- Current
- Browse
- Collections
-
For contributors
- For Authors
- Instructions to authors
- Article processing charge
- e-submission
- For Reviewers
- Instructions for reviewers
- How to become a reviewer
- Best reviewers
- For Readers
- Readership
- Subscription
- Permission guidelines
- About
- Editorial policy
Articles
- Page Path
- HOME > Diabetes Metab J > Volume 48(2); 2024 > Article
-
Original ArticleCardiovascular Risk/Epidemiology Real-World Treatment Patterns according to Clinical Practice Guidelines in Patients with Type 2 Diabetes Mellitus and Established Cardiovascular Disease in Korea: Multicenter, Retrospective, Observational Study
-
Ye Seul Yang1*
 , Nam Hoon Kim2, Jong Ha Baek3, Seung-Hyun Ko4, Jang Won Son5, Seung-Hwan Lee6, Sang Youl Rhee7, Soo-Kyung Kim8, Tae Seo Sohn1, Ji Eun Jun9, In-Kyung Jeong9, Chong Hwa Kim10, Keeho Song11, Eun-Jung Rhee12, Junghyun Noh13, Kyu Yeon Hur14, Committee of Clinical Practice Guidelines, Korean Diabetes Association
, Nam Hoon Kim2, Jong Ha Baek3, Seung-Hyun Ko4, Jang Won Son5, Seung-Hwan Lee6, Sang Youl Rhee7, Soo-Kyung Kim8, Tae Seo Sohn1, Ji Eun Jun9, In-Kyung Jeong9, Chong Hwa Kim10, Keeho Song11, Eun-Jung Rhee12, Junghyun Noh13, Kyu Yeon Hur14, Committee of Clinical Practice Guidelines, Korean Diabetes Association -
Diabetes & Metabolism Journal 2024;48(2):279-289.
DOI: https://doi.org/10.4093/dmj.2023.0225
Published online: January 26, 2024
- 1,111 Views
- 150 Download
- 1 Crossref
1Division of Endocrinology and Metabolism, Department of Internal Medicine, Uijeongbu St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Uijeongbu, Korea
2Division of Endocrinology and Metabolism, Department of Internal Medicine, Korea University College of Medicine, Seoul, Korea
3Department of Internal Medicine, Gyeongsang National University Changwon Hospital, Gyeongsang National University College of Medicine, Changwon, Korea
4Division of Endocrinology and Metabolism, Department of Internal Medicine, St. Vincent’s Hospital, College of Medicine, The Catholic University of Korea, Suwon, Korea
5Division of Endocrinology and Metabolism, Department of Internal Medicine, Bucheon St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Bucheon, Korea
6Division of Endocrinology and Metabolism, Department of Internal Medicine, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
7Department of Endocrinology and Metabolism, Kyung Hee University Hospital, College of Medicine, Kyung Hee University, Seoul, Korea
8Division of Endocrinology and Metabolism, Department of Internal Medicine, CHA Bundang Medical Center, CHA University, Seongnam, Korea
9Division of Endocrinology and Metabolism, Department of Internal Medicine, Kyung Hee University Hospital at Gangdong, College of Medicine, Kyung Hee University, Seoul, Korea
10Division of Endocrinology and Metabolism, Department of Internal Medicine, Sejong General Hospital, Bucheon, Korea
11Division of Endocrinology and Metabolism, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul, Korea
12Division of Endocrinology and Metabolism, Department of Internal Medicine, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, Korea
13Division of Endocrinology and Metabolism, Department of Internal Medicine, Inje University Ilsan Paik Hospital, Inje University College of Medicine, Goyang, Korea
14Division of Endocrinology and Metabolism, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
-
Corresponding author: Kyu Yeon Hur Division of Endocrinology and Metabolism, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, 81 Irwon-ro, Gangnam-gu, Seoul 06351, Korea E-mail: hurky73@gmail.com
- *Current affiliation: Department of Medicine, Seoul National University College of Medicine, Seoul, Korea.
Copyright © 2024 Korean Diabetes Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Background
- Recent diabetes management guidelines recommend that sodium-glucose cotransporter 2 inhibitors (SGLT2is) or glucagon-like peptide 1 receptor agonists (GLP-1RAs) with proven cardiovascular benefits should be prioritized for combination therapy in patients with type 2 diabetes mellitus (T2DM) and established cardiovascular disease (CVD). This study was aimed at evaluating SGLT2i or GLP-1RA usage rates and various related factors in patients with T2DM and established CVD.
-
Methods
- We enrolled adults with T2DM aged ≥30 years who were hospitalized due to established CVD from January 2019 to May 2020 at 13 secondary and tertiary hospitals in Korea in this retrospective observational study.
-
Results
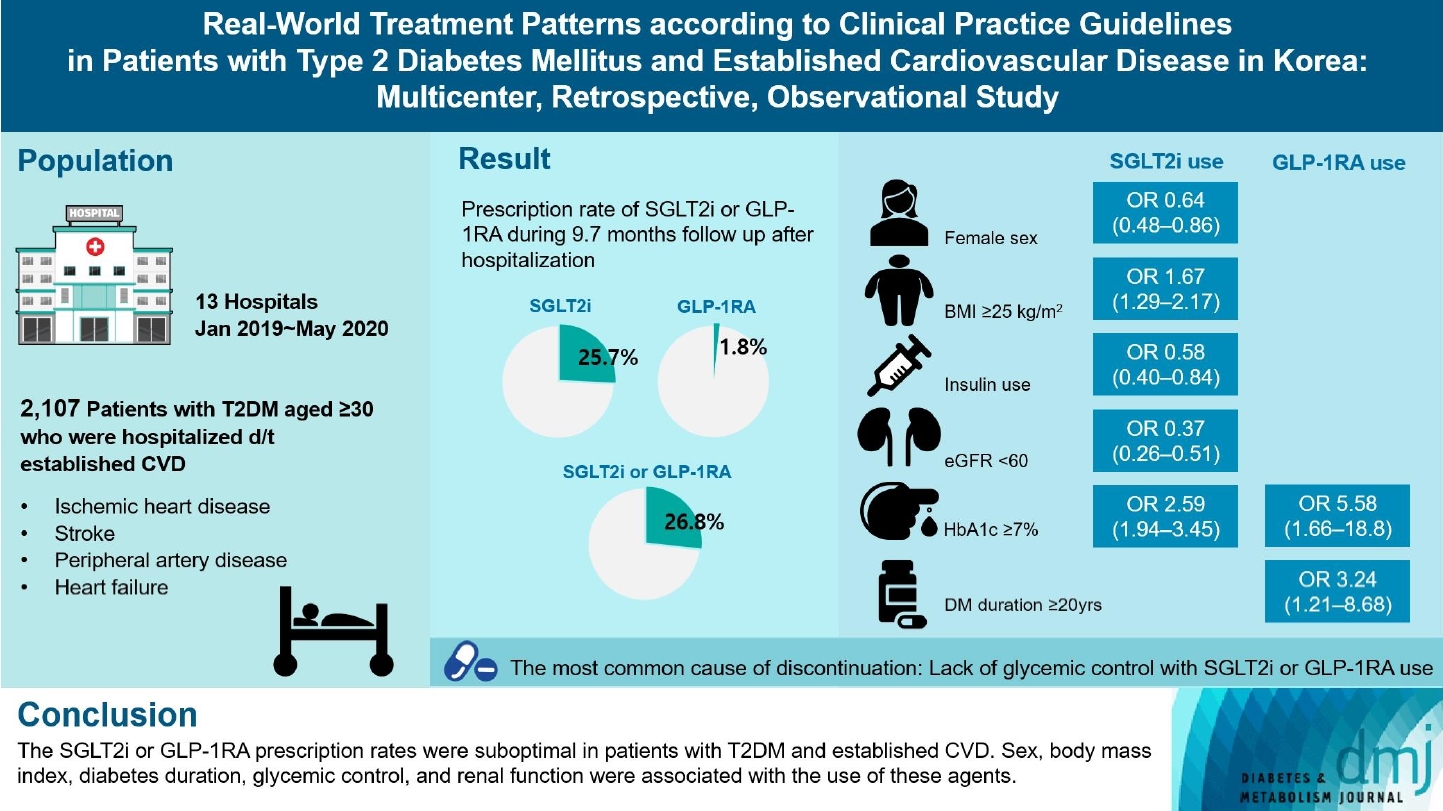
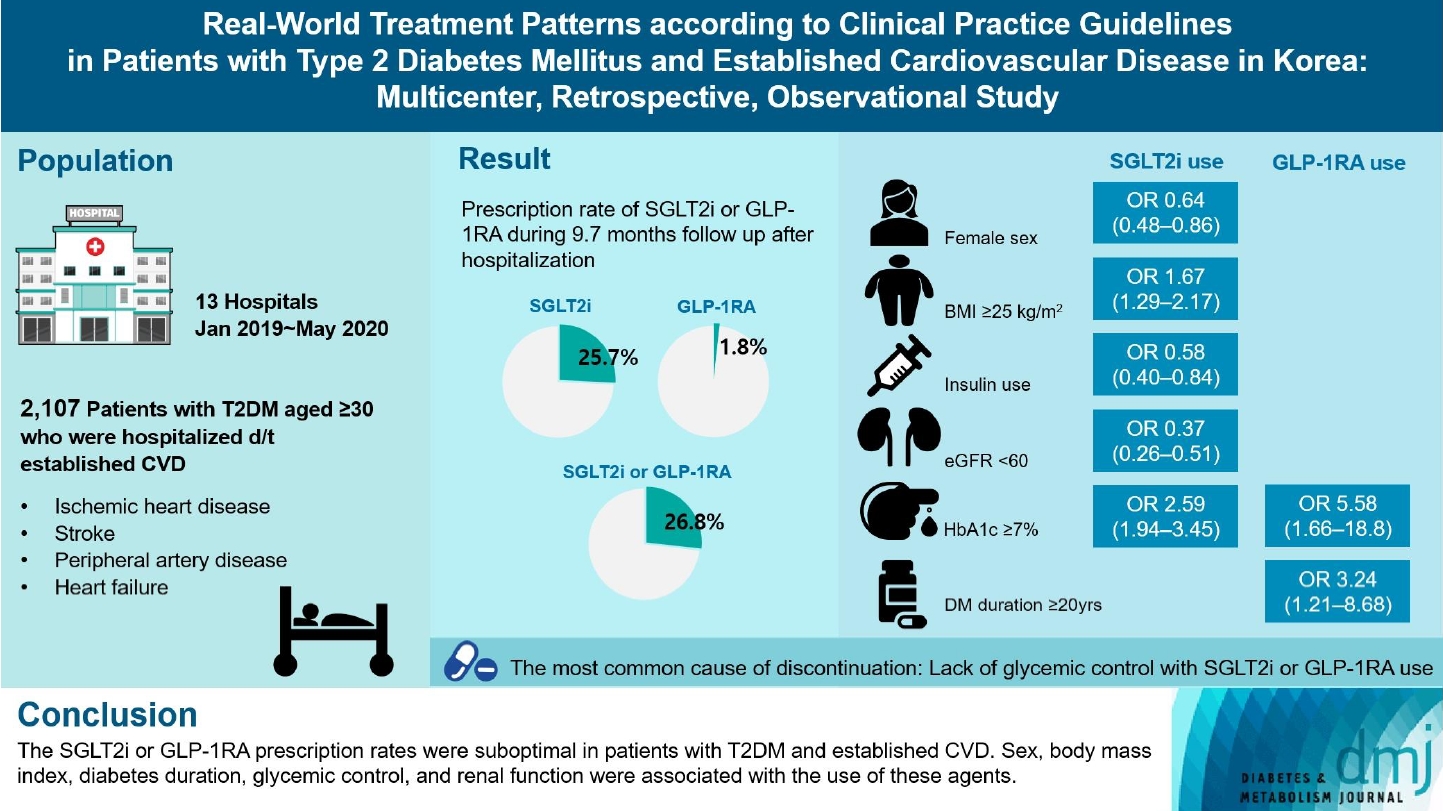
- Overall, 2,050 patients were eligible for analysis among 2,107 enrolled patients. The mean patient age, diabetes duration, and glycosylated hemoglobin level were 70.0 years, 12.0 years, and 7.5%, respectively. During the mean follow-up duration of 9.7 months, 25.7% of the patients were prescribed SGLT2is after CVD events. However, only 1.8% were prescribed GLP-1RAs. Compared with SGLT2i non-users, SGLT2i users were more frequently male and obese. Furthermore, they had a shorter diabetes duration but showed worse glycemic control and better renal function at the time of the event. GLP-1RA users had a longer duration of diabetes and worse glycemic control at the time of the event than GLP-1RA non-users.
-
Conclusion
- The SGLT2i or GLP-1RA prescription rates were suboptimal in patients with T2DM and established CVD. Sex, body mass index, diabetes duration, glycemic control, and renal function were associated with the use of these agents.
- • We aimed to evaluate SGLT2i or GLP-1RA use in patients with T2DM and established CVD.
- • 26.8% of the patients received SGLT2is or GLP-1RA after CVD events.
- • Sex, BMI, DM duration, glycemic control, and renal function influenced drug use.
- • The primary reason for discontinuing these drugs was inadequate glycemic control.
Highlights
- Among antidiabetic drugs, sodium-glucose cotransporter 2 inhibitors (SGLT2i) and glucagon-like peptide-1 receptor agonists (GLP-1RA) have been shown to reduce the risk of major adverse cardiovascular events and improve renal outcomes in several large randomized control trials [1-5]. Therefore, there has been a paradigm shift in the use of antidiabetic drugs, from the lowering of blood glucose levels to protection against cardiovascular disease (CVD) and chronic kidney disease (CKD). Recent recommendations for diabetes treatment by the American Diabetes Association [6] and the Korean Diabetes Association (KDA) [7] emphasize that SGLT2is and GLP-1RAs with proven cardiovascular benefits should be prioritized for combination therapy in patients with type 2 diabetes mellitus (T2DM) and established CVD or heart failure (HF).
- After the first large cardiovascular outcome trial of SGLT2i showed significant cardiovascular benefits in patients with T2DM [2], the prescription rates of SGLT2is and GLP-1RAs have continued to increase not only in Korea [8] but also worldwide [9-13]. It is therefore important to assess the real-world clinical treatment rates of SGLT2is and GLP-1RAs. If the actual treatment rates are not consistent, i.e., lower than the recommended guidelines, it is necessary to evaluate the barriers to the prescription of these agents or the causes of the lower-than-expected prescription rates for these agents. However, the prescription rates for these drugs in eligible patients with established CVD and HF according to guidelines have not been thoroughly evaluated in Korea. Therefore, we conducted this study to evaluate the prescription rates of SGLT2is or GLP-1RAs in patients with T2DM and established CVD according to the KDA guidelines.
INTRODUCTION
- Study design
- The current study was a multicenter retrospective study conducted at 13 secondary and tertiary hospitals in Korea. The study protocol was reviewed and approved by the local ethics committee of each hospital (Institutional Review Board no. for Uijeongbu St. Mary’s Hospital, CIRB-20200928-002), and conducted in accordance with the Declaration of Helsinki. The need for informed consent from the patients was waived because of the retrospective nature of this study.
- Patients and eligibility
- Patients with T2DM who were 30 years of age or older were eligible if they were hospitalized because of established CVD during the enrollment period (January 2019 to May 2020). The exclusion criteria were as follows: (1) patients with type 1 diabetes mellitus, (2) pregnant women, (3) those undergoing chemotherapy or radiotherapy for malignancy, and (4) those hospitalized for a simple diagnostic procedure for a CVD, such as coronary angiography. Established CVD was defined as atherosclerotic cardiovascular disease (ASCVD) and hospitalization for heart failure (HHF). ASCVD comprised three categories: (1) ischemic heart disease (IHD), defined as myocardial infarction and acute coronary syndrome requiring primary coronary intervention or coronary artery bypass grafting, and coronary artery disease with stenosis confirmed by coronary angiography from cardiologists; (2) stroke, which consisted of ischemic stroke or transient ischemic attack and was diagnosed based on magnetic resonance imaging or medical records from neurologists; and (3) peripheral artery disease (PAD) requiring angioplasty, bypass surgery, or amputation during hospitalization.
- Data collection
- The index date was defined as the day on which each patient was first admitted to the hospital owing to established CVD events. The enrolled patients were followed up until August 2020. The information analyzed included demographic characteristics, anthropometric data, medical history, laboratory test results, and antidiabetic medications prescribed. This information was collected from the patients’ electronic medical records at baseline and every 3 months after the index date by the investigators listed on the case report form. Baseline demographic and anthropometric data were collected at the time the patient was discharged or at the time closest to discharge after the index date. Prescription rates for cardiovascular risk-reducing drugs and antidiabetic drugs at discharge and during the follow-up period after the CVD event, were calculated for all cases who had been taking medication before the index date or started taking the medication after the index date. The primary outcomes were the prescription rates of SGLT2is or GLP-1RAs during the follow-up period, and the secondary outcomes were various factors related to the use and discontinuation of SGLT2is and GLP-1RAs. Causes of medication discontinuation were assessed by dividing them into two categories: patient factors (complaints of side effects, inappropriate glycemic control, or others) and treatment factors (evidence of side effects, inappropriate glycemic control, or progression of complications).
- Statistical analysis
- Continuous variables are presented as mean±standard deviation values, and categorical variables are presented as numbers and percentages. An independent-samples t-test was used to compare users and non-users of medication. The chi-square test and Fisher’s exact test were used to compare categorical variables. Logistic regression models were used to evaluate the odds ratios (ORs) with 95% confidence intervals (CIs) of clinical factors for the use or discontinuation of medications. Multivariate logistic regression models were used, including variables with a P value of <0.05, in the univariate analysis. All statistical analyses were performed using SPSS version 25.0 for Windows (IBM Co., Armonk, NY, USA), and a P value of <0.05 was considered significant.
METHODS
- Baseline patient demographics
- A total of 2,107 patients with T2DM who were hospitalized because of established CVD were enrolled from 13 centers; 57 patients died in the hospital during the admission period. Finally, 2,050 patients (66.9% of the patients were men) were eligible for analysis. The mean age of the study population, diabetes duration, and glycosylated hemoglobin (HbA1c) level were 70.0 years, 12.0 years, and 7.5%, respectively. Many patients (1,522 patients, 74.2%) had hypertension upon admission. Approximately 33.7%, 14.8%, 4.3%, and 11.4% of the patients previously had IHD, stroke, PAD, and HF, respectively. Other clinical variables are shown in Supplementary Table 1. Among the 2,050 patients, 58.3% (n=1,196), 20.9% (n=428), 4.1% (n=83), and 16.7% (n=343) were hospitalized due to IHD, stroke, PAD, and HF, respectively.
- Prescription patterns after established CVD events
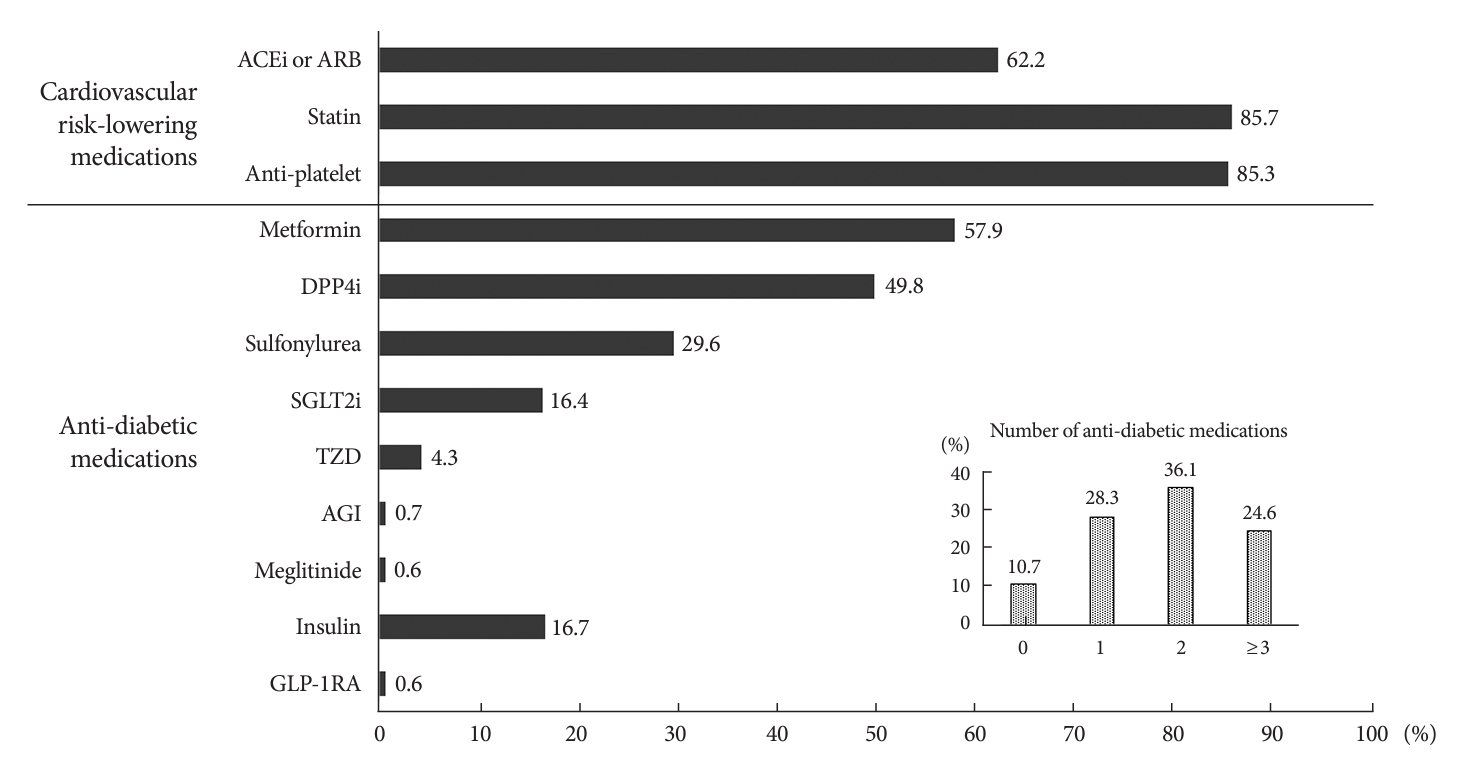
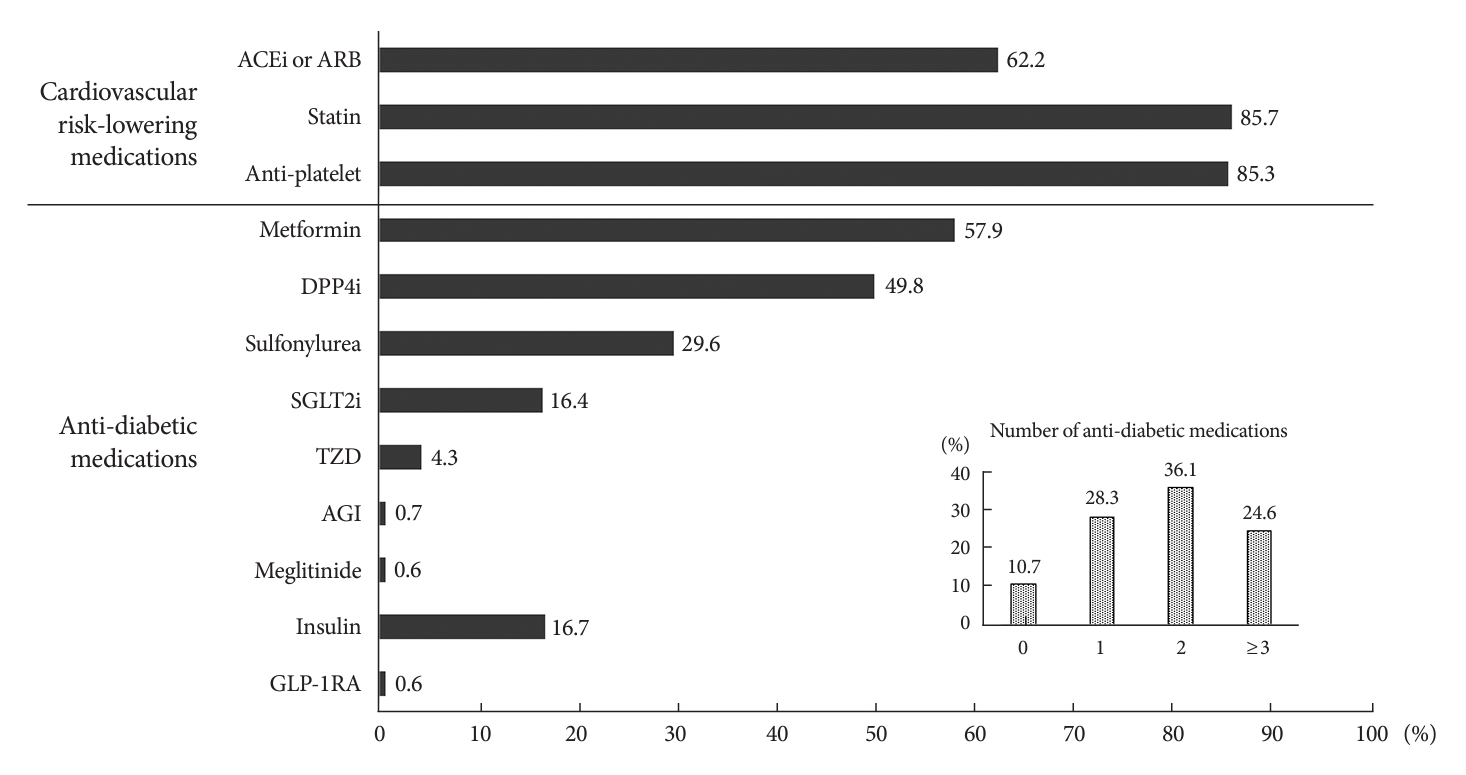
- The departments managing diabetes after CVD events were mostly endocrinology (43.8%, n=898) and cardiology (34.3%, n=704); 4.5% (n=92), 3.4% (n=70), and 11.7% (n=234) of the cases were handled by nephrology, neurology, and other departments. Fig. 1 shows the prescription rate of cardiovascular risk-lowering medications and antidiabetic agents at discharge after the CVD events. The prescription rates of statins and anti-platelet agents were approximately 85%. And 62.2% of patients received angiotensin-converting enzyme inhibitors or angiotensin receptor blockers as antihypertensive medications at discharge (Fig. 1). More than half of the patients used over two classes of antidiabetic agents; 36.1% used two classes of agents and 24.6% used ≥3 classes of agents. More than half of the patients (57.9%) used metformin, and the second most commonly used class of agents was dipeptidyl peptidase 4 inhibitors (DPP4is, 49.8%). The prescription rates of SGLT2is and GLP-1RAs at discharge were 16.4% and 0.6%, respectively (Fig. 1).
- During the mean follow-up duration of 9.7±0.1 months, 25.7% of the patients were prescribed SGLT2is after CVD events. However, only 1.8% of the patients were prescribed GLP-1RAs. Eventually, 26.8% of the patients were prescribed SGLT2is or GLP-1RAs among the patients with T2DM and established CVD. Of the patients taking SGLT2is and GLP-1RAs, 91.3% and 82.8% were newly started after CVD events occurred, respectively. The mean times to the initiation of SGLT2is and GLP-1RAs after discharge from the hospital were 58.9 and 91.6 days, respectively, among the patients for whom these agents were started after CVD events. And 58.7% and 27.6% of newly prescribed medication after CVD events were prescribed at discharge. The class and number of antidiabetic medications prescribed at the time of SGLT2is or GLP-1RAs initiation are shown in Supplementary Table 2.
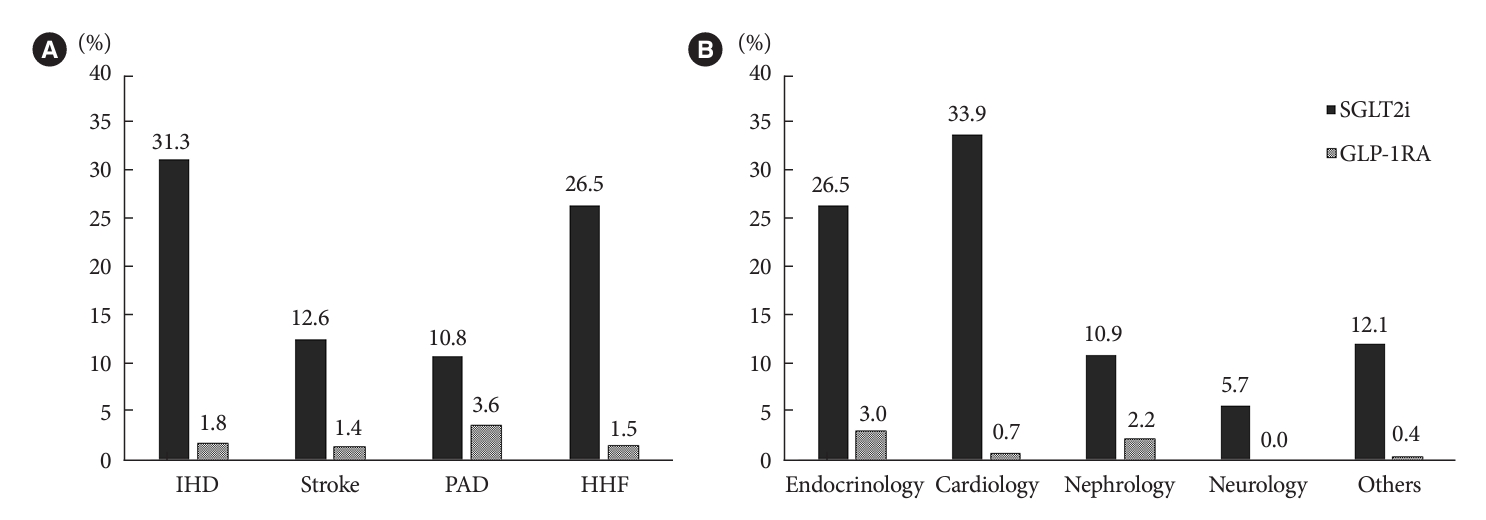
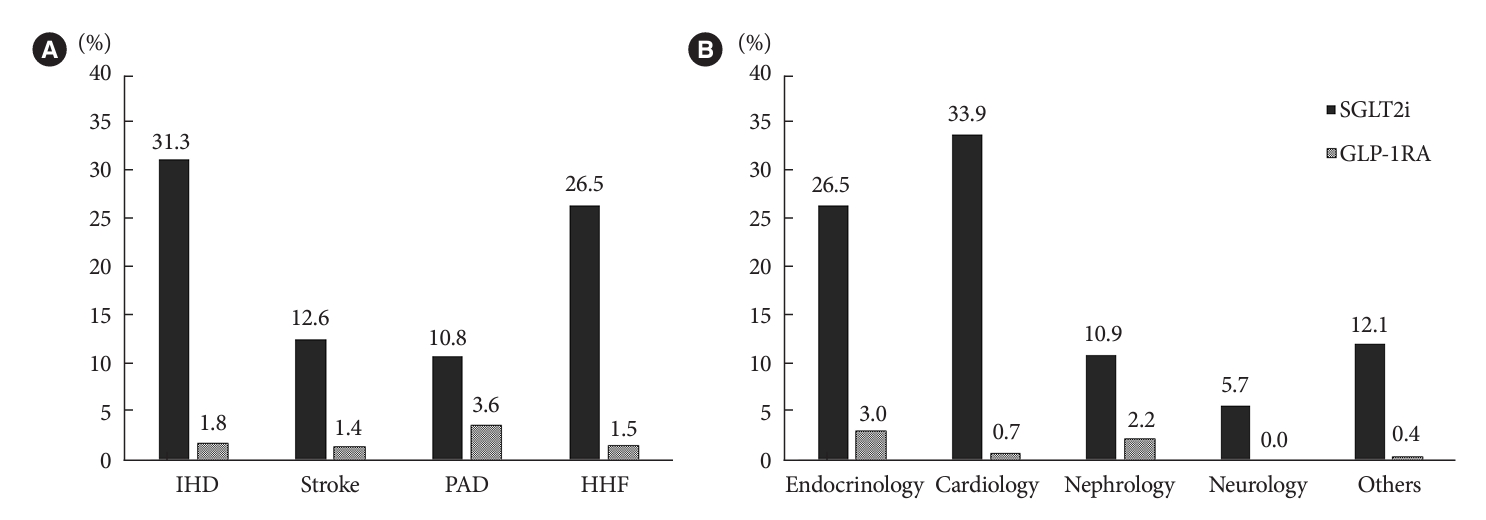
- The prescription rates of SGLT2is or GLP-1RAs differed according to the cause of the established CVD and the department managing diabetes after the CVD events (Fig. 2). SGLT2is were used in 31.3%, 26.5%, 12.6%, and 10.8% of the patients with IHD, HHF, stroke, and PAD, respectively. The corresponding percentages of patients in whom GLP-1RAs were used were 1.8%, 1.5%, 1.4%, and 3.6%. SGLT2is were more likely to be prescribed to patients who were attended to primarily by cardiologists (33.9%, 239/704) and endocrinologists (26.5%, 238/898). On the other hand, GLP-1RAs were predominantly prescribed by endocrinologists (3.0%, 27/898), followed by nephrologists (2.2%, 2/92). The distribution of the departments prescribing SGLT2is or GLP-1RAs showed differences according to the cause of the established CVD events (Supplementary Fig. 1A and B, respectively). In the case of IHD, SGLT2is were similarly prescribed by endocrinologists and cardiologists. On the other hand, in the case of HHF, SGLT2is were more frequently prescribed by cardiologists. GLP-1RAs were predominantly prescribed by endocrinologists for events of all causes.
- Comparison of patients’ characteristics at discharge according to the use of SGLT2is or GLP-1RAs
- Tables 1, 2 show the comparison of patients’ characteristics at discharge according to the use of SGLT2is or GLP-1RAs. Compared with SGLT2i non-users, SGLT2i users were more frequently male (75.8% vs. 64.0%, P<0.001) and obese (body mass index [BMI]: 25.5 kg/m2 vs. 24.7 kg/m2, P<0.001). Furthermore, the duration of diabetes was shorter among SGLT2i users (10.4 years vs. 12.6 years, P<0.001); however, they showed worse glycemic control (HbA1c: 7.9 % vs. 7.4%, P<0.001). SGLT2i users also had a higher estimated glomerular filtration rate (eGFR) at the time of the CVD event (82.5 mL/min/1.73 m2 vs. 69.1 mL/min/1.73 m2, P<0.001). Over half (62.1%) of the SGLT2i users were using the medication at the time of discharge after CVD events.
- Compared with that in GLP-1RA non-users, the duration of diabetes was longer among GLP-1RA users (16.3 years vs. 11.9 years, P=0.021) and glycemic control was worse (HbA1c: 8.9% vs. 7.5%, P<0.001) at the time of the CVD event. However, sex, BMI, and renal function were comparable between the two groups. GLP-1RA users took more antidiabetic medications than GLP-1RA non-users did. In particular, insulin use was significantly higher in GLP-1RA users than in GLP-1RA nonusers.
- Association between several baseline clinical factors and medication use
- We analyzed the associations between several clinical factors and the use of SGLT2is or GLP-1RAs (Table 3). Female sex, insulin use, and an eGFR of <60 mL/min/1.73 m2 were significantly associated with the non-use of SGLT2is. BMI of ≥25 kg/m2 and HbA1c level of ≥7% were significantly associated with SGLT2i use. Unlike SGLT2i use, GLP-1RA use was not associated with sex, BMI, and renal function. Univariate analysis showed that insulin use, diabetes duration of more than 20 years, and HbA1c level of ≥7% were significantly associated with GLP-1RA use. Multivariate analysis revealed that the duration of diabetes and HbA1c level were associated with GLP-1RA use.
- Discontinuation of medications
- Regarding the discontinuation of SGLT2is or GLP-1RAs, analysis of electronic medical records and laboratory test results showed that 17.0% (n=82/482) of SGLT2i users and 51.7% (n=15/29) of GLP-1RA users among those who started taking these medications after CVD events stopped taking these agents (Table 4). The mean times to SGLT2i and GLP-1RA discontinuation were 110.3 and 93.9 days, respectively, after starting the medications. The most common cause of SGLT2i discontinuation was a lack of glycemic control with SGLT2i use, followed by patient complaints of dehydration or body weight reduction after starting the medication. Objective evidence of urinary tract or genital infection was found in one case. The most common cause of GLP-1RA discontinuation was a lack of glycemic control with GLP-1RA use.
RESULTS
- In this retrospective, observational multicenter study, we assessed SGLT2i or GLP-1RA usage rates and various related factors in patients with T2DM and established CVD. We found that the prescription rates of SGLT2i or GLP-1RAs in our patient population were suboptimal (25.7% and 1.8%, respectively). Furthermore, compared with SGLT2i non-users, SGLT2i users were more frequently male and obese. SGLT2i users also had better renal function and a shorter duration of diabetes but had worse glycemic control. GLP-1RA users had a longer duration of diabetes and worse glycemic control than GLP-1RA non-users did. However, sex, BMI, and renal function were comparable between the two groups. Diabetes duration and glycemic control status were associated with the use of both agents, while sex, BMI, insulin use, and renal function were only associated with SGLT2i use. Insufficient glycemic control was the most common reason for the discontinuation of both classes of drugs.
- The prescription rates for SGLT2is or GLP-1RAs were lower than those recommended in the treatment guidelines in other countries also. In a study based on a large outpatient registry in the USA [14], only 5.2% and 6.0% of patients were prescribed SGLT2is and GLP-1RAs, respectively, among potentially eligible patients according to the enrollment criteria of previous cardiovascular outcome trials [2,3]. The low use of these agents was consistent with more recent real-world data in the USA [12]. In a Danish nationwide cohort study, 14.7% of patients with T2DM and CVD used SGLT2is and GLP-1RAs at 2 years after the diagnosis [15]. In an observational study in the USA, diabetes patients with CVD and nephropathy were 17% to 73% less likely to start GLP-1RAs and/or SGLT2is compared with DPP4is [16]. In our study, we found that SGLT2is were used at least for patients with IHD and HHF rather than others. However, the prescription rate for GLP-1RAs was especially low overall. In a study using nationwide population-based cohort data in Korea, the prescription rates of SGLT2is after the first hospitalization for ASCVD and HF in patients with T2DM were 13.7% and 11.2%, respectively, and there was no difference in the prescription rates of the drugs according to the presence of CVD and HF [17]. Considering that the national data showed a lower prescription rate of SGLT2is than in our study, the prescription rate of GLP-1RAs in the general population with T2DM with established CVD may be lower than the result in our study. The reason for this low prescription rate may be that the treatment guideline has not yet been widely implemented; the treatment guideline to prioritize the use of SGLT2i or GLP-1RA in diabetic patients with CVD was first published in Korea in 2019, and this study was conducted on patients hospitalized since 2019. Therefore, it is estimated that the use of these drugs will increase over time, and a follow-up study for more recent prescription patterns is needed.
- The prescription rates of medications differed depending on the diabetes management department or the cause of the CVD event. In the case of GLP-1RAs, these drugs were mainly used by endocrinologists, and the fact that they were administered by injection seems to have been a hurdle to their use. In fact, GLP-1RAs tended to be used more in patients taking insulin who would have had long-lasting and uncontrolled diabetes, possibly because the burden of injections is less in patients taking insulin. Considering this point [18], if oral GLP-1RAs are introduced in the future, it is expected that more patients will be prescribed GLP-1RAs, especially earlier, which will greatly change the prescription pattern of GLP-1RAs among antidiabetic medications. Since patients with CVD and CKD are often followed up in other departments such as cardiology and nephrology, the efficacy of GLP-1RAs should be better known to physicians dealing with diabetes, and it should become an option that can be used in primary care settings.
- The finding that SGLT2i use was more common in men and obese patients was probably due to side effects such as genital infections in women [19,20] and its weight-reducing effect [21]. This also reflects the fact that physicians are concerned about the use of SGLT2is in elderly non-obese women in clinical practice. Although older age was not significantly associated with the medication use in our study, the previously mentioned study found that elderly and female patients were less likely to start SGLT2i treatment [17]. And another study revealed that use of SGLT2is and GLP-1RAs as first-line medications compared with that of metformin was associated with younger age and prevalent CVD [12].
- Unlike in the case of GLP-1RA users, patients with an eGFR of <60 mL/min/1.73 m2 were less likely to start SGLT2is (adjusted OR, 0.37; 95% CI, 0.26 to 0.51). This might be related to clinicians’ concerns regarding the decrease in eGFR in the early phase after starting SGLT2is in patients with CKD. The limitation of the use of SGLT2is in patients with CKD might be another reason because drug labeling for SGLT2is was extended to those with an eGFR of ≥45 mL/min/1.73 m2 in August 2019 after the CREDENCE trial results were published in June 2019 [22]. The clinical barriers based on renal function encountered in our study were also reported in a study of diabetes patients with CKD, defined as an eGFR of <60 mL/min/1.73 m2 or urine albumin-to-creatinine ratio of ≥30 mg/g, after September 2019. Only 25.6% of the patients received SGLT2is [23]. In other words, although it is well known that SGLT2is are effective against CKD, renal function has served as a barrier to drug initiation until recently. However, in July 2020, the KDA and the Korean Society of Nephrology released a consensus statement on the use of SGLT2is in patients with T2DM for attenuating renal function decline [19]. And recent studies have shown a protective effect in a population with more advanced CKD [5,24]. Therefore, it is expected that this association with eGFR will be negligible; rather, it will be used more in patients with low eGFR when changes in SGLT2i use are tracked in the future.
- It is interesting to note that the most common reason for discontinuing medication was poor glycemic control. Of course, in the case of GLP-1RA, the glucose-lowering effect of the agent might be insignificant in patients with a long duration of diabetes. However, given that GLP-1RAs were primarily used in patients with longer diabetes duration and poor glycemic control in the first place, this result for the reason for discontinuation suggests that clinicians are still focused on the glucose-lowering effect rather than on the preventive effect on complications such as CVD. At this point, it is imperative that physicians shift their perception of diabetes management from a glucocentric approach to a patient-centered holistic approach. This should be addressed through continuous education for physicians based on evidence-based treatment guidelines. In addition, there were fewer cases of drug discontinuation than expected due to side effects such as acute kidney injury or urinary tract/genital infection. This could be attributed to several factors. The incidence of side effects was low in Asians [25], and patients were well educated about side effects or the side effects were not serious enough to stop the medication. This result may also be a difference between clinical trials and real-world data.
- The timing of the initiation of these drugs is also interesting. Many trials allowed patients to be enrolled the study at least 2 weeks [3] or 2 months [1,2,4] after an established CVD events, such as myocardial infarction or unstable angina. However, our real-world data showed that 58.7% of patients who were newly prescribed the SGLT2i after events received the prescription at the time of discharge. There are no specific guidelines on when to initiate these drugs after the events. However, considering that there may be an initial decrease in GFR after the initiation of the SGLT2i and that ketoacidosis may occur in an ischemic state, the patient’s overall health, the severity of the event, and individual treatment goals are necessary to be considered when the drug should be initiated.
- Our study had several limitations. First, this study was conducted at 13 centers; therefore, it cannot represent the entire population with established CVD in Korea. However, patients with established CVD, who are definite targets for treatment with SGLT2is or GLP-1RAs, mostly require hospitalization in a secondary or tertiary hospital. We reviewed all participants’ data during the study period in several secondary and tertiary hospitals in various regions to overcome this limitation. Second, the follow-up period was short, less than 1 year. Longer follow-up may have showed increased SGLT2is or GLP-1RAs usage rates. Lastly, since the reasons for discontinuation of medication were evaluated retrospectively through medical records, the reasons for medication discontinuation may be underestimated or the proportion may not be accurate if the records are incomplete. However, the reason for medication discontinuation in real-world data can only be identified through a medical record review. Therefore, medical records of other departments and outpatient clinics were comprehensively reviewed to increase accuracy. Furthermore, objective data such as HbA1c level and urinary test results were also reviewed.
- In conclusion, the prescription rates of SGLT2is or GLP-1RAs were suboptimal in patients with T2DM and established CVD. Sex, BMI, duration of diabetes, glycemic control, and renal function were associated with the use of these agents. Our study results suggest that more effort is needed for education based on evidence-based treatment. Because of these efforts and accumulated evidence, we expect an increase in the prescriptions of SGLT2is or GLP-1RAs with the adoption of patient-centered approaches.
DISCUSSION
SUPPLEMENTARY MATERIALS
Supplementary Table 1.
Supplementary Table 2.
Supplementary Fig. 1.
-
CONFLICTS OF INTEREST
Seung-Hyun Ko has been executive editor of the Diabetes & Metabolism Journal since 2022. She was not involved in the review process of this article. Otherwise, there was no conflict of interest.
-
AUTHOR CONTRIBUTIONS
Conception or design: Y.S.Y., J.H.B., S.H.K., K.Y.H.
Acquisition, analysis, or interpretation of data: All authors.
Drafting the work or revising: Y.S.Y., K.Y.H.
Final approval of the manuscript: All authors.
-
FUNDING
None
NOTES
-
Acknowledgements
- This work was supported by the Korea Health Industry Development Institute-AstraZeneca (KHIDI-AZ) Diabetes Research Program and the Korean Diabetes Association (KDA). Statistical consultation was supported by the Department of Biostatistics of the Catholic Research Coordinating Center.
Values are presented as number (%) or mean±standard deviation.
SGLT2i, sodium-glucose cotransporter 2 inhibitor; BMI, body mass index; IHD, ischemic heart disease; PAD, peripheral artery disease; HF, heart failure; HHF, hospitalization for heart failure; SBP, systolic blood pressure; DBP, diastolic blood pressure; HbA1c, glycosylated hemoglobin; eGFR, estimated glomerular filtration rate; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; TZD, thiazolidinedione; DPP4i, dipeptidyl peptidase 4 inhibitor; AGI, alpha-glucosidase inhibitor; GLP-1RA, glucagon-like peptide 1 receptor agonist; ACEi, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blockade.
Values are presented as number (%) or mean±standard deviation.
GLP-1RA, glucagon-like peptide 1 receptor agonist; BMI, body mass index; IHD, ischemic heart disease; PAD, peripheral artery disease; HF, heart failure; HHF, hospitalization for heart failure; SBP, systolic blood pressure; DBP, diastolic blood pressure; HbA1c, glycosylated hemoglobin; eGFR, estimated glomerular filtration rate; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; TZD, thiazolidinedione; DPP4i, dipeptidyl peptidase 4 inhibitor; SGLT2i, sodium-glucose cotransporter 2 inhibitor; AGI, alpha-glucosidase inhibitor; ACEi, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blockade.
| Variable | No. (%) |
|---|---|
| SGLT2i | |
| Discontinuation of SGLT2ia | 82/482 (17.0) |
| Patient factor; complaint of | 10/82 (12.2) |
| Dehydration or weight reduction | 5 (6.1) |
| Genital problem | 1 (1.2) |
| Polyuria | 1 (1.2) |
| Glucose control (hyper/hypo-glycemia) | 1 (1.2) |
| Others | 2 (2.4) |
| Treatment factor; evidence for | 22/82 (26.8) |
| Uncontrolled glucose level | 16 (19.5) |
| Acute kidney injury | 2 (2.4) |
| Urinary tract/genital infection | 1 (1.2) |
| Complication of diabetes | 1 (1.2) |
| Diabetic ketoacidosis | 0 |
| GLP-1RA | |
| Discontinuation of GLP-1RAb | 15/29 (51.7) |
| Patient factor; complaint of | 3/15 (20.0) |
| Gastrointestinal problem | 1 (6.7) |
| Injection site problem | 1 (6.7) |
| Glucose control (hyper/hypo-glycemia) | 0 |
| Others | 1 (6.7) |
| Treatment factor; evidence for | 4/15 (26.7) |
| Uncontrolled glucose level | 3 (20.0) |
| Complication of diabetes | 1 (6.7) |
| Gastropathy | 0 |
- 1. Wiviott SD, Raz I, Bonaca MP, Mosenzon O, Kato ET, Cahn A, et al. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med 2019;380:347-57.ArticlePubMed
- 2. Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, Hantel S, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med 2015;373:2117-28.ArticlePubMed
- 3. Marso SP, Daniels GH, Brown-Frandsen K, Kristensen P, Mann JF, Nauck MA, et al. Liraglutide and cardiovascular outcomes in type 2 diabetes. N Engl J Med 2016;375:311-22.ArticlePubMedPMC
- 4. Gerstein HC, Colhoun HM, Dagenais GR, Diaz R, Lakshmanan M, Pais P, et al. Dulaglutide and cardiovascular outcomes in type 2 diabetes (REWIND): a double-blind, randomised placebo-controlled trial. Lancet 2019;394:121-30.PubMed
- 5. Heerspink HJ, Stefansson BV, Correa-Rotter R, Chertow GM, Greene T, Hou FF, et al. Dapagliflozin in patients with chronic kidney disease. N Engl J Med 2020;383:1436-46.ArticlePubMed
- 6. American Diabetes Association Professional Practice Committee. 9. Pharmacologic approaches to glycemic treatment: standards of medical care in diabetes-2022. Diabetes Care 2022;45(Suppl 1):S125-43.ArticlePubMedPDF
- 7. Hur KY, Moon MK, Park JS, Kim SK, Lee SH, Yun JS, et al. 2021 Clinical practice guidelines for diabetes mellitus of the Korean Diabetes Association. Diabetes Metab J 2021;45:461-81.PubMedPMC
- 8. Bae JH, Han KD, Ko SH, Yang YS, Choi JH, Choi KM, et al. Diabetes fact sheet in Korea 2021. Diabetes Metab J 2022;46:417-26.ArticlePubMedPMCPDF
- 9. Wilkinson S, Douglas I, Stirnadel-Farrant H, Fogarty D, Pokrajac A, Smeeth L, et al. Changing use of antidiabetic drugs in the UK: trends in prescribing 2000-2017. BMJ Open 2018;8:e022768.ArticlePubMedPMC
- 10. Engler C, Leo M, Pfeifer B, Juchum M, Chen-Koenig D, Poelzl K, et al. Long-term trends in the prescription of antidiabetic drugs: real-world evidence from the Diabetes Registry Tyrol 2012-2018. BMJ Open Diabetes Res Care 2020;8:e001279.ArticlePubMedPMC
- 11. Yang A, Wu H, Lau ES, Zhang X, Shi M, Fan B, et al. Glucose-lowering drug use, glycemic outcomes, and severe hypoglycemia: 18-year trends in 0.9 million adults with Diabetes in Hong Kong (2002-2019). Lancet Reg Health West Pac 2022;26:100509.ArticlePubMedPMC
- 12. Shin H, Schneeweiss S, Glynn RJ, Patorno E. Trends in first-line glucose-lowering drug use in adults with type 2 diabetes in light of emerging evidence for SGLT-2i and GLP-1RA. Diabetes Care 2021;44:1774-82.ArticlePubMedPMCPDF
- 13. Pottegard A, Andersen JH, Sondergaard J, Thomsen RW, Vilsboll T. Changes in the use of glucose-lowering drugs: a Danish nationwide study. Diabetes Obes Metab 2023;25:1002-10.ArticlePubMedPDF
- 14. Arnold SV, Inzucchi SE, Tang F, McGuire DK, Mehta SN, Maddox TM, et al. Real-world use and modeled impact of glucose-lowering therapies evaluated in recent cardiovascular outcomes trials: an NCDR® Research to Practice project. Eur J Prev Cardiol 2017;24:1637-45.ArticlePubMedPDF
- 15. Funck KL, Knudsen JS, Hansen TK, Thomsen RW, Grove EL. Real-world use of cardioprotective glucose-lowering drugs in patients with type 2 diabetes and cardiovascular disease: a Danish nationwide cohort study, 2012 to 2019. Diabetes Obes Metab 2021;23:520-9.ArticlePubMedPMCPDF
- 16. McCoy RG, Van Houten HK, Karaca-Mandic P, Ross JS, Montori VM, Shah ND. Second-line therapy for type 2 diabetes management: the treatment/benefit paradox of cardiovascular and kidney comorbidities. Diabetes Care 2021;44:2302-11.ArticlePubMedPMCPDF
- 17. Baek JH, Yang YS, Ko SH, Han KD, Kim JH, Moon MK, et al. Real-world prescription patterns and barriers related to the use of sodium-glucose cotransporter 2 inhibitors among Korean patients with type 2 diabetes mellitus and cardiovascular disease. Diabetes Metab J 2022;46:701-12.ArticlePubMedPMCPDF
- 18. Igarashi A, Bekker Hansen B, Langer J, Tavella F, Collings H, Davies N, et al. Preference for oral and injectable GLP-1 RA therapy profiles in Japanese patients with type 2 diabetes: a discrete choice experiment. Adv Ther 2021;38:721-38.ArticlePubMedPMCPDF
- 19. Oh TJ, Moon JY, Hur KY, Ko SH, Kim HJ, Kim T, et al. Sodium-glucose cotransporter-2 inhibitor for renal function preservation in patients with type 2 diabetes mellitus: a Korean Diabetes Association and Korean Society of Nephrology consensus statement. Diabetes Metab J 2020;44:489-97.ArticlePubMedPMCPDF
- 20. McGovern AP, Hogg M, Shields BM, Sattar NA, Holman RR, Pearson ER, et al. Risk factors for genital infections in people initiating SGLT2 inhibitors and their impact on discontinuation. BMJ Open Diabetes Res Care 2020;8:e001238.ArticlePubMedPMC
- 21. Cheong AJ, Teo YN, Teo YH, Syn NL, Ong HT, Ting AZ, et al. SGLT inhibitors on weight and body mass: a meta-analysis of 116 randomized-controlled trials. Obesity (Silver Spring) 2022;30:117-28.ArticlePubMedPDF
- 22. Perkovic V, Jardine MJ, Neal B, Bompoint S, Heerspink HJ, Charytan DM, et al. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. N Engl J Med 2019;380:2295-306.ArticlePubMed
- 23. Jeong SJ, Lee SE, Shin DH, Park IB, Lee HS, Kim KA. Barriers to initiating SGLT2 inhibitors in diabetic kidney disease: a real-world study. BMC Nephrol 2021;22:177.ArticlePubMedPMCPDF
- 24. The EMPA-KIDNEY Collaborative Group, Herrington WG, Staplin N, Wanner C, Green JB, Hauske SJ, et al. Empagliflozin in patients with chronic kidney disease. N Engl J Med 2023;388:117-27.ArticlePubMedPMC
- 25. Cai X, Gao X, Yang W, Chen Y, Zhang S, Zhou L, et al. No disparity of the efficacy and all-cause mortality between Asian and non-Asian type 2 diabetes patients with sodium-glucose cotransporter 2 inhibitors treatment: a meta-analysis. J Diabetes Investig 2018;9:850-61.ArticlePubMedPMCPDF
REFERENCES
Figure & Data
References
Citations
- Enhancing Patient Outcomes: Prioritizing SGLT2is and GLP-1RAs in Diabetes with CVD
Gwanpyo Koh
Diabetes & Metabolism Journal.2024; 48(2): 208. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite