2024; 40(1): 228. CrossRef - LC‐MS based metabolite profiling, in‐vitro antioxidant and in‐vivo antihyperlipidemic activity of Nigella sativa extract
Amit Kumar Shrivastava, Laxmi Shrestha, Buddhi Raj Pokhrel, Bishal Joshi, Gopal Lamichhane, Bojana Vidović, Niranjan Koirala
eFood.2023;[Epub] CrossRef - Development of New Genome Editing Tools for the Treatment of Hyperlipidemia
Giulio Preta
Cells.2023; 12(20): 2466. CrossRef - High residual cardiovascular risk after lipid-lowering: prime time for Predictive, Preventive, Personalized, Participatory, and Psycho-cognitive medicine
E. Reijnders, A. van der Laarse, J. W. Jukema, C. M. Cobbaert
Frontiers in Cardiovascular Medicine.2023;[Epub] CrossRef - Riesgo residual. Conclusiones
Ángel Cequier, José Luis Zamorano
Revista Española de Cardiología Suplementos.2023; 23: 25. CrossRef - Anti-hyperglycemic, anti-hyperlipidemic, and anti-inflammatory effect of the drug Guggulutiktaka ghrita on high-fat diet-induced obese rats
Samreen M. Sheik, Pugazhandhi Bakthavatchalam, Revathi P. Shenoy, Basavaraj S. Hadapad, Deepak Nayak M, Monalisa Biswas, Varashree Bolar Suryakanth
Journal of Ayurveda and Integrative Medicine.2022; 13(3): 100583. CrossRef - New, Novel Lipid-Lowering Agents for Reducing Cardiovascular Risk: Beyond Statins
Kyuho Kim, Henry N. Ginsberg, Sung Hee Choi
Diabetes & Metabolism Journal.2022; 46(4): 517. CrossRef - A New Modality in Dyslipidemia Treatment: Antisense Oligonucleotide Therapy
Kyuho Kim, Sung Hee Choi
Journal of Lipid and Atherosclerosis.2022; 11(3): 250. CrossRef - Tyramine exerts hypolipidemic and anti-obesity effects in vivo
Thamires Maria Fontenele Morais, Tiago Sousa Melo, Mariana Brito Dantas, Jamile Magalhães Ferreira, Daniel Freire de Sousa, Emanuel Paula Magalhães, Ramon Róseo Paula Pessoa Bezerra de Menezes, Otília Deusdênia Loiola Pessoa, Mariana Lima Feitosa, Francis
Brazilian Journal of Pharmaceutical Sciences.2022;[Epub] CrossRef - Statin adherence and risk of all-cause, cancer, and cardiovascular mortality among dyslipidemia patients: A time-dependent analysis
Young Ran Lee, Sarah Soyeon Oh, Sung-In Jang, Eun-Cheol Park
Nutrition, Metabolism and Cardiovascular Diseases.2020; 30(12): 2207. CrossRef - Efficient reabsorption of transintestinally excreted cholesterol is a strong determinant for cholesterol disposal in mice
Ivo P. van de Peppel, Anna Bertolini, Theo H. van Dijk, Albert K. Groen, Johan W. Jonker, Henkjan J. Verkade
Journal of Lipid Research.2019; 60(9): 1562. CrossRef - Pharmacological Strategies beyond Statins: Ezetimibe and PCSK9 Inhibitors
Jah Yeon Choi, Jin Oh Na
Journal of Lipid and Atherosclerosis.2019; 8(2): 183. CrossRef - Effects of silymarin supplementation on blood lipids: A systematic review and meta‐analysis of clinical trials
Hamed Mohammadi, Amir Hadi, Arman Arab, Sajjad Moradi, Mohammad Hossein Rouhani
Phytotherapy Research.2019; 33(4): 871. CrossRef - Change in ALT levels after administration of HMG‐CoA reductase inhibitors to subjects with pretreatment levels three times the upper normal limit in clinical practice
Hyunah Kim, Hyeseon Lee, Tong Min Kim, So Jung Yang, Seo Yeon Baik, Seung‐Hwan Lee, Jae‐Hyoung Cho, Hyunyong Lee, Hyeon Woo Yim, In Young Choi, Kun‐Ho Yoon, Hun‐Sung Kim
Cardiovascular Therapeutics.2018;[Epub] CrossRef - Host-targeting therapies for hepatitis C virus infection: current developments and future applications
Emilie Crouchet, Florian Wrensch, Catherine Schuster, Mirjam B. Zeisel, Thomas F. Baumert
Therapeutic Advances in Gastroenterology.2018; 11: 175628481875948. CrossRef - New and Future Parenteral Therapies for the Management of Lipid Disorders
Roberto Garcia, Jaime Burkle
Archives of Medical Research.2018; 49(8): 538. CrossRef - NEW DRUGS FOR THE TREATMENT OF DYSLIPIDEMIA
Aleksandra Novaković, Marija Marinko, Ivan Stojanović, Dragoslav Nenezić, Predrag Milojević, Vladimir Kanjuh
Acta Medica Medianae.2018; 57(1): 54. CrossRef - Effects of diethylene glycol dibenzoate and Bisphenol A on the lipid metabolism of Danio rerio
Stefania Santangeli, Valentina Notarstefano, Francesca Maradonna, Elisabetta Giorgini, Giorgia Gioacchini, Isabel Forner-Piquer, Hamid R. Habibi, Oliana Carnevali
Science of The Total Environment.2018; 636: 641. CrossRef - Cardiac autonomic neuropathy: Risk factors, diagnosis and treatment
Victoria A Serhiyenko, Alexandr A Serhiyenko
World Journal of Diabetes.2018; 9(1): 1. CrossRef - Krüppel-like factor 14, a coronary artery disease associated transcription factor, inhibits endothelial inflammation via NF-κB signaling pathway
Wenting Hu, Haocheng Lu, Jifeng Zhang, Yanbo Fan, Ziyi Chang, Wenying Liang, Huilun Wang, Tianqing Zhu, Minerva T. Garcia-Barrio, Daoquan Peng, Y. Eugene Chen, Yanhong Guo
Atherosclerosis.2018; 278: 39. CrossRef - Strategies for the use of nonstatin therapies
Angela Pirillo, Giuseppe D. Norata, Alberico L. Catapano
Current Opinion in Lipidology.2017; 28(6): 458. CrossRef - The efficacy advantage of evolocumab (AMG 145) dosed at 140 mg every 2 weeks versus 420 mg every 4 weeks in patients with hypercholesterolemia: Evidence from a meta-analysis
Xiao-Xiao He, Rong Zhang, Pei-Yuan Zuo, Yu-Wei Liu, Xiang-Nan Zha, Sheng-Shuai Shan, Cheng-Yun Liu
European Journal of Internal Medicine.2017; 38: 52. CrossRef - The Potential Therapeutic Application of Peptides and Peptidomimetics in Cardiovascular Disease
Carlota Recio, Francesco Maione, Asif J. Iqbal, Nicola Mascolo, Vincenzo De Feo
Frontiers in Pharmacology.2017;[Epub] CrossRef - Emerging biologic therapies for hypercholesterolaemia
Giacomo Pucci, Arrigo F Cicero, Claudio Borghi, Giuseppe Schillaci
Expert Opinion on Biological Therapy.2017; 17(9): 1077. CrossRef - ANMCO/ISS/AMD/ANCE/ARCA/FADOI/GICR-IACPR/SICI-GISE/SIBioC/SIC/SICOA/SID/SIF/SIMEU/SIMG/SIMI/SISA Joint Consensus Document on cholesterol and cardiovascular risk: diagnostic–therapeutic pathway in Italy
Michele Massimo Gulizia, Furio Colivicchi, Gualtiero Ricciardi, Simona Giampaoli, Aldo Pietro Maggioni, Maurizio Averna, Maria Stella Graziani, Ferruccio Ceriotti, Alessandro Mugelli, Francesco Rossi, Gerardo Medea, Damiano Parretti, Maurizio Giuseppe Abr
European Heart Journal Supplements.2017; 19(suppl_D): D3. CrossRef - Rev-erb regulation of cholesterologenesis
Sadichha Sitaula, Jinsong Zhang, Fernanda Ruiz, Thomas P. Burris
Biochemical Pharmacology.2017; 131: 68. CrossRef - Novel lipid modifying drugs to lower LDL cholesterol
Arjen J. Cupido, Laurens F. Reeskamp, John J.P. Kastelein
Current Opinion in Lipidology.2017; 28(4): 367. CrossRef - 2017 Position Paper of the Italian Society for Cardiovascular Prevention (SIPREC) for an Updated Clinical Management of Hypercholesterolemia and Cardiovascular Risk: Executive Document
Massimo Volpe, Roberto Volpe, Giovanna Gallo, Vivianne Presta, Giuliano Tocci, Emanuela Folco, Andrea Peracino, Elena Tremoli, Bruno Trimarco
High Blood Pressure & Cardiovascular Prevention.2017; 24(3): 313. CrossRef - Sobetirome: the past, present and questions about the future
Jan Lammel Lindemann, Paul Webb
Expert Opinion on Therapeutic Targets.2016; 20(2): 145. CrossRef - Role of growth hormone-releasing hormone in dyslipidemia associated with experimental type 1 diabetes
Maritza J. Romero, Rudolf Lucas, Huijuan Dou, Supriya Sridhar, Istvan Czikora, Eby M. Mosieri, Ferenc G. Rick, Norman L. Block, Subbaramiah Sridhar, David Fulton, Neal L. Weintraub, Zsolt Bagi, Andrew V. Schally
Proceedings of the National Academy of Sciences.2016; 113(7): 1895. CrossRef - Recent trends in and new data on the epidemiology and prevention of non-communicable diseases
S. A. Boytsov
Terapevticheskii arkhiv.2016; 88(1): 4. CrossRef - Cellular Model of Atherogenesis Based on Pluripotent Vascular Wall Pericytes
Ekaterina A. Ivanova, Alexander N. Orekhov
Stem Cells International.2016; 2016: 1. CrossRef - Pre-treatment with simvastatin prevents the induction of diet-induced atherosclerosis in a rabbit model
Nikolaos Oikonomidis, Nikolaos Kavantzas, Laskarina-Maria Korou, Panagiotis Konstantopoulos, Vasilios Pergialiotis, Evangelos Misiakos, Ioannis Rizos, Christos Verikokos, Despina N. Perrea
Biomedical Reports.2016; 5(6): 667. CrossRef - Prevention of oxLDL uptake leads to decreased atherosclerosis in hematopoietic NPC1-deficient Ldlr−/− mice
Mike L.J. Jeurissen, Sofie M.A. Walenbergh, Tom Houben, Marion J.J. Gijbels, Jieyi Li, Tim Hendrikx, Yvonne Oligschlaeger, Patrick J. van Gorp, Christoph J. Binder, Marjo M.P.C. Donners, Ronit Shiri-Sverdlov
Atherosclerosis.2016; 255: 59. CrossRef
 PubReader
PubReader Cite
Cite