
- Current
- Browse
- Collections
-
For contributors
- For Authors
- Instructions to authors
- Article processing charge
- e-submission
- For Reviewers
- Instructions for reviewers
- How to become a reviewer
- Best reviewers
- For Readers
- Readership
- Subscription
- Permission guidelines
- About
- Editorial policy
Articles
- Page Path
- HOME > Diabetes Metab J > Volume 35(3); 2011 > Article
-
Original ArticleTherapeutic Target Achievement in Type 2 Diabetic Patients after Hyperglycemia, Hypertension, Dyslipidemia Management
- Ah Young Kang1, Su Kyung Park2, So Young Park2, Hye Jeong Lee3, Ying Han4, Sa Ra Lee5, Sung Hwan Suh6, Duk Kyu Kim2,4, Mi Kyoung Park2,4
-
Diabetes & Metabolism Journal 2011;35(3):264-272.
DOI: https://doi.org/10.4093/dmj.2011.35.3.264
Published online: June 30, 2011
- 10,055 Views
- 35 Download
- 12 Crossref
1Department of Internal Medicine, Choon Hae Hospital, Busan, Korea.
2Division of Endocrinology and Metabolism, Department of Internal Medicine, Dong-A University Medical Center, Busan, Korea.
3Department of Pharmacology, Dong-A University College of Medicine, Busan, Korea.
4Diabetes Center, Dong-A University Medical Sciences Research Institute, Busan, Korea.
5Department of Internal Medicine, Sevrance UVA Surgery, Busan, Korea.
6Division of Endocrinology and Metabolism, Department of Internal Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- Corresponding author: Mi Kyoung Park. Division of Endocrinology and Metabolism, Department of Internal Medicine, Dong-A University Medical Center, Dong-A University College of Medicine, 3-1 Dongdaesin-dong, Seo-gu, Busan 602-715, Korea. pmk02@dau.ac.kr
Copyright © 2011 Korean Diabetes Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.

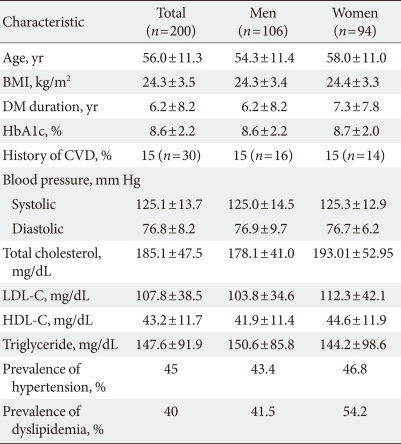

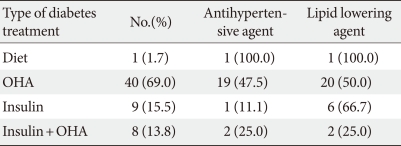
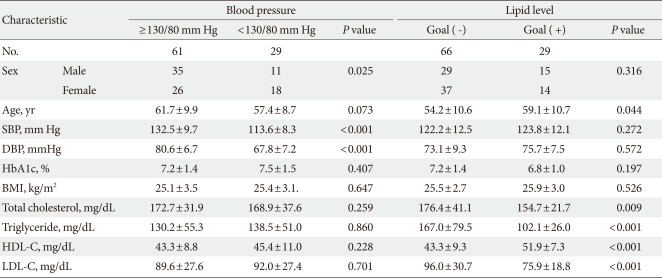
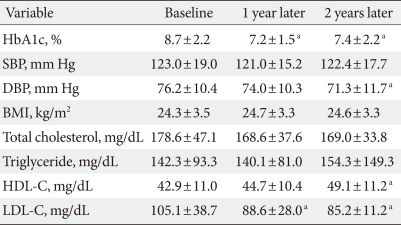
Figure & Data
References
Citations
- Achievement of the ABC goal among Canadians with type 2 diabetes and the influence of physical activity: data from the Canadian Health Measures Survey
Alexis Marcotte-Chénard, René Maréchal, Ahmed Ghachem, Alan Cohen, Eléonor Riesco
Applied Physiology, Nutrition, and Metabolism.2023; 48(9): 657. CrossRef - Poor Adherence to Common Recommendations and Associated Factors among Outpatients with Type 2 Diabetes Mellitus in a Police Hospital of Ethiopia
Tariku Shimels, Melesse Abebaw, Gebremedhin Beedemariam Gebretekle
Journal of Social Health and Diabetes.2021; 9(01): e8. CrossRef - Prevalence and correlation of glycemic control achievement in patients with type 2 diabetes in Iraq: A retrospective analysis of a tertiary care database over a 9-year period
Abbas Ali Mansour, Nassar T.Y. Alibrahim, Haider A. Alidrisi, Ali H. Alhamza, Ammar M. Almomin, Ibrahim Abbood Zaboon, Muayad Baheer Kadhim, Rudha Naser Hussein, Hussein Ali Nwayyir, Adel Gassab Mohammed, Dheyaa K.J. Al-Waeli, Ibrahim Hani Hussein
Diabetes & Metabolic Syndrome: Clinical Research & Reviews.2020; 14(3): 265. CrossRef - Notoginsenoside R1 Ameliorates Diabetic Retinopathy through PINK1-Dependent Activation of Mitophagy
Ping Zhou, Weijie Xie, Xiangbao Meng, Yadong Zhai, Xi Dong, Xuelian Zhang, Guibo Sun, Xiaobo Sun
Cells.2019; 8(3): 213. CrossRef - Association of Self-Reported Dietary and Drug Compliance with Optimal Metabolic Control in Patients with Type 2 Diabetes: Clinic-Based Single-Center Study in a Developing Country
Thilak Priyantha Weerarathna, Miyuru Kavinda Weerarathna, Vidarsha Senadheera, Herath Mudiyanselage Meththananda Herath, Gayani Liyanage
Journal of Nutrition and Metabolism.2018; 2018: 1. CrossRef - Prevalence of primary aldosteronism among patients with type 2 diabetes
Mauro Tancredi, Gudmundur Johannsson, Björn Eliasson, Robert Eggertsen, Ulf Lindblad, Sofia Dahlqvist, Henrik Imberg, Marcus Lind
Clinical Endocrinology.2017; 87(3): 233. CrossRef - GS-E3D, a new pectin lyase-modified red ginseng extract, inhibited diabetes-related renal dysfunction in streptozotocin-induced diabetic rats
Chan-Sik Kim, Kyuhyung Jo, Jin Sook Kim, Mi-Kyung Pyo, Junghyun Kim
BMC Complementary and Alternative Medicine.2017;[Epub] CrossRef - Ursodeoxycholic acid and 4-phenylbutyrate prevent endoplasmic reticulum stress-induced podocyte apoptosis in diabetic nephropathy
Ai-Li Cao, Li Wang, Xia Chen, Yun-Man Wang, Heng-Jiang Guo, Shuang Chu, Cheng Liu, Xue-Mei Zhang, Wen Peng
Laboratory Investigation.2016; 96(6): 610. CrossRef - Ursodeoxycholic Acid Ameliorated Diabetic Nephropathy by Attenuating Hyperglycemia-Mediated Oxidative Stress
Aili Cao, Li Wang, Xia Chen, Hengjiang Guo, Shuang Chu, Xuemei Zhang, Wen Peng
Biological & Pharmaceutical Bulletin.2016; 39(8): 1300. CrossRef - Withania coagulansFruit Extract Reduces Oxidative Stress and Inflammation in Kidneys of Streptozotocin-Induced Diabetic Rats
Shreesh Ojha, Juma Alkaabi, Naheed Amir, Azimullah Sheikh, Ahmad Agil, Mohamed Abdelmonem Fahim, Abdu Adem
Oxidative Medicine and Cellular Longevity.2014; 2014: 1. CrossRef - Assessment of cardiometabolic risk and prevalence of meeting treatment guidelines among patients with type 2 diabetes stratified according to their use of insulin and/or other diabetic medications: results from INSPIRE ME IAA
J. Smith, J.‐A. Nazare, A.‐L. Borel, P. Aschner, P. J. Barter, L. Van Gaal, Y. Matsuzawa, T. Kadowaki, R. Ross, C. Brulle‐Wohlhueter, N. Alméras, S. M. Haffner, B. Balkau, J.‐P. Després
Diabetes, Obesity and Metabolism.2013; 15(7): 629. CrossRef - Are PPAR alpha agonists a rational therapeutic strategy for preventing abnormalities of the diabetic kidney?
Pitchai Balakumar, Supriya Kadian, Nanjaian Mahadevan
Pharmacological Research.2012; 65(4): 430. CrossRef
 PubReader
PubReader Cite
Cite



