- Current
- Browse
- Collections
-
For contributors
- For Authors
- Instructions to authors
- Article processing charge
- e-submission
- For Reviewers
- Instructions for reviewers
- How to become a reviewer
- Best reviewers
- For Readers
- Readership
- Subscription
- Permission guidelines
- About
- Editorial policy
Articles
- Page Path
- HOME > Diabetes Metab J > Volume 47(5); 2023 > Article
-
ReviewGuideline/Fact Sheet 2023 Clinical Practice Guidelines for Diabetes Mellitus of the Korean Diabetes Association
-
Jong Han Choi1
 , Kyung Ae Lee2, Joon Ho Moon3, Suk Chon4, Dae Jung Kim5, Hyun Jin Kim6, Nan Hee Kim7, Ji A Seo7, Mee Kyoung Kim8, Jeong Hyun Lim9, YoonJu Song10, Ye Seul Yang11, Jae Hyeon Kim12, You-Bin Lee12, Junghyun Noh13, Kyu Yeon Hur12, Jong Suk Park14, Sang Youl Rhee4, Hae Jin Kim5, Hyun Min Kim15, Jung Hae Ko16, Nam Hoon Kim17, Chong Hwa Kim18, Jeeyun Ahn19, Tae Jung Oh3, Soo-Kyung Kim20, Jaehyun Kim21, Eugene Han22, Sang-Man Jin12, Won Suk Choi23, Min Kyong Moon24, Committee of Clinical Practice Guidelines, Korean Diabetes Association
, Kyung Ae Lee2, Joon Ho Moon3, Suk Chon4, Dae Jung Kim5, Hyun Jin Kim6, Nan Hee Kim7, Ji A Seo7, Mee Kyoung Kim8, Jeong Hyun Lim9, YoonJu Song10, Ye Seul Yang11, Jae Hyeon Kim12, You-Bin Lee12, Junghyun Noh13, Kyu Yeon Hur12, Jong Suk Park14, Sang Youl Rhee4, Hae Jin Kim5, Hyun Min Kim15, Jung Hae Ko16, Nam Hoon Kim17, Chong Hwa Kim18, Jeeyun Ahn19, Tae Jung Oh3, Soo-Kyung Kim20, Jaehyun Kim21, Eugene Han22, Sang-Man Jin12, Won Suk Choi23, Min Kyong Moon24, Committee of Clinical Practice Guidelines, Korean Diabetes Association -
Diabetes & Metabolism Journal 2023;47(5):575-594.
DOI: https://doi.org/10.4093/dmj.2023.0282
Published online: September 26, 2023
1Division of Endocrinology and Metabolism, Department of Internal Medicine, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul, Korea
2Division of Endocrinology and Metabolism, Department of Internal Medicine, Jeonbuk National University Hospital, Jeonbuk National University Medical School, Jeonju, Korea
3Department of Internal Medicine, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea
4Department of Endocrinology and Metabolism, College of Medicine, Kyung Hee University, Seoul, Korea
5Department of Endocrinology and Metabolism, Ajou University Hospital, Ajou University School of Medicine, Suwon, Korea
6Department of Internal Medicine, Chungnam National University Hospital, Chungnam National University College of Medicine, Daejeon, Korea
7Division of Endocrinology and Metabolism, Department of Internal Medicine, Korea University Ansan Hospital, Korea University College of Medicine, Ansan, Korea
8Division of Endocrinology and Metabolism, Department of Internal Medicine, Yeouido St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
9Department of Food Service and Nutrition Care, Seoul National University Hospital, Seoul, Korea
10Department of Food Science and Nutrition, The Catholic University of Korea, Bucheon, Korea
11Department of Internal Medicine, Seoul National University College of Medicine, Seoul, Korea
12Division of Endocrinology and Metabolism, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
13Division of Endocrinology and Metabolism, Department of Internal Medicine, Inje University Ilsan Paik Hospital, Inje University College of Medicine, Goyang, Korea
14Division of Endocrinology and Metabolism, Department of Internal Medicine, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea
15Division of Endocrinology and Metabolism, Department of Internal Medicine, Chung-Ang University College of Medicine, Seoul, Korea
16Division of Endocrinology and Metabolism, Department of Internal Medicine, Inje University Haeundae Paik Hospital, Inje University College of Medicine, Busan, Korea
17Division of Endocrinology and Metabolism, Department of Internal Medicine, Korea University Anam Hospital, Korea University College of Medicine, Seoul, Korea
18Division of Endocrinology and Metabolism, Department of Internal Medicine, Sejong General Hospital, Bucheon, Korea
19Department of Ophthalmology, Seoul Metropolitan Government Seoul National University Boramae Medical Center, Seoul National University College of Medicine, Seoul, Korea
20Division of Endocrinology and Metabolism, Department of Internal Medicine, CHA Bundang Medical Center, CHA University School of Medicine, Seongnam, Korea
21Department of Pediatrics, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea
22Department of Internal Medicine, Keimyung University School of Medicine, Daegu, Korea
23Division of Infectious Diseases, Department of Internal Medicine, Korea University Ansan Hospital, Korea University College of Medicine, Ansan, Korea
24Department of Internal Medicine, Seoul Metropolitan Government Seoul National University Boramae Medical Center, Seoul National University College of Medicine, Seoul, Korea
-
Corresponding author: Min Kyong Moon Department of Internal Medicine, Seoul Metropolitan Government Seoul National University Boramae Medical Center, Seoul National University College of Medicine, 20 Boramae-ro 5-gil, Dongjak-gu, Seoul 07061, Korea E-mail: mkmoon@snu.ac.kr
Copyright © 2023 Korean Diabetes Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- ABSTRACT
- INTRODUCTION AND SUMMARY OF REVISIONS
- SCREENING FOR DIABETES MELLITUS
- GLUCOSE MONITORING AND GLYCEMIC TARGET
- PHARMACOLOGICAL TREATMENT FOR ADULTS WITH T2DM
- HYPERTENSION MANAGEMENT IN PATIENTS WITH DIABETES
- LIPID MANAGEMENT IN PATIENTS WITH DIABETES
- DIABETIC KIDNEY DISEASE
- NON-ALCOHOLIC FATTY LIVER DISEASE IN PATIENTS WITH T2DM
- CONCLUSIONS
- NOTES
- REFERENCES
ABSTRACT
- In May 2023, the Committee of Clinical Practice Guidelines of the Korean Diabetes Association published the revised clinical practice guidelines for Korean adults with diabetes and prediabetes. We incorporated the latest clinical research findings through a comprehensive systematic literature review and applied them in a manner suitable for the Korean population. These guidelines are designed for all healthcare providers nationwide, including physicians, diabetes experts, and certified diabetes educators who manage patients with diabetes or individuals at risk of developing diabetes. Based on recent changes in international guidelines and the results of a Korean epidemiological study, the recommended age for diabetes screening has been lowered. In collaboration with the relevant Korean medical societies, recently revised guidelines for managing hypertension and dyslipidemia in patients with diabetes have been incorporated into this guideline. An abridgment containing practical information on patient education and systematic management in the clinic was published separately.
- Diabetes is a common disease; however, as a chronic and progressive condition accompanied by various complications, it significantly increases individual and socioeconomic burdens. According to the “Diabetes fact sheet in Korea 2021” by the Korean Diabetes Association (KDA), 16.7% of adults over 30 years of age, which is about 5.7 million people, will have diabetes in 2020 [1]. Moreover, 44.3% of adults over 30 years of age have prediabetes with impaired fasting glucose or glycosylated hemoglobin (HbA1c) levels of 5.7% to 6.4% [1]. However, 35% of adults with diabetes, identified by an HbA1c level ≥6.5%, are undiagnosed, and only 25% of those achieve the HbA1c target of less than 6.5% [1]. Diabetes management involves improving individual health status and quality of life through the prevention and early detection of diabetes as well as the prevention or delay of complications via proper glycemic control. Simultaneously, this includes appropriate management of various comorbidities such as blood pressure (BP), lipids, and body weight. Since 1990, the KDA has continuously published treatment guidelines to achieve these treatment goals. These guidelines are targeted at adults with either type 1 diabetes mellitus (T1DM) or type 2 diabetes mellitus (T2DM), as well as children or adolescents with T2DM, and patients with gestational diabetes.
- The Committee of Clinical Practice Guidelines of KDA has carried forward the “2021 Clinical practice guideline for diabetes (7th edition)” [2] and incorporated recent clinical evidence through systematic literature reviews to publish the revised “2023 Clinical practice guideline for diabetes (8th edition).” In this edition, we have organized the levels of evidence into four distinct categories based on the design of the key research that provides the evidence. These categories are: “randomized controlled trials (RCTs),” which include systematic reviews and/or meta-analyses of such trials; “non-randomized controlled studies (NRS)”; case series falling under “others”; and “expert opinions”. Additionally, the grade of recommendation is classified either as a “general recommendation (General)” applicable to the majority of subjects, or a “limited recommendation (Limited)” intended for specific subgroups within the target population.
- In the “screenings for diabetes” section, guidelines were updated to recommend screening for diabetes in all adults aged ≥35 years or those aged ≥19 years who have risk factors, reflecting a recent position statement on screening for prediabetes and diabetes in Korean nonpregnant adults announced by the KDA [3]. In the section “glucose monitoring and glycemic target,” the use of continuous glucose monitoring (CGM) devices was emphasized, and target values of key metrics for CGM have been added. In the section on “pharmacologic treatment of T2DM,” the latest medications have been incorporated, and the algorithms, which were divided into four in the previous guidelines, have now been combined and displayed as one. In cases where intensified injectable therapy is required for people with T2DM who have not reached their glycemic target despite a combination of oral antidiabetic drugs, the recommendation has been changed to prioritize the use of glucagon-like peptide-1 receptor agonist (GLP-1RA) over basal insulin. In the sections “obesity, hypertension, and lipid management,” recent guidelines from other professional medical societies have been reflected [4-6]. The section “non-alcoholic fatty liver disease (NAFLD)” has been updated to include a new algorithm for evaluating NAFLD in people with T2DM. For the practical implementation and widespread use of these guidelines, we separately created an appendix compiling useful information and educational materials for people with diabetes and healthcare professionals.
INTRODUCTION AND SUMMARY OF REVISIONS
- Annual screening (Expert opinion, General) for diabetes should be conducted for adults aged ≥35 and adults aged ≥19 with risk factors (Others, General) using fasting plasma glucose, HbA1c, and 2-hour plasma glucose during a 75 g oral glucose tolerance test (NRS, General). The risk factors of T2DM are shown in Table 1, and abdominal obesity (waist circumference ≥90 cm for men, ≥85 cm for women) has been added compared to the previous guidelines. Owing to the recent increase in the prevalence of prediabetes, diabetes, obesity, and abdominal obesity among young adults under the age of 40 [1,7], there have been suggestions for a change in previous screening criteria for diabetes (adults aged ≥40 and adults aged ≥30 years with risk factors) [2]. The Committee of Clinical Practice Guidelines of the KDA conducted a cross-sectional study on the age for diabetes screening in adults aged ≥20 years using data from the Korean National Health and Nutrition Examination Survey (KNHANES, 2016 to 2020) and the Korean National Health Insurance Service sample cohort (2012 to 2017) [3]. In this study, when evaluating the number needed to screen (NNS) to identify one patient with diabetes according to age group, there was a significant change in NNS values in the 35 to 39 age group. Moreover, when evaluating the NNS for diabetes based on risk factors for T2DM in adults aged 20 to 34 using the KNHANES data, it was found that the NNS was lower at age 23 for abdominal obesity compared to an NNS of age 34 for general obesity (body mass index [BMI] ≥25 kg/m2). Based on these results, it was concluded that screening for diabetes is appropriate in adults aged ≥35 years and those aged ≥20 years with risk factors for T2DM. Applying the revised age criteria, we found that the number of missed participants in diabetes screening significantly decreased from 4.0% to 0.2%, without a significant increase in the NNS value, compared to the previous guideline standards.
SCREENING FOR DIABETES MELLITUS
- Strict glucose control is implemented to prevent microvascular and macrovascular complications in patients with diabetes (RCT, General) [8-10]. Therefore, the long-term maintenance of glycemic control within the near-normal range is critical for patients with diabetes [11]. The recommended optimal HbA1c target is <6.5% for patients with T2DM and <7.0% for those with T1DM (RCT, General) through lifestyle modifications and glucose-lowering agents, especially in recently diagnosed or young people without severe complications or hypoglycemia. However, the glycemic target should be individualized based on physical or psychological status, social circumstances, life expectancy, severity of comorbidities, or risk of hypoglycemia (NRS, General). In patients with a long duration of diabetes, a history of severe hypoglycemia, advanced diabetic complications, short life expectancy, or advanced age, consideration should be given to setting lower glycemic control targets [12-14].
- In addition to HbA1c and blood glucose monitoring, real-time CGM is recommended to achieve better glycemic control and reduce the risk of hypoglycemia in adults with T1DM (RCT, General) and T2DM (RCT, Limited) treated with insulin injections [15-18]. In adults with diabetes receiving insulin therapy who cannot or do not wish to use real-time CGM continuously or in adults with T2DM receiving non-insulin therapy, real-time CGM can be used periodically for glycemic control (RCT, Limited) [19-21]. Intermittently scanned CGM may be used in patients with diabetes and indications for real-time CGM because it is also beneficial for glycemic control and preventing hypoglycemia [22-24] and is available at a lower cost. However, in a randomized controlled study that compared real-time CGM with intermittently scanned CGM, the time below range (below 70 mg/dL) and the time in range (70 to 180 mg/dL) were found to be better with real-time CGM [25]. Therefore, the use of real-time CGM is recommended in cases where insufficient benefits are obtained from intermittently scanned CGM. The recommended target values for the CGM metrics based on the type of diabetes are listed in Table 2.
GLUCOSE MONITORING AND GLYCEMIC TARGET
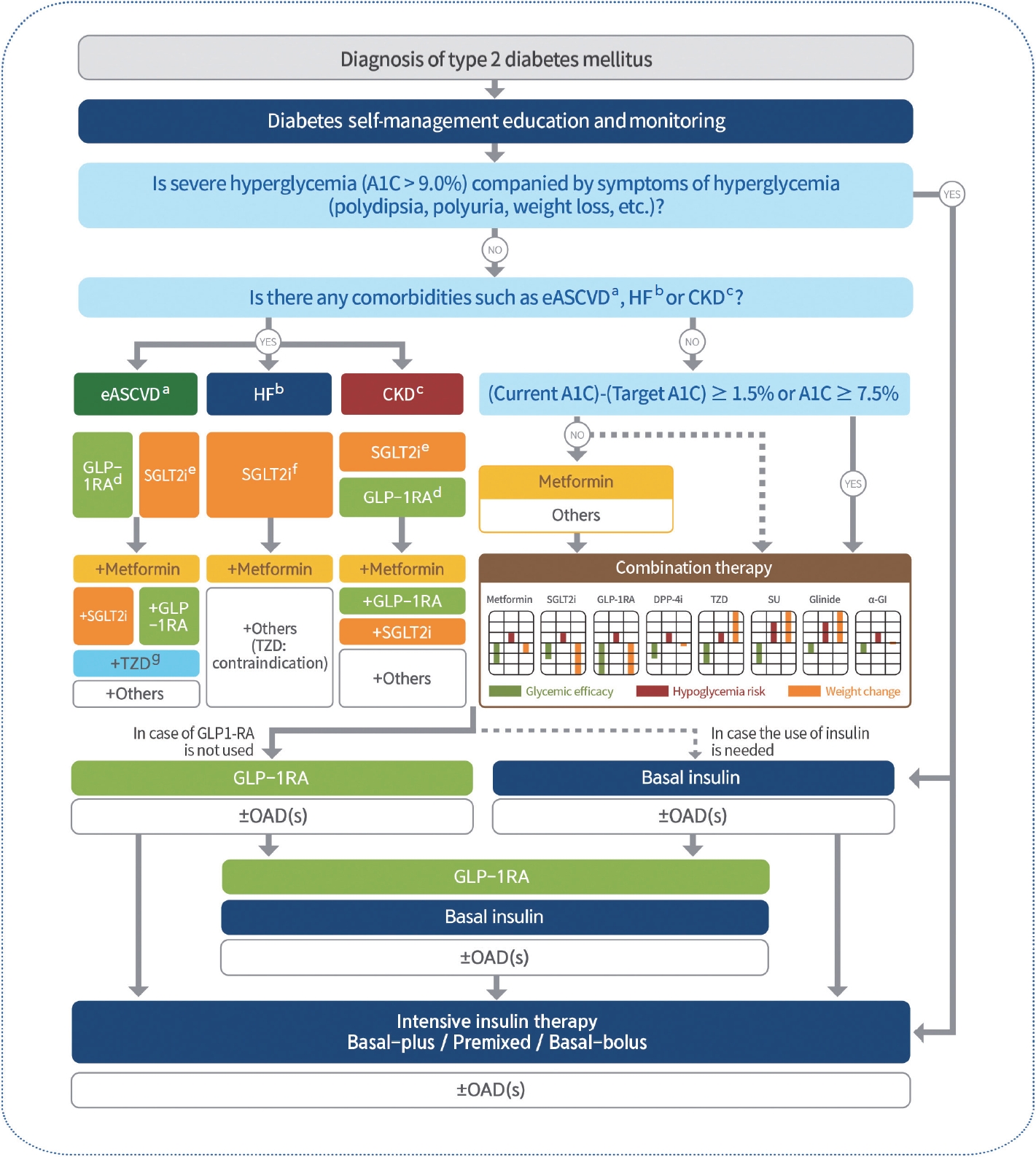
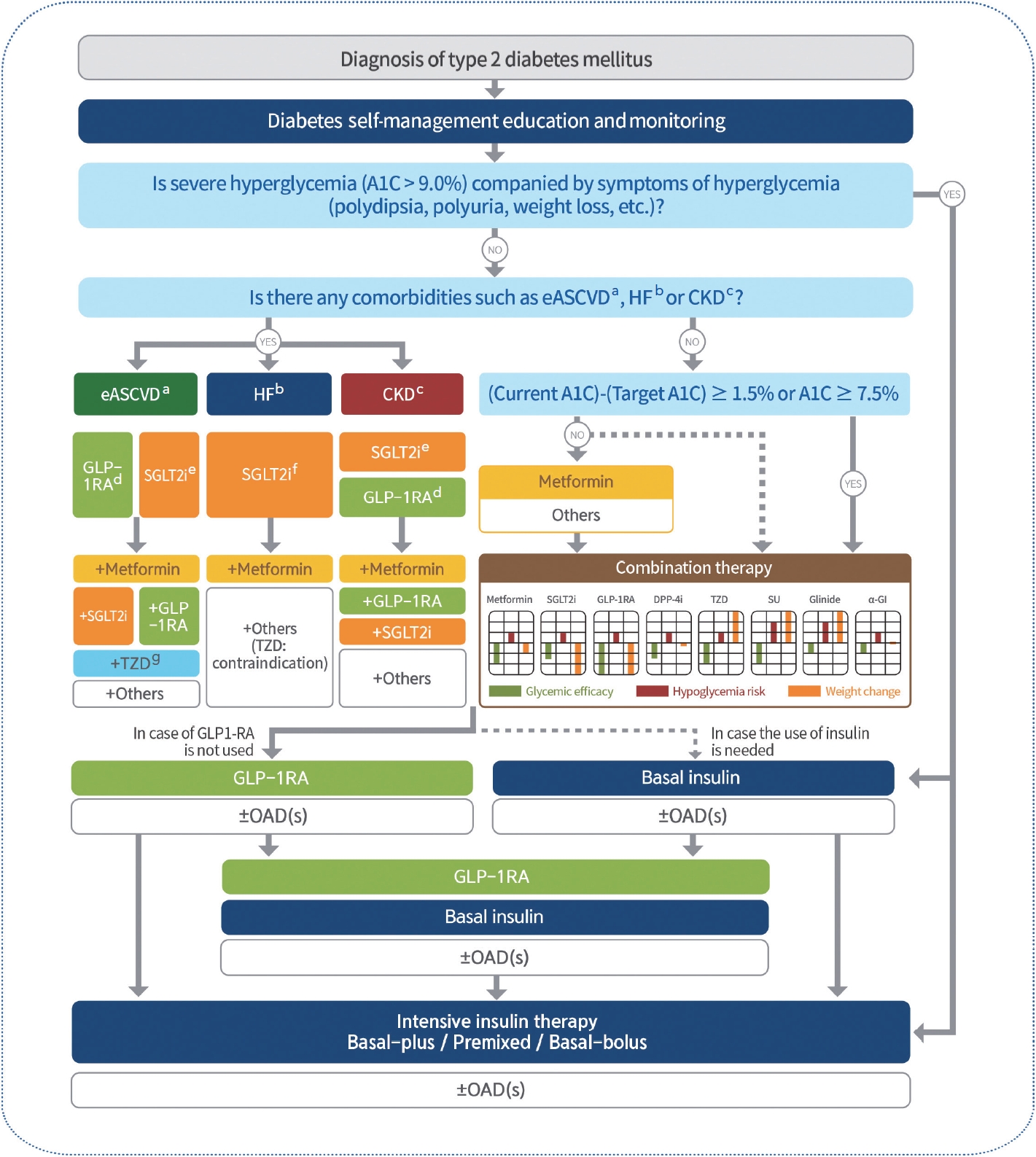
- Immediately upon diagnosis, actively educate patients on self-management methods and monitor whether it is maintained (RCT, General). When selecting drugs, consider the presence of comorbidities (established atherosclerotic cardiovascular disease [eASCVD], heart failure [HF], and chronic kidney disease [CKD]), glucose-lowering efficacy, effects on body weight, risk of hypoglycemia, side effects, treatment acceptability, age, value of life pursued by patients, and cost (Expert opinion, General) [26-38]. Insulin therapy is recommended for patients with severe hyperglycemia (HbA1c >9.0%) and hyperglycemic symptoms (polydipsia, polyuria, and weight loss) (Expert opinion, General) [39,40]. When initiating pharmacological therapy, monotherapy or combination therapy should be administered, taking into consideration the goal and current levels of HbA1c (RCT, General). Generally, the glucose-lowering efficacy (reduction in HbA1c) of monotherapy with an oral glucose-lowering agent is estimated to be 1.0%; therefore, if the current HbA1c level is 1.5% higher than the target HbA1c level, initial combination therapy is recommended [39,41]. However, early combination therapy should be actively considered from the beginning of the diagnosis to reduce the risk of glycemic control failure (RCT, Limited). The Vildagliptin Efficacy in combination with metfoRmIn for earlY treatment of type 2 diabetes (VERIFY) trial demonstrated that an early intervention strategy with combination therapy of vildagliptin and metformin in treatment-naïve patients with T2DM provided more durable long-term clinical benefits than metformin monotherapy with a traditional stepwise regimen [42]. According to a subgroup analysis of Korean patients with newly diagnosed T2DM among the VERIFY trial participants, early combination treatment significantly and consistently improved long-term glycemic durability compared to monotherapy with metformin [43]. Adherence to glucose-lowering agents is strongly associated with metabolic control in patients with T2DM. For each 10% increase in drug adherence, HbA1c levels decreased by 0.16% [44]. Therefore, medication adherence should be evaluated regularly, and medication adjustment should not be delayed if necessary (Expert opinion, General). If the target HbA1c level has not been reached within 3 to 6 months, uptitration of existing medications, combination therapy using drugs with different mechanisms of action, or injection therapy should be actively considered as soon as possible; however, dipeptidyl peptidase-4 (DPP-4) inhibitors and GLP-1RAs should not be combined (RCT, General).
- Metformin is recommended as a first-line glucose-lowering agent in patients with T2DM and is maintained if there are no contraindications or intolerable side effects (RCT, General). In the Practical Evidence of Antidiabetic Monotherapy (PEAM) study, the glucose-lowering efficacy of sulfonylureas, metformin, and thiazolidinediones as monotherapies administered for 48 weeks was similar in drug-naïve Korean patients with T2DM [45]. Metformin has adequate efficacy, a low-risk of hypoglycemia, weight neutrality, and cost-effectiveness. However, if there are contraindications or intolerable side effects of metformin, a different class of medication can be considered.
- Injectable therapy, GLP-1RA or insulin, is recommended when potent glucose-lowering efficacy is required (RCT, General) [46]. When considering injectable-based combination therapy, GLP-1RAs are preferred over basal insulin (RCT, General) [47]. If the glycemic target is not achieved with GLP-1RA or basal insulin alone, the two drugs can be combined (RCT, Limited) [48-65]. If the glycemic target is not achieved with GLP-1RA or basal insulin, intensive insulin therapy such as a basal-plus, premixed, or basal-bolus regimen should be initiated (RCT, Limited) [66-72].
- Sodium-glucose cotransporter 2 (SGLT2) inhibitors with proven benefits for HF should be used first in patients with HF regardless of HbA1c levels and should be maintained as long as there are no contraindications or side effects (RCT, General). In the Dapagliflozin and Prevention of Adverse outcomes in Heart Failure (DAPA-HF) study, conducted in 4,744 patients with existing HF (New York Heart Association [NYHA] class II, III, or IV) and reduced ejection fraction (EF ≤40%) regardless of the presence of T2DM, dapagliflozin 10 mg reduced the risk of HF exacerbation or death from cardiovascular disease (CVD) by 26% (hazard ratio [HR], 0.74; 95% confidence interval [CI], 0.65 to 0.85; P<0.001) over an average study period of 18.2 months and showed similar results in patients with or without diabetes [73]. Empagliflozin was also evaluated in patients with HF (NYHA class II, III, or IV HF and EF ≤40%) regardless of the presence of diabetes in the EMPagliflozin outcomE tRial in patients with chrOnic heaRt failure with reduced ejection fraction (EMPEROR-Reduced) study. Over an average study period of 16 months, the primary endpoint of death from CVD or hospitalization due to HF exacerbation was 25% less in the empagliflozin treatment group compared to the placebo group (HR, 0.75; 95% CI, 0.65 to 0.86; P<0.001). The effect of empagliflozin was evident regardless of the presence of diabetes [74]. The benefit of SGLT2 inhibitors in HF has also been demonstrated in patients with preserved EF. In the EMPagliflozin outcomE tRial in patients with chrOnic heaRt failure with preserved ejection fraction (EMPEROR-Preserved) study, which targeted patients with NYHA class II–IV HF and an EF of 40% or more, the primary endpoint of death from CVD or hospitalization due to HF exacerbation occurred 25% less in the empagliflozin treatment group compared to the placebo group (HR, 0.79; 95% CI, 0.69 to 0.90; P<0.001) over an average study period of 26 months [75].
- SGLT2 inhibitors with proven renal benefits should be used primarily regardless of the HbA1c level in patients with albuminuria or reduced estimated glomerular filtration rate (eGFR) and should be continued unless contraindicated or side effects are present (RCT, Limited). The Dapagliflozin and Prevention of Adverse Outcomes in Chronic Kidney Disease (DAPA-CKD) study confirmed a 39% reduction in renal endpoints (a decrease of 50% or more in eGFR, end-stage renal disease, or death due to renal disease or CVD) in patients with or without diabetes with CKD (eGFR 25 to 75 mL/min/1.73 m2, urine albumin/creatinine ratio [UACR] 200 to 5,000 mg/g) compared to placebo [76]. The Study of Heart and Kidney Protection with Empagliflozin (EMPA-KIDNEY) included patients with CKD regardless of their diabetes status (eGFR 20 to 45 mL/min/1.73 m2, or if the eGFR is 45 to 90 mL/min/1.73 m2 and the UACR is 200 mg/g or more). The primary endpoint, a composite of worsening kidney function or death due to CVD, was reduced by 18% compared to placebo (HR, 0.72; 95% CI, 0.64 to 0.82; P <0.001). Notably, the EMPA-KIDNEY study included patients with decreased eGFR without proteinuria and confirmed beneficial results in renal protection [77].
- GLP-1RAs or SGLT2 inhibitors, which have proven cardiovascular benefits, should be primarily used in patients with eASCVD (RCT, General). In the Empagliflozin Cardiovascular Outcome Event Trial in Type 2 Diabetes Mellitus Patients–Removing Excess Glucose (EMPA-REG OUTCOME) trial, a randomized controlled study that administered the SGLT2 inhibitor empagliflozin to 7,020 patients with T2DM with established CVD, it was observed that over an average of 3 years, the occurrence of 3-point major adverse cardiovascular diseases (MACE; including cardiovascular death, nonfatal myocardial infarction, nonfatal stroke) decreased by 14% compared to the placebo group (HR, 0.86; 95% CI, 0.74 to 0.99; P=0.04) [26]. The Liraglutide Effect and Action in Diabetes: Evaluation of CV Outcome Results (LEADER) study was a double-blind study that randomly assigned liraglutide and placebo to 9,340 adult patients with T2DM. The 3-point MACE was decreased by 13% in the liraglutide group compared to placebo group (HR, 0.87; 95% CI, 0.78 to 0.97), with cardiovascular death (HR, 0.78; 95% CI, 0.66 to 0.93), asymptomatic/nonfatal/fatal myocardial infarction (HR, 0.86; 95% CI, 0.73 to 1.00), and nonfatal/fatal stroke (HR, 0.89; 95% CI, 0.71 to 1.06). All-cause mortality decreased by 15% in the liraglutide group compared to the placebo group (HR, 0.85; 95% CI, 0.74 to 0.97), mainly due to decreased cardiovascular death [27]. The Trial to Evaluate CV and Other Long-term Outcomes With Semaglutide in Subjects With T2D (SUSTAIN-6) was a double-blind study that randomly assigned semaglutide and placebo to 3,297 adult patients with T2DM. Of the patients, 72% had baseline atherosclerotic cardiovascular disease (ASCVD). The 3-point MACE was decreased by 26% in the semaglutide group compared to the placebo group (HR, 0.74; 95% CI, 0.58 to 0.95), with each element showing cardiovascular death (HR, 0.98; 95% CI, 0.65 to 1.48), nonfatal myocardial infarction (HR, 0.74; 95% CI, 0.51 to 1.08), and nonfatal stroke (HR, 0.61; 95% CI, 0.38 to 0.99). All-cause mortality in the semaglutide group compared to the placebo group had a HR of 1.05 (95% CI, 0.74 to 1.50) [78]. The Researching CV Events With a Weekly Incretin in Diabetes (REWIND) was a double-blind study that randomly assigned dulaglutide and placebo to 9,901 adult patients with T2DM. Unlike the two studies above, baseline ASCVD was present in only 31% of all patients, and most had risk factors for ASCVD but not for ASCVD [4]. The 3-point MACE was decreased by 12% in the dulaglutide group compared to the placebo group (HR, 0.88; 95% CI, 0.79 to 0.99), and cardiovascular death (HR, 0.91; 95% CI, 0.7 to 1.06), nonfatal/fatal myocardial infarction (HR, 0.96; 95% CI, 0.79 to 1.15) were not statistically significant; however, the risk of nonfatal/fatal stroke decreased by 24% (HR, 0.76; 95% CI, 0.62 to 0.94). These reductions in MACE were consistent regardless of the presence of baseline ASCVD. In the REWIND study, 69% of the participants were adults with T2DM who did not have underlying ASCVD, and MACE was also reduced even in these cases (HR, 0.87; 95% CI, 0.74 to 1.02 for both; P for interaction=0.97) [28]. Therefore, dulaglutide could be considered for both secondary and primary prevention. However, there are no other large-scale RCTs for patients without ASCVD at baseline; therefore, further research is needed (Fig. 1).
PHARMACOLOGICAL TREATMENT FOR ADULTS WITH T2DM
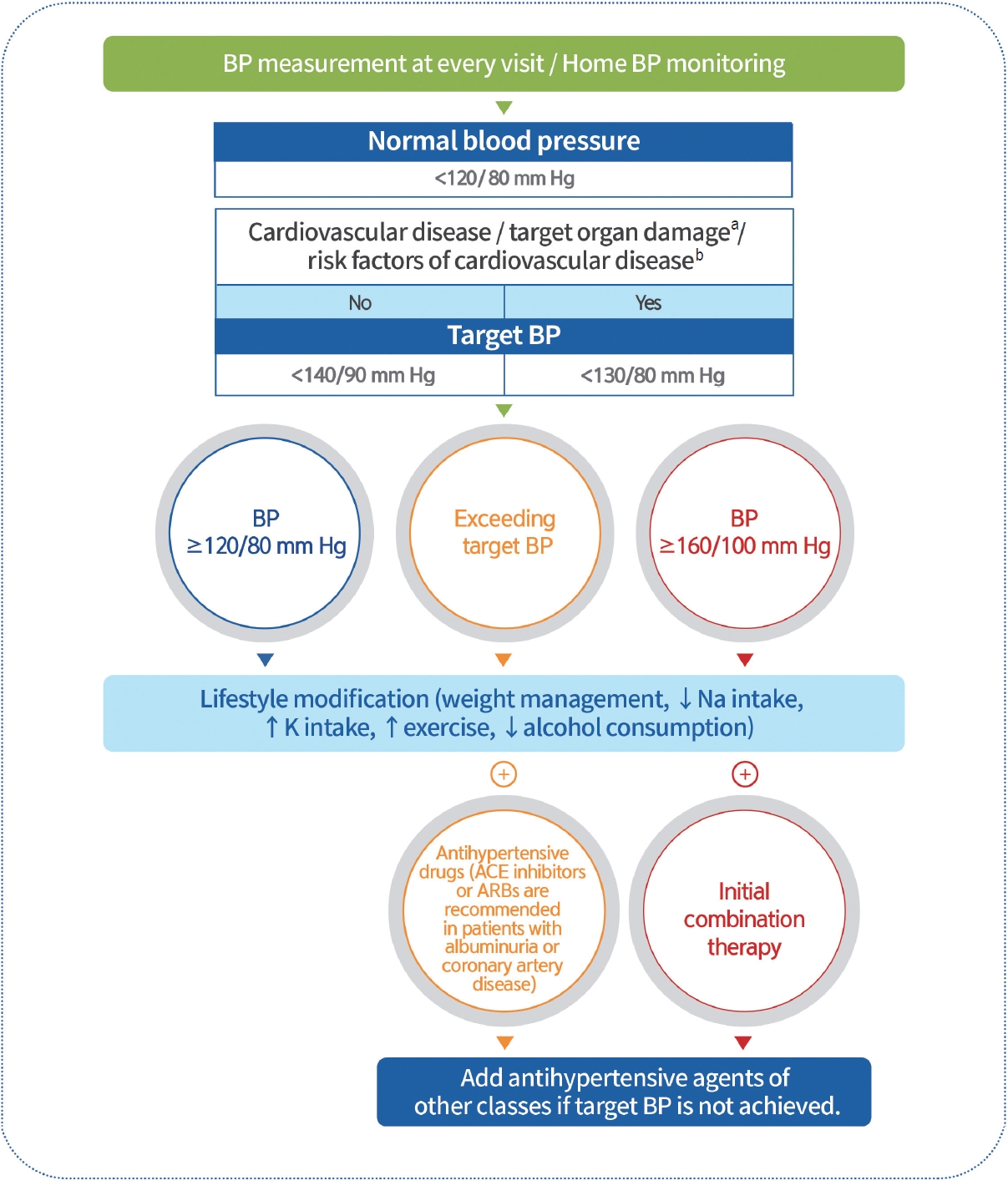
- BP should be measured at every clinic visit and at home (Expert opinion, General). Home BP monitoring is recommended in adults with diabetes and hypertension (RCT, General) [79]. The recommended target BP level is <140/90 mm Hg in adults with diabetes without CVD or its risk factors (RCT, General) [5]. The recommended target BP level is <130/80 mm Hg in adults with diabetes with CVD, target organ damage (albuminuria, CKD, retinopathy, and left ventricular hypertrophy [LVH]), or risk factors for CVD (RCT, General) [5,80-86]. Adults with diabetes and BP ≥120/80 mm Hg should undergo lifestyle modifications, including weight management, proper exercise, and healthy diets, to maintain a normal BP (systolic BP <120 mm Hg and diastolic BP <80 mm Hg) (RCT, General). Pharmacological therapy should be implemented if the target BP is not achieved. Adults with diabetes and hypertension can be prescribed any class of antihypertensive medication as a primary medication for BP control to achieve the target range (RCT, General). There was no difference in the CVD prevention effect between angiotensin-converting enzyme (ACE) inhibitors, angiotensin II receptor blockers (ARBs), calcium channel blockers, and β-blockers, which can all be used as first-line antihypertensive agents in T2DM [87,88]. ACE inhibitors or ARBs are preferred when hypertension is accompanied by albuminuria (RCT, General) [89-91] or coronary artery disease (RCT, General) [92]. If BP is not controlled by the primary antihypertensive medication, combination therapy using a drug with a different mechanism is recommended (RCT, General). However, the combination of ACE inhibitors and ARBs is not recommended (RCT, General). If BP exceeds 160/100 mm Hg, initial combination therapy with two or more medications is recommended with intensive lifestyle intervention (RCT, General) (Fig. 2) [85].
HYPERTENSION MANAGEMENT IN PATIENTS WITH DIABETES
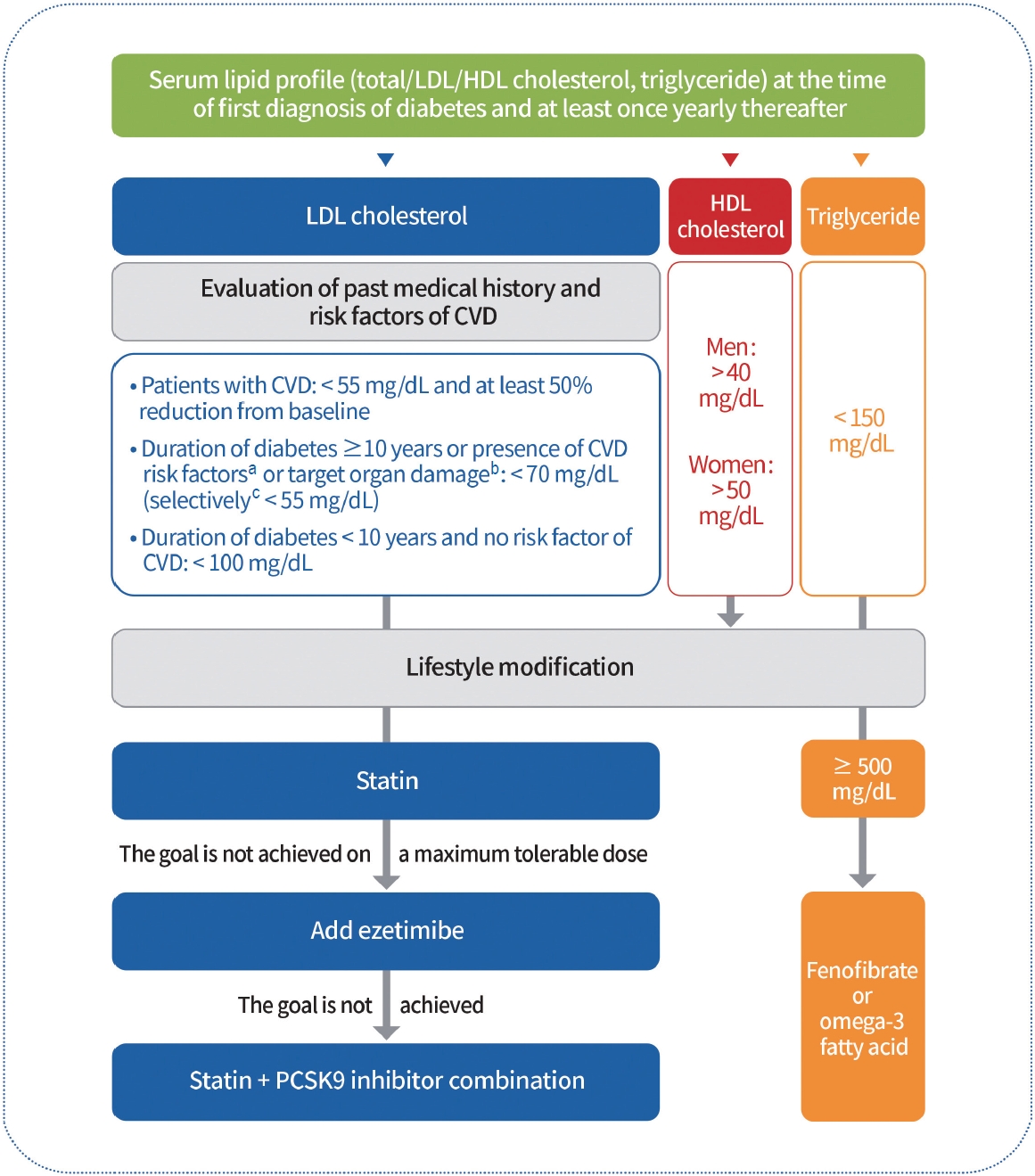
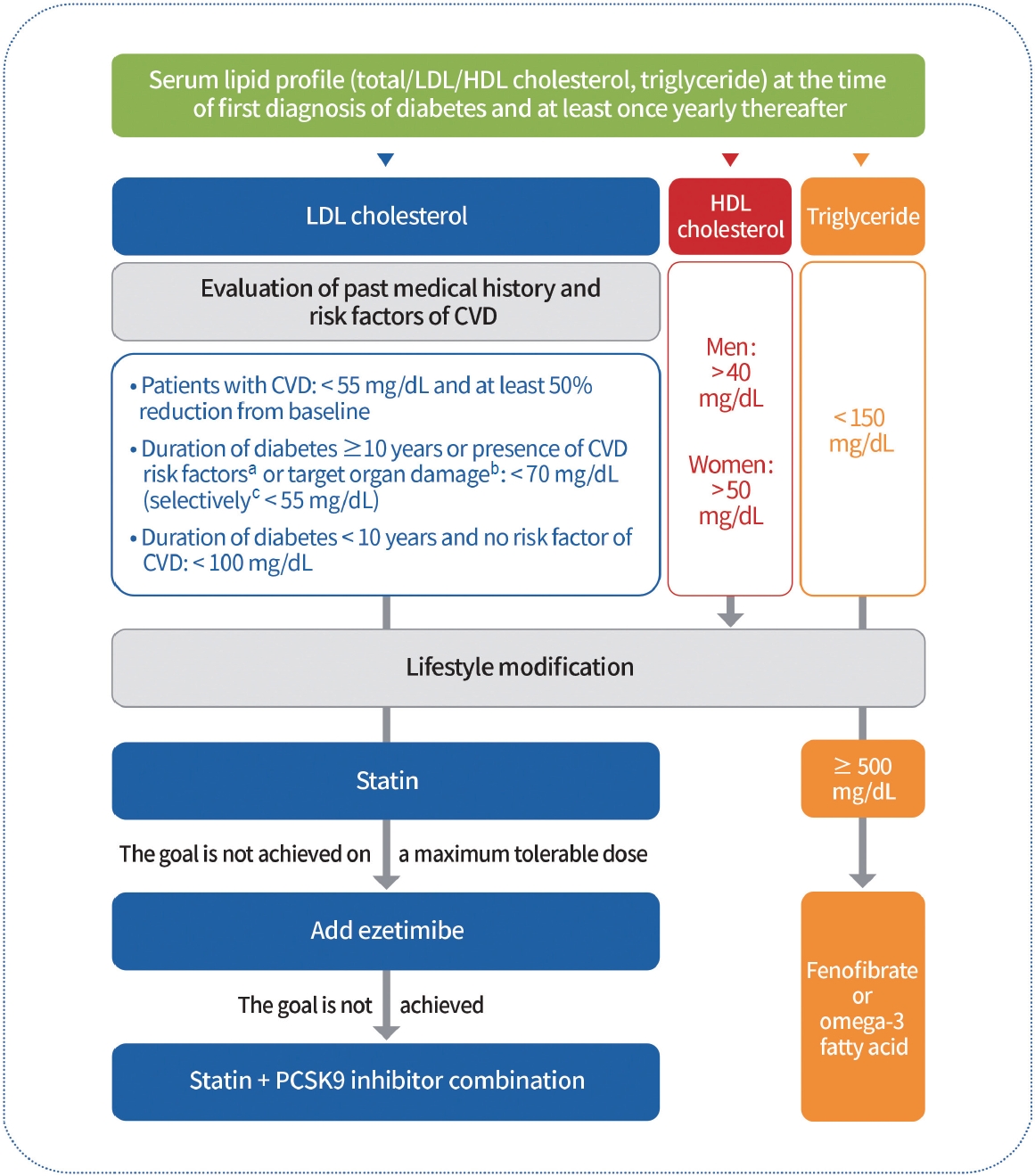
- To evaluate the risk of CVD, serum lipid profiling (total cholesterol, high-density lipoprotein cholesterol [HDL-C], triglycerides, and low-density lipoprotein cholesterol [LDL-C]) should be performed at the time of the initial diagnosis of diabetes and at least once a year thereafter (Expert opinion, General). The primary objective of lipid management is to control LDL-C levels (RCT, General). To determine the LDL-C goal, comorbidities including past history of CVD, target organ damage (albuminuria, eGFR <60 mL/min/1.73 m 2 , retinopathy, and LVH), major risk factors for CVD (age, family history of early-onset coronary artery disease, hypertension, smoking, and HDL-C <40 mg/dL), and duration of diabetes should be investigated first (Expert opinion, General). LDL-C goals are as follows. (1) For patients with CVD, LDL-C should be reduced to <55 mg/dL and at least 50% from baseline (RCT, General); (2) For those with a duration of diabetes ≥10 years or with the major risk factors for CVD or target organ damage, LDL-C should be reduced to <70 mg/dL (NRS, General); (3) For those who have target organ damage or three or more major risk factors for CVD, LDL-C can be reduced to <55 mg/dL (NRS, General); (4) For those whose duration of the disease is <10 years and who do not have major risk factors for CVD, LDL-C should be reduced to <100 mg/dL (RCT, General) [6,93-98]. Education on active lifestyle modifications and continuous monitoring of their implementation should be included in lipid management (RCT, general). Pharmacologic therapy should be implemented if LDL-C goals are not achieved as follows: (1) a statin should be used as first-line therapy (RCT, General); (2) ezetimibe should be added if the goal is not achieved with a maximum tolerable dose of statin therapy (RCT, Limited); (3) if patients with diabetes with CVD do not achieve the goal even after treatment with a statin adding ezetimibe, combination therapy with a statin and proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors should be considered (RCT, Limited) [99-104]. Adults with hypertriglyceridemia (triglyceride levels ≥150 mg/dL) should be managed first with lifestyle modifications, such as stopping alcohol consumption and losing weight, as well as controlling secondary factors, such as glycemic control (RCT, General). Adults with severe hypertriglyceridemia (triglyceride levels ≥500 mg/dL) are treated with medications such as fenofibrate or omega-3 fatty acids to reduce the risk of acute pancreatitis (RCT, General) [105]. Four to 12 weeks after the initiation of lipid-lowering therapy, serum lipid tests must be performed to evaluate the response to the drug and patient compliance (Expert opinion, General) (Fig. 3).
LIPID MANAGEMENT IN PATIENTS WITH DIABETES
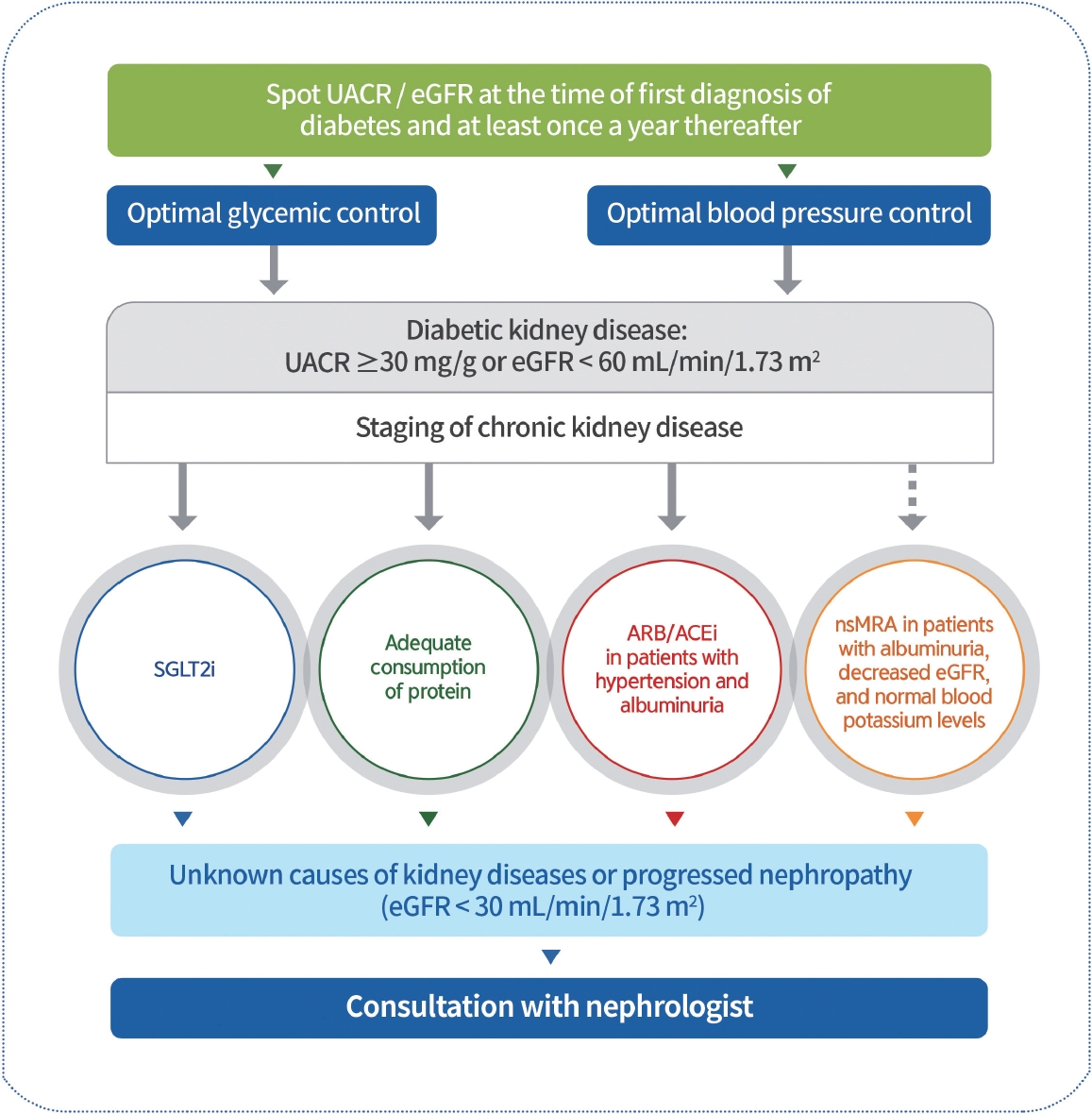
- UACR and eGFR should be evaluated in patients with T2DM at the time of diagnosis and at least once yearly thereafter (NRS, General) [106]. Blood glucose and BP should be optimally controlled to suppress the development and progression of diabetic kidney disease (DKD) (RCT, General) [107]. Patients with DKD should avoid excessively high or low ( ≤0.8 g/kg/day) consumption of protein (RCT, General) [108,109]. ACE inhibitors or ARBs should be prescribed to patients with diabetes with albuminuria and hypertension (RCT, General) [110-112]. To prevent DKD progression, ACE inhibitors or ARBs are not recommended for patients with normal BP (RCT, General) [113]. SGLT2 inhibitors with renal benefits should be used to inhibit the progression of DKD in patients with albuminuria or a reduced eGFR (RCT, General) [76,77]. SGLT2 inhibitors can be maintained until renal replacement therapies are initiated (RCT, General). Nonsteroidal mineralocorticoid receptor antagonists (e.g., finerenone) that have shown cardiac and renal benefits can be considered in T2DM patients with albuminuria, decreased eGFR, and normal blood potassium levels (RCT, General) [114-116]. GLP-1RAs that have shown cardiovascular and renal benefits can be considered to inhibit the progression of albuminuria in T2DM patients at a high-risk of CVD (RCT, General) [28,117,118]. Request a consultation with nephrologists about those with unknown causes of kidney diseases or progressed nephropathy (eGFR <30 mL/min/1.73 m2) (Expert opinion, General) (Fig. 4).
DIABETIC KIDNEY DISEASE
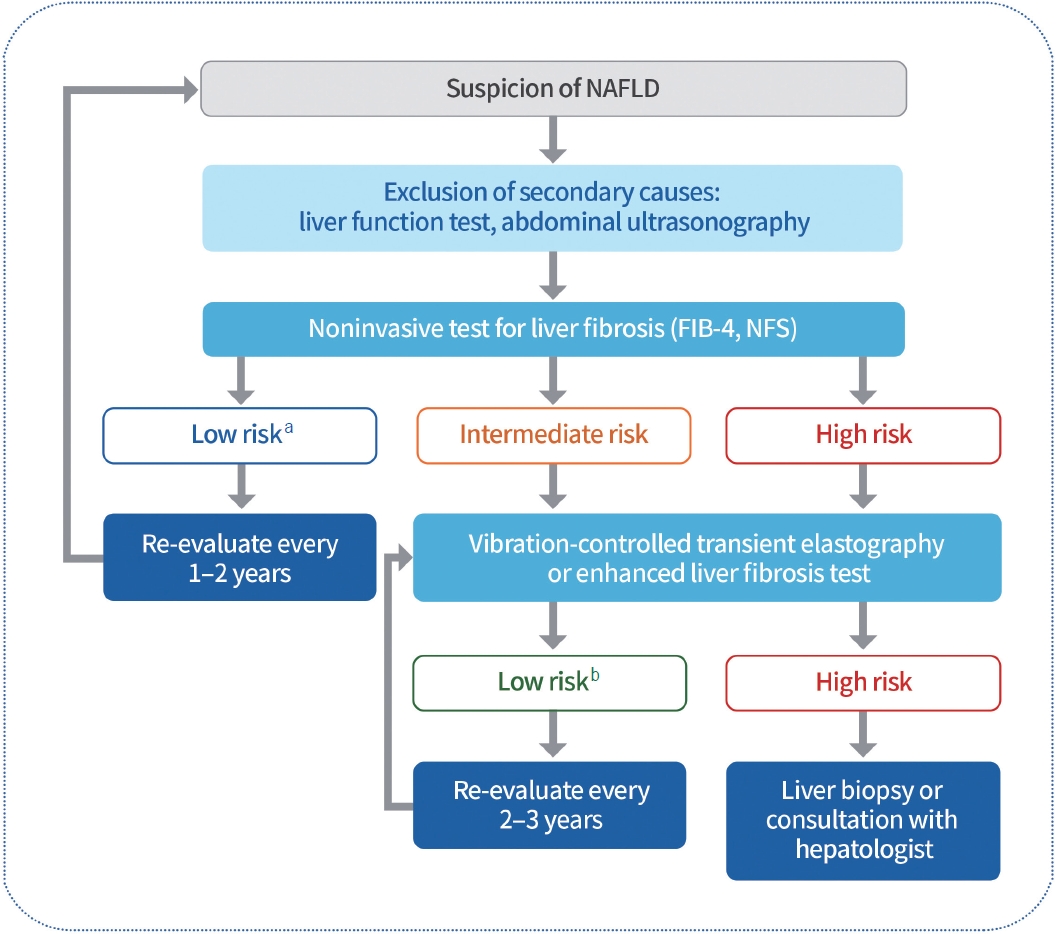
- All adults with T2DM should be evaluated for the presence of NAFLD (Expert opinion, General). Alanine aminotransferase or abdominal ultrasonography should be performed as primary screening to evaluate NAFLD and exclude secondary causes (Expert opinion, General) [119-122]. If NAFLD is confirmed, the evaluation of liver fibrosis is necessary. Non-invasive and relatively simple tests, such as the fibrosis index-4 (FIB-4) or NAFLD fibrosis score (NFS), can be utilized as markers. Compared to liver biopsy, these non-invasive diagnostic models have higher specificity but lower sensitivity [123-125]. Therefore, additional diagnostic strategies for liver fibrosis are necessary for the remainder of the group, excluding the low-risk group (FIB-4 <1.3, NFS <2.67) [126]. Vibration-controlled transient elastography should be considered for the evaluation of liver fibrosis in adults with T2DM with NAFLD (Expert opinion, Limited) (Fig. 5) [127,128]. Lifestyle modification is recommended to reduce the risk factors for CVD and treat fatty liver disease in adults with T2DM with NAFLD (RCT, General) [129-132]. Weight reduction should be performed by at least 7% of the body weight to improve intrahepatic inflammation in adults with T2DM with NAFLD and a BMI ≥23 kg/m2 (RCT, General) [132-134]. Thiazolidinediones can be used as first-line therapy for NAFLD in T2DM adults (RCT, General) [135,136]. GLP-1RAs that have shown effects can be used as first-line therapy for NAFLD in T2DM adults (RCT, Limited) [28-30]. Metformin, DPP-4 inhibitors, vitamin E, statins, ursodeoxycholic acid, and pentoxifylline are not used to treat NAFLD (RCT, General) [134,135,137,138]. Bariatric surgery can be considered for adults with T2DM with obesity (BMI ≥30 kg/m2) and NAFLD who have had non-surgical treatment but failed weight loss and had no improvement in the fatty liver (NRS, Limited) [139-142].
NON-ALCOHOLIC FATTY LIVER DISEASE IN PATIENTS WITH T2DM
- Despite remarkable advances in pharmacological treatment, medical technology, and the ongoing updating of comprehensive guidelines for managing diabetes mellitus, the rate of achieving treatment goals remains unsatisfactory. Therefore, certified education by professional and multidisciplinary teams and constant monitoring of adherence to self-management, including nutrition and exercise, in people with diabetes should be emphasized. An appropriate choice, active titration, and adherence to antidiabetic medication while avoiding clinical inertia could lead to an individualized target glycemic goal. To achieve these goals, various supplementary methods, including information technology, can be helpful. In addition, regular monitoring and early detection of acute or chronic complications and comorbidities are urgently needed in patients with diabetes. The Clinical Practice Guidelines of KDA will provide timely, evidence-based clinical recommendations to support healthcare professionals in providing more advanced diabetes care in Korea.
CONCLUSIONS
-
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
FUNDING
This work was supported by the Korean Diabetes Association.
NOTES
-
Acknowledgements
- We thank the Research Groups and Committees of the Korean Diabetes Association (KDA), and external academic groups for their thoughtful peer review and endorsement of the guidelines: the KDA research group on Diabetic Neuropathy, Diabetic Nephropathy, Gestational Diabetes, Exercise, Diabetes in Old Age, Fatty Liver Disease; the KDA Committee of Education, Food and Nutrition, Patient Advocacy, Medical Practitioners; the Korean Association of Internal Medicine, Korean Endocrine Society, Korean Society for the Study of Obesity, Korean Association of Ophthalmology, Korean Society of Hypertension, Korean Society of Lipid and Atherosclerosis, Korean Society of Nephrology; Korean Association of Diabetes Dietetic Educators, Korean Association of Diabetes Nurse Educators, Korean Society of Social Workers for Diabetes Education. We also thank Hyun Jung Kim, a clinical guideline methodology expert; Seong Ouk Lee and Youngjin Lee, professional librarians; and Seung-Hyun Ko, Hyuk Sang Kwon, and Seak Ki Yun, advisory members along with Se Hee Min and Min Young Lee, members of the Committee of Clinical Practice Guidelines.

| Variable |
T1DM and T2DM |
Older or high-risk (T1DM or T2DM) |
Pregnancy in T1DMc |
Pregnancy in T2DM or GDMd |
||||
|---|---|---|---|---|---|---|---|---|
| Glucose range, mg/dL | Target % in range | Glucose range, mg/dL | Target % in range | Glucose range, mg/dL | Target % in range | Glucose range, mg/dL | Target % in range | |
| Level 2 hyperglycemia | >250 | <5 | >250 | <10 | No data | |||
| Level 1 hyperglycemia | >180 | <25a | >180 | <50 | >140 | <25 | >140 | |
| In target | 70–180 | >70 | 70–180 | >50 | 63–140 | >70 | 63–140 | |
| Level 1 hypoglycemia | <70 | <4b | <70 | <1 | <63 | <4b | <63 | |
| Level 2 hypoglycemia | <54 | <1 | <54 | <1 | <54 | |||
T1DM, type 1 diabetes mellitus; T2DM, type 2 diabetes mellitus; GDM, gestational diabetes mellitus.
a Proportion including Level 2 hyperglycemia,
b Proportion including Level 2 hypoglycemia,
c The target range is based on limited evidence. More research is needed,
d No target range ratio is provided for pregnant women with T2DM or gestational diabetes owing to the limited evidence available.
- 1. Bae JH, Han KD, Ko SH, Yang YS, Choi JH, Choi KM, et al. Diabetes fact sheet in Korea 2021. Diabetes Metab J 2022;46:417-26.ArticlePubMedPMCPDF
- 2. Hur KY, Moon MK, Park JS, Kim SK, Lee SH, Yun JS, et al. 2021 Clinical practice guidelines for diabetes mellitus of the Korean Diabetes Association. Diabetes Metab J 2021;45:461-81.ArticlePubMedPMCPDF
- 3. Lee KA, Kim DJ, Han K, Chon S, Moon MK; Committee of Clinical Practice Guideline of Korean Diabetes Association. Screening for prediabetes and diabetes in Korean nonpregnant adults: a position statement of the Korean Diabetes Association, 2022. Diabetes Metab J 2022;46:819-26.ArticlePubMedPMCPDF
- 4. Kim BY, Kang SM, Kang JH, Kang SY, Kim KK, Kim KB, et al. 2020 Korean Society for the Study of Obesity guidelines for the management of obesity in Korea. J Obes Metab Syndr 2021;30:81-92.ArticlePubMedPMC
- 5. Kim HL, Lee EM, Ahn SY, Kim KI, Kim HC, Kim JH, et al. The 2022 focused update of the 2018 Korean Hypertension Society guidelines for the management of hypertension. Clin Hypertens 2023;29:11.ArticlePubMedPMCPDF
- 6. Yang YS, Kim HL, Kim SH, Moon MK. Lipid management in Korean people with type 2 diabetes mellitus: Korean Diabetes Association and Korean Society of Lipid and Atherosclerosis Consensus Statement. Diabetes Metab J 2023;47:1-9.ArticlePubMedPMCPDF
- 7. Yang YS, Han BD, Han K, Jung JH, Son JW. Obesity fact sheet in Korea, 2021: trends in obesity prevalence and obesity-related comorbidity incidence stratified by age from 2009 to 2019. J Obes Metab Syndr 2022;31:169-77.ArticlePubMedPMC
- 8. Diabetes Control and Complications Trial Research Group, Nathan DM, Genuth S, Lachin J, Cleary P, Crofford O, et al. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med 1993;329:977-86.ArticlePubMed
- 9. UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet 1998;352:837-53.ArticlePubMed
- 10. Ohkubo Y, Kishikawa H, Araki E, Miyata T, Isami S, Motoyoshi S, et al. Intensive insulin therapy prevents the progression of diabetic microvascular complications in Japanese patients with non-insulin-dependent diabetes mellitus: a randomized prospective 6-year study. Diabetes Res Clin Pract 1995;28:103-17.ArticlePubMed
- 11. Holman RR, Paul SK, Bethel MA, Matthews DR, Neil HA. 10-Year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med 2008;359:1577-89.ArticlePubMed
- 12. Hayward RA, Reaven PD, Wiitala WL, Bahn GD, Reda DJ, Ge L, et al. Follow-up of glycemic control and cardiovascular outcomes in type 2 diabetes. N Engl J Med 2015;372:2197-206.ArticlePubMed
- 13. Lee AK, Warren B, Lee CJ, McEvoy JW, Matsushita K, Huang ES, et al. The association of severe hypoglycemia with incident cardiovascular events and mortality in adults with type 2 diabetes. Diabetes Care 2018;41:104-11.ArticlePubMedPDF
- 14. Writing Group for the DCCT/EDIC Research Group, Orchard TJ, Nathan DM, Zinman B, Cleary P, Brillon D, et al. Association between 7 years of intensive treatment of type 1 diabetes and long-term mortality. JAMA 2015;313:45-53.ArticlePubMedPMC
- 15. Heinemann L, Freckmann G, Ehrmann D, Faber-Heinemann G, Guerra S, Waldenmaier D, et al. Real-time continuous glucose monitoring in adults with type 1 diabetes and impaired hypoglycaemia awareness or severe hypoglycaemia treated with multiple daily insulin injections (HypoDE): a multicentre, randomised controlled trial. Lancet 2018;391:1367-77.ArticlePubMed
- 16. Battelino T, Phillip M, Bratina N, Nimri R, Oskarsson P, Bolinder J. Effect of continuous glucose monitoring on hypoglycemia in type 1 diabetes. Diabetes Care 2011;34:795-800.ArticlePubMedPMCPDF
- 17. Seyed Ahmadi S, Westman K, Pivodic A, Olafsdottir AF, Dahlqvist S, Hirsch IB, et al. The association between HbA1c and time in hypoglycemia during CGM and self-monitoring of blood glucose in people with type 1 diabetes and multiple daily insulin injections: a randomized clinical trial (GOLD-4). Diabetes Care 2020;43:2017-24.ArticlePubMedPMCPDF
- 18. Beck RW, Riddlesworth TD, Ruedy K, Ahmann A, Haller S, Kruger D, et al. Continuous glucose monitoring versus usual care in patients with type 2 diabetes receiving multiple daily insulin injections: a randomized trial. Ann Intern Med 2017;167:365-74.ArticlePubMed
- 19. Vigersky RA, Fonda SJ, Chellappa M, Walker MS, Ehrhardt NM. Short- and long-term effects of real-time continuous glucose monitoring in patients with type 2 diabetes. Diabetes Care 2012;35:32-8.ArticlePubMedPDF
- 20. Ehrhardt NM, Chellappa M, Walker MS, Fonda SJ, Vigersky RA. The effect of real-time continuous glucose monitoring on glycemic control in patients with type 2 diabetes mellitus. J Diabetes Sci Technol 2011;5:668-75.ArticlePubMedPMCPDF
- 21. Yoo HJ, An HG, Park SY, Ryu OH, Kim HY, Seo JA, et al. Use of a real time continuous glucose monitoring system as a motivational device for poorly controlled type 2 diabetes. Diabetes Res Clin Pract 2008;82:73-9.ArticlePubMed
- 22. Bolinder J, Antuna R, Geelhoed-Duijvestijn P, Kroger J, Weitgasser R. Novel glucose-sensing technology and hypoglycaemia in type 1 diabetes: a multicentre, non-masked, randomised controlled trial. Lancet 2016;388:2254-63.ArticlePubMed
- 23. Haak T, Hanaire H, Ajjan R, Hermanns N, Riveline JP, Rayman G. Flash glucose-sensing technology as a replacement for blood glucose monitoring for the management of insulin-treated type 2 diabetes: a multicenter, open-label randomized controlled trial. Diabetes Ther 2017;8:55-73.ArticlePubMedPDF
- 24. Yaron M, Roitman E, Aharon-Hananel G, Landau Z, Ganz T, Yanuv I, et al. Effect of flash glucose monitoring technology on glycemic control and treatment satisfaction in patients with type 2 diabetes. Diabetes Care 2019;42:1178-84.ArticlePubMedPDF
- 25. Haskova A, Radovnicka L, Petruzelkova L, Parkin CG, Grunberger G, Horova E, et al. Real-time CGM is superior to flash glucose monitoring for glucose control in type 1 diabetes: the CORRIDA Randomized Controlled Trial. Diabetes Care 2020;43:2744-50.ArticlePubMedPMCPDF
- 26. Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, Hantel S, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med 2015;373:2117-28.ArticlePubMed
- 27. Marso SP, Daniels GH, Brown-Frandsen K, Kristensen P, Mann JF, Nauck MA, et al. Liraglutide and cardiovascular outcomes in type 2 diabetes. N Engl J Med 2016;375:311-22.ArticlePubMedPMC
- 28. Gerstein HC, Colhoun HM, Dagenais GR, Diaz R, Lakshmanan M, Pais P, et al. Dulaglutide and cardiovascular outcomes in type 2 diabetes (REWIND): a double-blind, randomised placebo-controlled trial. Lancet 2019;394:121-30.PubMed
- 29. Maloney A, Rosenstock J, Fonseca V. A model-based meta-analysis of 24 antihyperglycemic drugs for type 2 diabetes: comparison of treatment effects at therapeutic doses. Clin Pharmacol Ther 2019;105:1213-23.ArticlePubMedPDF
- 30. Egede LE, Gebregziabher M, Echols C, Lynch CP. Longitudinal effects of medication nonadherence on glycemic control. Ann Pharmacother 2014;48:562-70.ArticlePubMedPDF
- 31. Huber CA, Reich O. Medication adherence in patients with diabetes mellitus: does physician drug dispensing enhance quality of care?: evidence from a large health claims database in Switzerland. Patient Prefer Adherence 2016;10:1803-9.ArticlePubMedPMC
- 32. Iglay K, Cartier SE, Rosen VM, Zarotsky V, Rajpathak SN, Radican L, et al. Meta-analysis of studies examining medication adherence, persistence, and discontinuation of oral antihyperglycemic agents in type 2 diabetes. Curr Med Res Opin 2015;31:1283-96.ArticlePubMed
- 33. McGovern A, Tippu Z, Hinton W, Munro N, Whyte M, de Lusignan S. Systematic review of adherence rates by medication class in type 2 diabetes: a study protocol. BMJ Open 2016;6:e010469.ArticlePubMedPMC
- 34. Khunti K, Seidu S, Kunutsor S, Davies M. Association between adherence to pharmacotherapy and outcomes in type 2 diabetes: a meta-analysis. Diabetes Care 2017;40:1588-96.ArticlePubMedPDF
- 35. Polonsky WH, Henry RR. Poor medication adherence in type 2 diabetes: recognizing the scope of the problem and its key contributors. Patient Prefer Adherence 2016;10:1299-307.ArticlePubMedPMC
- 36. McGovern A, Tippu Z, Hinton W, Munro N, Whyte M, de Lusignan S. Comparison of medication adherence and persistence in type 2 diabetes: a systematic review and meta-analysis. Diabetes Obes Metab 2018;20:1040-3.ArticlePubMedPDF
- 37. Lasalvia P, Barahona-Correa JE, Romero-Alvernia DM, Gil-Tamayo S, Castaneda-Cardona C, Bayona JG, et al. Pen devices for insulin self-administration compared with needle and vial: systematic review of the literature and meta-analysis. J Diabetes Sci Technol 2016;10:959-66.ArticlePubMedPMCPDF
- 38. ElSayed NA, Aleppo G, Aroda VR, Bannuru RR, Brown FM, Bruemmer D, et al. 4. Comprehensive medical evaluation and assessment of comorbidities: standards of care in diabetes-2023. Diabetes Care 2023;46(Suppl 1):S49-67.
- 39. Weng J, Li Y, Xu W, Shi L, Zhang Q, Zhu D, et al. Effect of intensive insulin therapy on beta-cell function and glycaemic control in patients with newly diagnosed type 2 diabetes: a multicentre randomised parallel-group trial. Lancet 2008;371:1753-60.PubMed
- 40. Kramer CK, Zinman B, Retnakaran R. Short-term intensive insulin therapy in type 2 diabetes mellitus: a systematic review and meta-analysis. Lancet Diabetes Endocrinol 2013;1:28-34.ArticlePubMed
- 41. Holman RR, Thorne KI, Farmer AJ, Davies MJ, Keenan JF, Paul S, et al. Addition of biphasic, prandial, or basal insulin to oral therapy in type 2 diabetes. N Engl J Med 2007;357:1716-30.ArticlePubMed
- 42. Matthews DR, Paldanius PM, Proot P, Chiang Y, Stumvoll M, Del Prato S, et al. Glycaemic durability of an early combination therapy with vildagliptin and metformin versus sequential metformin monotherapy in newly diagnosed type 2 diabetes (VERIFY): a 5-year, multicentre, randomised, double-blind trial. Lancet 2019;394:1519-29.ArticlePubMed
- 43. Yoo SJ, Chang SA, Sohn TS, Kwon HS, Lee JM, Moon S, et al. Long-term glycaemic durability of early combination therapy strategy versus metformin monotherapy in Korean patients with newly diagnosed type 2 diabetes mellitus. Diabetes Metab J 2021;45:954-9.ArticlePubMedPDF
- 44. Schectman JM, Nadkarni MM, Voss JD. The association between diabetes metabolic control and drug adherence in an indigent population. Diabetes Care 2002;25:1015-21.ArticlePubMedPDF
- 45. Yoon KH, Shin JA, Kwon HS, Lee SH, Min KW, Ahn YB, et al. Comparison of the efficacy of glimepiride, metformin, and rosiglitazone monotherapy in Korean drug-naive type 2 diabetic patients: the practical evidence of antidiabetic monotherapy study. Diabetes Metab J 2011;35:26-33.ArticlePubMedPMC
- 46. Tsapas A, Avgerinos I, Karagiannis T, Malandris K, Manolopoulos A, Andreadis P, et al. Comparative effectiveness of glucose-lowering drugs for type 2 diabetes: a systematic review and network meta-analysis. Ann Intern Med 2020;173:278-86.PubMed
- 47. Nauck MA, Mirna AE, Quast DR. Meta-analysis of head-to-head clinical trials comparing incretin-based glucose-lowering medications and basal insulin: an update including recently developed glucagon-like peptide-1 (GLP-1) receptor agonists and the glucose-dependent insulinotropic polypeptide/GLP-1 receptor co-agonist tirzepatide. Diabetes Obes Metab 2023;25:1361-71.PubMed
- 48. DeVries JH, Bain SC, Rodbard HW, Seufert J, D’Alessio D, Thomsen AB, et al. Sequential intensification of metformin treatment in type 2 diabetes with liraglutide followed by randomized addition of basal insulin prompted by A1C targets. Diabetes Care 2012;35:1446-54.ArticlePubMedPMCPDF
- 49. Aroda VR, Bailey TS, Cariou B, Kumar S, Leiter LA, Raskin P, et al. Effect of adding insulin degludec to treatment in patients with type 2 diabetes inadequately controlled with metformin and liraglutide: a double-blind randomized controlled trial (BEGIN: ADD TO GLP-1 Study). Diabetes Obes Metab 2016;18:663-70.PubMedPMC
- 50. Rosenstock J, Aronson R, Grunberger G, Hanefeld M, Piatti P, Serusclat P, et al. Benefits of lixilan, a titratable fixed-ratio combination of insulin glargine plus lixisenatide, versus insulin glargine and lixisenatide monocomponents in type 2 diabetes inadequately controlled on oral agents: the LixiLan-O Randomized Trial. Diabetes Care 2016;39:2026-35.ArticlePubMedPDF
- 51. Blonde L, Rosenstock J, Del Prato S, Henry R, Shehadeh N, Frias J, et al. Switching to iGlarLixi versus continuing daily or weekly GLP-1 RA in type 2 diabetes inadequately controlled by GLP-1 RA and oral antihyperglycemic therapy: the LixiLan-G Randomized Clinical Trial. Diabetes Care 2019;42:2108-16.ArticlePubMedPDF
- 52. Gough SC, Bode B, Woo V, Rodbard HW, Linjawi S, Poulsen P, et al. Efficacy and safety of a fixed-ratio combination of insulin degludec and liraglutide (IDegLira) compared with its components given alone: results of a phase 3, open-label, randomised, 26-week, treat-to-target trial in insulin-naive patients with type 2 diabetes. Lancet Diabetes Endocrinol 2014;2:885-93.ArticlePubMed
- 53. Linjawi S, Bode BW, Chaykin LB, Courreges JP, Handelsman Y, Lehmann LM, et al. The efficacy of IDegLira (insulin Degludec/Liraglutide combination) in adults with type 2 diabetes inadequately controlled with a GLP-1 receptor agonist and oral therapy: DUAL III Randomized Clinical Trial. Diabetes Ther 2017;8:101-14.ArticlePubMedPDF
- 54. Buse JB, Bergenstal RM, Glass LC, Heilmann CR, Lewis MS, Kwan AY, et al. Use of twice-daily exenatide in Basal insulin-treated patients with type 2 diabetes: a randomized, controlled trial. Ann Intern Med 2011;154:103-12.ArticlePubMed
- 55. Seino Y, Min KW, Niemoeller E, Takami A; EFC10887 GETGOAL-L Asia Study Investigators. Randomized, double-blind, placebo-controlled trial of the once-daily GLP-1 receptor agonist lixisenatide in Asian patients with type 2 diabetes insufficiently controlled on basal insulin with or without a sulfonylurea (GetGoal-L-Asia). Diabetes Obes Metab 2012;14:910-7.PubMedPMC
- 56. Riddle MC, Aronson R, Home P, Marre M, Niemoeller E, Miossec P, et al. Adding once-daily lixisenatide for type 2 diabetes inadequately controlled by established basal insulin: a 24-week, randomized, placebo-controlled comparison (GetGoal-L). Diabetes Care 2013;36:2489-96.PubMedPMC
- 57. Riddle MC, Forst T, Aronson R, Sauque-Reyna L, Souhami E, Silvestre L, et al. Adding once-daily lixisenatide for type 2 diabetes inadequately controlled with newly initiated and continuously titrated basal insulin glargine: a 24-week, randomized, placebo-controlled study (GetGoal-Duo 1). Diabetes Care 2013;36:2497-503.PubMedPMC
- 58. Yang W, Min K, Zhou Z, Li L, Xu X, Zhu D, et al. Efficacy and safety of lixisenatide in a predominantly Asian population with type 2 diabetes insufficiently controlled with basal insulin: the GetGoal-L-C randomized trial. Diabetes Obes Metab 2018;20:335-43.PubMed
- 59. Ahmann A, Rodbard HW, Rosenstock J, Lahtela JT, de Loredo L, Tornoe K, et al. Efficacy and safety of liraglutide versus placebo added to basal insulin analogues (with or without metformin) in patients with type 2 diabetes: a randomized, placebo-controlled trial. Diabetes Obes Metab 2015;17:1056-64.ArticlePubMedPMCPDF
- 60. Pozzilli P, Norwood P, Jodar E, Davies MJ, Ivanyi T, Jiang H, et al. Placebo-controlled, randomized trial of the addition of once-weekly glucagon-like peptide-1 receptor agonist dulaglutide to titrated daily insulin glargine in patients with type 2 diabetes (AWARD-9). Diabetes Obes Metab 2017;19:1024-31.PubMed
- 61. Rodbard HW, Lingvay I, Reed J, de la Rosa R, Rose L, Sugimoto D, et al. Semaglutide added to basal insulin in type 2 diabetes (SUSTAIN 5): a randomized, controlled trial. J Clin Endocrinol Metab 2018;103:2291-301.ArticlePubMedPMC
- 62. Aroda VR, Rosenstock J, Wysham C, Unger J, Bellido D, Gonzalez-Galvez G, et al. Efficacy and safety of lixilan, a titratable fixed-ratio combination of insulin glargine plus lixisenatide in type 2 diabetes inadequately controlled on basal insulin and metformin: the LixiLan-L Randomized Trial. Diabetes Care 2016;39:1972-80.ArticlePubMedPDF
- 63. Rosenstock J, Diamant M, Aroda VR, Silvestre L, Souhami E, Zhou T, et al. Efficacy and safety of lixilan, a titratable fixed-ratio combination of lixisenatide and insulin glargine, versus insulin glargine in type 2 diabetes inadequately controlled on metformin monotherapy: the LixiLan Proof-of-Concept Randomized Trial. Diabetes Care 2016;39:1579-86.ArticlePubMedPMCPDF
- 64. Buse JB, Vilsboll T, Thurman J, Blevins TC, Langbakke IH, Bottcher SG, et al. Contribution of liraglutide in the fixed-ratio combination of insulin degludec and liraglutide (IDegLira). Diabetes Care 2014;37:2926-33.ArticlePubMedPDF
- 65. Lingvay I, Perez Manghi F, Garcia-Hernandez P, Norwood P, Lehmann L, Tarp-Johansen MJ, et al. Effect of insulin glargine up-titration vs insulin degludec/liraglutide on glycated hemoglobin levels in patients with uncontrolled type 2 diabetes: the DUAL V Randomized Clinical Trial. JAMA 2016;315:898-907.ArticlePubMed
- 66. Owens DR, Luzio SD, Sert-Langeron C, Riddle MC. Effects of initiation and titration of a single pre-prandial dose of insulin glulisine while continuing titrated insulin glargine in type 2 diabetes: a 6-month ‘proof-of-concept’ study. Diabetes Obes Metab 2011;13:1020-7.ArticlePubMedPMC
- 67. Lankisch MR, Ferlinz KC, Leahy JL, Scherbaum WA; Orals Plus Apidra and LANTUS (OPAL) study group. Introducing a simplified approach to insulin therapy in type 2 diabetes: a comparison of two single-dose regimens of insulin glulisine plus insulin glargine and oral antidiabetic drugs. Diabetes Obes Metab 2008;10:1178-85.ArticlePubMed
- 68. Leahy JL. Insulin therapy in type 2 diabetes mellitus. Endocrinol Metab Clin North Am 2012;41:119-44.ArticlePubMed
- 69. Giugliano D, Maiorino MI, Bellastella G, Chiodini P, Ceriello A, Esposito K. Efficacy of insulin analogs in achieving the hemoglobin A1c target of <7% in type 2 diabetes: meta-analysis of randomized controlled trials. Diabetes Care 2011;34:510-7.PubMedPMC
- 70. Davidson MB, Raskin P, Tanenberg RJ, Vlajnic A, Hollander P. A stepwise approach to insulin therapy in patients with type 2 diabetes mellitus and basal insulin treatment failure. Endocr Pract 2011;17:395-403.ArticlePubMed
- 71. Castellana M, Cignarelli A, Brescia F, Laviola L, Giorgino F. GLP-1 receptor agonist added to insulin versus basal-plus or basal-bolus insulin therapy in type 2 diabetes: a systematic review and meta-analysis. Diabetes Metab Res Rev 2019;35:e3082.PubMed
- 72. Rosenstock J, Nino A, Soffer J, Erskine L, Acusta A, Dole J, et al. Impact of a weekly glucagon-like peptide 1 receptor agonist, albiglutide, on glycemic control and on reducing prandial insulin use in type 2 diabetes inadequately controlled on multiple insulin therapy: a randomized trial. Diabetes Care 2020;43:2509-18.ArticlePubMedPMC
- 73. McMurray JJ, Solomon SD, Inzucchi SE, Kober L, Kosiborod MN, Martinez FA, et al. Dapagliflozin in patients with heart failure and reduced ejection fraction. N Engl J Med 2019;381:1995-2008.PubMed
- 74. Packer M, Anker SD, Butler J, Filippatos G, Pocock SJ, Carson P, et al. Cardiovascular and renal outcomes with empagliflozin in heart failure. N Engl J Med 2020;383:1413-24.PubMed
- 75. Anker SD, Butler J, Filippatos G, Ferreira JP, Bocchi E, Bohm M, et al. Empagliflozin in heart failure with a preserved ejection fraction. N Engl J Med 2021;385:1451-61.PubMed
- 76. Heerspink HJ, Stefansson BV, Correa-Rotter R, Chertow GM, Greene T, Hou FF, et al. Dapagliflozin in patients with chronic kidney disease. N Engl J Med 2020;383:1436-46.ArticlePubMed
- 77. The EMPA-KIDNEY Collaborative Group, Herrington WG, Staplin N, Wanner C, Green JB, Hauske SJ, et al. Empagliflozin in patients with chronic kidney disease. N Engl J Med 2023;388:117-27.ArticlePubMed
- 78. Marso SP, Bain SC, Consoli A, Eliaschewitz FG, Jodar E, Leiter LA, et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med 2016;375:1834-44.ArticlePubMed
- 79. Omboni S, Gazzola T, Carabelli G, Parati G. Clinical usefulness and cost effectiveness of home blood pressure telemonitoring: meta-analysis of randomized controlled studies. J Hypertens 2013;31:455-68.PubMed
- 80. Emdin CA, Rahimi K, Neal B, Callender T, Perkovic V, Patel A. Blood pressure lowering in type 2 diabetes: a systematic review and meta-analysis. JAMA 2015;313:603-15.ArticlePubMed
- 81. ACCORD Study Group, Cushman WC, Evans GW, Byington RP, Goff DC Jr, Grimm RH Jr, et al. Effects of intensive blood-pressure control in type 2 diabetes mellitus. N Engl J Med 2010;362:1575-85.ArticlePubMedPMC
- 82. SPRINT Research Group, Wright JT Jr, Williamson JD, Whelton PK, Snyder JK, Sink KM, et al. A randomized trial of intensive versus standard blood-pressure control. N Engl J Med 2015;373:2103-16.ArticlePubMedPMC
- 83. Buckley LF, Dixon DL, Wohlford GF 4th, Wijesinghe DS, Baker WL, Van Tassell BW. Intensive versus standard blood pressure control in SPRINT-Eligible participants of ACCORD-BP. Diabetes Care 2017;40:1733-8.ArticlePubMedPDF
- 84. Whelton PK, Carey RM, Aronow WS, Casey DE Jr, Collins KJ, Dennison Himmelfarb C, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension 2018;71:e13-115.PubMed
- 85. Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, et al. 2018 ESC/ESH guidelines for the management of arterial hypertension: the task force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension: the Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension. J Hypertens 2018;36:1953-2041.PubMed
- 86. Zhang W, Zhang S, Deng Y, Wu S, Ren J, Sun G, et al. Trial of intensive blood-pressure control in older patients with hypertension. N Engl J Med 2021;385:1268-79.ArticlePubMed
- 87. Turnbull F, Neal B, Algert C, Chalmers J, Chapman N, Cutler J, et al. Effects of different blood pressure-lowering regimens on major cardiovascular events in individuals with and without diabetes mellitus: results of prospectively designed overviews of randomized trials. Arch Intern Med 2005;165:1410-9.ArticlePubMed
- 88. Bangalore S, Fakheri R, Toklu B, Messerli FH. Diabetes mellitus as a compelling indication for use of renin angiotensin system blockers: systematic review and meta-analysis of randomized trials. BMJ 2016;352:i438.ArticlePubMedPMC
- 89. Lindholm LH, Ibsen H, Dahlof B, Devereux RB, Beevers G, de Faire U, et al. Cardiovascular morbidity and mortality in patients with diabetes in the Losartan Intervention For Endpoint reduction in hypertension study (LIFE): a randomised trial against atenolol. Lancet 2002;359:1004-10.ArticlePubMed
- 90. Berl T, Hunsicker LG, Lewis JB, Pfeffer MA, Porush JG, Rouleau JL, et al. Cardiovascular outcomes in the Irbesartan Diabetic Nephropathy Trial of patients with type 2 diabetes and overt nephropathy. Ann Intern Med 2003;138:542-9.ArticlePubMed
- 91. Palmer SC, Mavridis D, Navarese E, Craig JC, Tonelli M, Salanti G, et al. Comparative efficacy and safety of blood pressure-lowering agents in adults with diabetes and kidney disease: a network meta-analysis. Lancet 2015;385:2047-56.ArticlePubMed
- 92. Arnold SV, Bhatt DL, Barsness GW, Beatty AL, Deedwania PC, Inzucchi SE, et al. Clinical management of stable coronary artery disease in patients with type 2 diabetes mellitus: a scientific statement from the American Heart Association. Circulation 2020;141:e779-806.ArticlePubMed
- 93. Brugts JJ, Yetgin T, Hoeks SE, Gotto AM, Shepherd J, Westendorp RG, et al. The benefits of statins in people without established cardiovascular disease but with cardiovascular risk factors: meta-analysis of randomised controlled trials. BMJ 2009;338:b2376.ArticlePubMedPMC
- 94. Cholesterol Treatment Trialists’ (CTT) Collaboration, Baigent C, Blackwell L, Emberson J, Holland LE, Reith C, et al. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet 2010;376:1670-81.ArticlePubMedPMC
- 95. Ahmed S, Cannon CP, Murphy SA, Braunwald E. Acute coronary syndromes and diabetes: is intensive lipid lowering beneficial?: results of the PROVE IT-TIMI 22 trial. Eur Heart J 2006;27:2323-9.ArticlePubMed
- 96. Nissen SE, Tuzcu EM, Schoenhagen P, Brown BG, Ganz P, Vogel RA, et al. Effect of intensive compared with moderate lipid-lowering therapy on progression of coronary atherosclerosis: a randomized controlled trial. JAMA 2004;291:1071-80.ArticlePubMed
- 97. Shepherd J, Barter P, Carmena R, Deedwania P, Fruchart JC, Haffner S, et al. Effect of lowering LDL cholesterol substantially below currently recommended levels in patients with coronary heart disease and diabetes: the Treating to New Targets (TNT) study. Diabetes Care 2006;29:1220-6.PubMed
- 98. Moon MK, Noh J, Rhee EJ, Park SH, Kim HC, Kim BJ, et al. Cardiovascular outcomes according to comorbidities and low-density lipoprotein cholesterol in Korean people with type 2 diabetes mellitus. Diabetes Metab J 2023;47:45-58.ArticlePubMedPMCPDF
- 99. Colhoun HM, Betteridge DJ, Durrington PN, Hitman GA, Neil HA, Livingstone SJ, et al. Primary prevention of cardiovascular disease with atorvastatin in type 2 diabetes in the Collaborative Atorvastatin Diabetes Study (CARDS): multicentre randomised placebo-controlled trial. Lancet 2004;364:685-96.ArticlePubMed
- 100. Cholesterol Treatment Trialists’ (CTT) Collaborators, Kearney PM, Blackwell L, Collins R, Keech A, Simes J, et al. Efficacy of cholesterol-lowering therapy in 18,686 people with diabetes in 14 randomised trials of statins: a meta-analysis. Lancet 2008;371:117-25.ArticlePubMed
- 101. Cannon CP, Blazing MA, Giugliano RP, McCagg A, White JA, Theroux P, et al. Ezetimibe added to statin therapy after acute coronary syndromes. N Engl J Med 2015;372:2387-97.ArticlePubMed
- 102. Hong N, Lee YH, Tsujita K, Gonzalez JA, Kramer CM, Kovarnik T, et al. Comparison of the effects of ezetimibe-statin combination therapy on major adverse cardiovascular events in patients with and without diabetes: a meta-analysis. Endocrinol Metab (Seoul) 2018;33:219-27.ArticlePubMedPMCPDF
- 103. Sabatine MS, Giugliano RP, Keech AC, Honarpour N, Wiviott SD, Murphy SA, et al. Evolocumab and clinical outcomes in patients with cardiovascular disease. N Engl J Med 2017;376:1713-22.ArticlePubMed
- 104. Schwartz GG, Steg PG, Szarek M, Bhatt DL, Bittner VA, Diaz R, et al. Alirocumab and cardiovascular outcomes after acute coronary syndrome. N Engl J Med 2018;379:2097-107.ArticlePubMed
- 105. ElSayed NA, Aleppo G, Aroda VR, Bannuru RR, Brown FM, Bruemmer D, et al. 10. Cardiovascular disease and risk management: standards of care in diabetes-2023. Diabetes Care 2023;46(Suppl 1):S158-90.
- 106. Stevens PE, Levin A; Kidney Disease: Improving Global Outcomes Chronic Kidney Disease Guideline Development Work Group Members. Evaluation and management of chronic kidney disease: synopsis of the kidney disease: improving global outcomes 2012 clinical practice guideline. Ann Intern Med 2013;158:825-30.ArticlePubMed
- 107. UK Prospective Diabetes Study Group. Tight blood pressure control and risk of macrovascular and microvascular complications in type 2 diabetes: UKPDS 38. BMJ 1998;317:703-13.ArticlePubMedPMC
- 108. Kasiske BL, Lakatua JD, Ma JZ, Louis TA. A meta-analysis of the effects of dietary protein restriction on the rate of decline in renal function. Am J Kidney Dis 1998;31:954-61.ArticlePubMed
- 109. Wheeler ML, Dunbar SA, Jaacks LM, Karmally W, Mayer-Davis EJ, Wylie-Rosett J, et al. Macronutrients, food groups, and eating patterns in the management of diabetes: a systematic review of the literature, 2010. Diabetes Care 2012;35:434-45.PubMedPMC
- 110. Lewis EJ, Hunsicker LG, Bain RP, Rohde RD. The effect of angiotensin-converting-enzyme inhibition on diabetic nephropathy. The Collaborative Study Group. N Engl J Med 1993;329:1456-62.ArticlePubMed
- 111. Brenner BM, Cooper ME, de Zeeuw D, Keane WF, Mitch WE, Parving HH, et al. Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy. N Engl J Med 2001;345:861-9.ArticlePubMed
- 112. Heart Outcomes Prevention Evaluation Study Investigators. Effects of ramipril on cardiovascular and microvascular outcomes in people with diabetes mellitus: results of the HOPE study and MICRO-HOPE substudy. Lancet 2000;355:253-9.ArticlePubMed
- 113. Mauer M, Zinman B, Gardiner R, Suissa S, Sinaiko A, Strand T, et al. Renal and retinal effects of enalapril and losartan in type 1 diabetes. N Engl J Med 2009;361:40-51.ArticlePubMedPMC
- 114. Bakris GL, Agarwal R, Anker SD, Pitt B, Ruilope LM, Rossing P, et al. Effect of finerenone on chronic kidney disease outcomes in type 2 diabetes. N Engl J Med 2020;383:2219-29.ArticlePubMed
- 115. Pitt B, Filippatos G, Agarwal R, Anker SD, Bakris GL, Rossing P, et al. Cardiovascular events with finerenone in kidney disease and type 2 diabetes. N Engl J Med 2021;385:2252-63.ArticlePubMed
- 116. Agarwal R, Filippatos G, Pitt B, Anker SD, Rossing P, Joseph A, et al. Cardiovascular and kidney outcomes with finerenone in patients with type 2 diabetes and chronic kidney disease: the FIDELITY pooled analysis. Eur Heart J 2022;43:474-84.ArticlePubMedPDF
- 117. Mann JF, Orsted DD, Brown-Frandsen K, Marso SP, Poulter NR, Rasmussen S, et al. Liraglutide and renal outcomes in type 2 diabetes. N Engl J Med 2017;377:839-48.ArticlePubMed
- 118. Kristensen SL, Rorth R, Jhund PS, Docherty KF, Sattar N, Preiss D, et al. Cardiovascular, mortality, and kidney outcomes with GLP-1 receptor agonists in patients with type 2 diabetes: a systematic review and meta-analysis of cardiovascular outcome trials. Lancet Diabetes Endocrinol 2019;7:776-85.ArticlePubMed
- 119. European Association for the Study of the Liver (EASL); European Association for the Study of Diabetes (EASD); European Association for the Study of Obesity (EASO). EASL-EASD-EASO clinical practice guidelines for the management of non-alcoholic fatty liver disease. Diabetologia 2016;59:1121-40.ArticlePubMedPDF
- 120. Chalasani N, Younossi Z, Lavine JE, Charlton M, Cusi K, Rinella M, et al. The diagnosis and management of nonalcoholic fatty liver disease: practice guidance from the American Association for the Study of Liver Diseases. Hepatology 2018;67:328-57.ArticlePubMedPDF
- 121. Hossain N, Afendy A, Stepanova M, Nader F, Srishord M, Rafiq N, et al. Independent predictors of fibrosis in patients with non-alcoholic fatty liver disease. Clin Gastroenterol Hepatol 2009;7:1224-9.ArticlePubMed
- 122. Hernaez R, Lazo M, Bonekamp S, Kamel I, Brancati FL, Guallar E, et al. Diagnostic accuracy and reliability of ultrasonography for the detection of fatty liver: a meta-analysis. Hepatology 2011;54:1082-90.ArticlePubMed
- 123. Xiao G, Zhu S, Xiao X, Yan L, Yang J, Wu G. Comparison of laboratory tests, ultrasound, or magnetic resonance elastography to detect fibrosis in patients with nonalcoholic fatty liver disease: a meta-analysis. Hepatology 2017;66:1486-501.ArticlePubMedPDF
- 124. Siddiqui MS, Yamada G, Vuppalanchi R, Van Natta M, Loomba R, Guy C, et al. Diagnostic accuracy of noninvasive fibrosis models to detect change in fibrosis stage. Clin Gastroenterol Hepatol 2019;17:1877-85.ArticlePubMedPMC
- 125. Bril F, McPhaul MJ, Caulfield MP, Clark VC, Soldevilla-Pico C, Firpi-Morell RJ, et al. Performance of plasma biomarkers and diagnostic panels for nonalcoholic steatohepatitis and advanced fibrosis in patients with type 2 diabetes. Diabetes Care 2020;43:290-7.ArticlePubMedPDF
- 126. Lee BW, Lee YH, Park CY, Rhee EJ, Lee WY, Kim NH, et al. Non-alcoholic fatty liver disease in patients with type 2 diabetes mellitus: a position statement of the Fatty Liver Research Group of the Korean Diabetes Association. Diabetes Metab J 2020;44:382-401.ArticlePubMedPMCPDF
- 127. Wong VW, Vergniol J, Wong GL, Foucher J, Chan HL, Le Bail B, et al. Diagnosis of fibrosis and cirrhosis using liver stiffness measurement in nonalcoholic fatty liver disease. Hepatology 2010;51:454-62.ArticlePubMed
- 128. Karlas T, Petroff D, Sasso M, Fan JG, Mi YQ, de Ledinghen V, et al. Individual patient data meta-analysis of controlled attenuation parameter (CAP) technology for assessing steatosis. J Hepatol 2017;66:1022-30.ArticlePubMed
- 129. Koutoukidis DA, Astbury NM, Tudor KE, Morris E, Henry JA, Noreik M, et al. Association of weight loss interventions with changes in biomarkers of nonalcoholic fatty liver disease: a systematic review and meta-analysis. JAMA Intern Med 2019;179:1262-71.ArticlePubMedPMC
- 130. Keating SE, Hackett DA, George J, Johnson NA. Exercise and non-alcoholic fatty liver disease: a systematic review and meta-analysis. J Hepatol 2012;57:157-66.ArticlePubMed
- 131. Musso G, Gambino R, Cassader M, Pagano G. A meta-analysis of randomized trials for the treatment of nonalcoholic fatty liver disease. Hepatology 2010;52:79-104.ArticlePubMed
- 132. Thoma C, Day CP, Trenell MI. Lifestyle interventions for the treatment of non-alcoholic fatty liver disease in adults: a systematic review. J Hepatol 2012;56:255-66.ArticlePubMed
- 133. Vilar-Gomez E, Martinez-Perez Y, Calzadilla-Bertot L, Torres-Gonzalez A, Gra-Oramas B, Gonzalez-Fabian L, et al. Weight loss through lifestyle modification significantly reduces features of nonalcoholic steatohepatitis. Gastroenterology 2015;149:367-78.ArticlePubMed
- 134. Musso G, Cassader M, Rosina F, Gambino R. Impact of current treatments on liver disease, glucose metabolism and cardiovascular risk in non-alcoholic fatty liver disease (NAFLD): a systematic review and meta-analysis of randomized trials. Diabetologia 2012;55:885-904.ArticlePubMedPDF
- 135. Musso G, Cassader M, Paschetta E, Gambino R. Thiazolidinediones and advanced liver fibrosis in nonalcoholic steatohepatitis: a meta-analysis. JAMA Intern Med 2017;177:633-40.ArticlePubMedPMC
- 136. Lee YH, Kim JH, Kim SR, Jin HY, Rhee EJ, Cho YM, et al. Lobeglitazone, a novel thiazolidinedione, improves non-alcoholic fatty liver disease in type 2 diabetes: its efficacy and predictive factors related to responsiveness. J Korean Med Sci 2017;32:60-9.ArticlePubMedPDF
- 137. Tang W, Xu Q, Hong T, Tong G, Feng W, Shen S, et al. Comparative efficacy of anti-diabetic agents on nonalcoholic fatty liver disease in patients with type 2 diabetes mellitus: a systematic review and meta-analysis of randomized and non-randomized studies. Diabetes Metab Res Rev 2016;32:200-16.ArticlePubMed
- 138. Li Y, Liu L, Wang B, Wang J, Chen D. Metformin in non-alcoholic fatty liver disease: a systematic review and meta-analysis. Biomed Rep 2013;1:57-64.ArticlePubMed
- 139. Seeberg KA, Borgeraas H, Hofso D, Smastuen MC, Kvan NP, Grimnes JO, et al. Gastric bypass versus sleeve gastrectomy in type 2 diabetes: effects on hepatic steatosis and fibrosis: a randomized controlled trial. Ann Intern Med 2022;175:74-83.ArticlePubMed
- 140. Lassailly G, Caiazzo R, Ntandja-Wandji LC, Gnemmi V, Baud G, Verkindt H, et al. Bariatric surgery provides long-term resolution of nonalcoholic steatohepatitis and regression of fibrosis. Gastroenterology 2020;159:1290-301.ArticlePubMed
- 141. Lee Y, Doumouras AG, Yu J, Brar K, Banfield L, Gmora S, et al. Complete resolution of nonalcoholic fatty liver disease after bariatric surgery: a systematic review and meta-analysis. Clin Gastroenterol Hepatol 2019;17:1040-60.ArticlePubMed
- 142. Cusi K, Isaacs S, Barb D, Basu R, Caprio S, Garvey WT, et al. American Association of Clinical Endocrinology clinical practice guideline for the diagnosis and management of nonalcoholic fatty liver disease in primary care and endocrinology clinical settings: co-sponsored by the American Association for the Study of Liver Diseases (AASLD). Endocr Pract 2022;28:528-62.PubMed
REFERENCES
Figure & Data
References
Citations
- Mortality in metabolic dysfunction-associated steatotic liver disease: A nationwide population-based cohort study
Eugene Han, Byung-Wan Lee, Eun Seok Kang, Bong-Soo Cha, Sang Hoon Ahn, Yong-ho Lee, Seung Up Kim
Metabolism.2024; 152: 155789. CrossRef - Letter by In-Kyung Jeong Regarding Article, Trends in Prevalence of Hypertriglyceridemia and Related Factors in Korean Adults: A Serial Cross-Sectional Study
In-Kyung Jeong
Journal of Lipid and Atherosclerosis.2024; 13(1): 80. CrossRef - Association between cardiovascular disease risk and incident type 2 diabetes mellitus in individuals with prediabetes: A retrospective cohort study
Myung Jin Kim, Yun Kyung Cho, Chang Hee Jung, Woo Je Lee
Diabetes Research and Clinical Practice.2024; 208: 111125. CrossRef - Korea Hypertension Fact Sheet 2023: analysis of nationwide population-based data with a particular focus on hypertension in special populations
Hyeon Chang Kim, Hokyou Lee, Hyeok-Hee Lee, Dasom Son, Minsung Cho, Sojung Shin, Yeeun Seo, Eun-Jin kim, Song Vogue Ahn, Sun Ha Jee, Sungha Park, Hae-Young Lee, Min Ho Shin, Sang-Hyun Ihm, Seung Won Lee, Jong Ku Park, Il Suh, Tae-Yong Lee
Clinical Hypertension.2024;[Epub] CrossRef - Diabetes Duration, Cholesterol Levels, and Risk of Cardiovascular Diseases in Individuals With Type 2 Diabetes
Mee Kyoung Kim, Kyu Na Lee, Kyungdo Han, Seung-Hwan Lee
The Journal of Clinical Endocrinology & Metabolism.2024;[Epub] CrossRef - Effect of Adding Apolipoprotein B Testing on the Prevalence of Dyslipidemia and Risk of Cardiovascular Disease in the Korean Adult Population
Rihwa Choi, Sang Gon Lee, Eun Hee Lee
Metabolites.2024; 14(3): 169. CrossRef - A self-powered and supercapacitive microneedle continuous glucose monitoring system with a wide range of glucose detection capabilities
Hye-Jun Kil, Jang Hyeon Kim, Kanghae Lee, Tae-Uk Kang, Ju-Hyun Yoo, Yong-ho Lee, Jin-Woo Park
Biosensors and Bioelectronics.2024; 257: 116297. CrossRef - Cardiorenal outcomes and mortality after sodium‐glucose cotransporter‐2 inhibitor initiation in type 2 diabetes patients with percutaneous coronary intervention history
Jin Hwa Kim, Young Sang Lyu, BongSeong Kim, Mee Kyung Kim, Sang Yong Kim, Ki‐Hyun Baek, Ki‐Ho Song, Kyungdo Han, Hyuk‐Sang Kwon
Diabetes, Obesity and Metabolism.2024;[Epub] CrossRef - Management of Dyslipidemia in Patients with Diabetes Mellitus
Kyung Ae Lee
The Journal of Korean Diabetes.2023; 24(3): 111. CrossRef - 2023 Clinical Practice Guidelines for Diabetes: Recommendations for Pharmacological Treatment of Type 2 Diabetes
Junghyun Noh
The Journal of Korean Diabetes.2023; 24(3): 127. CrossRef - 2023 Clinical Practice Guidelines for Diabetes
Min Kyong Moon
The Journal of Korean Diabetes.2023; 24(3): 120. CrossRef - 2023 Clinical Practice Guidelines for Diabetes: Management of Cardiovascular Risk Factors
Ye Seul Yang
The Journal of Korean Diabetes.2023; 24(3): 135. CrossRef - A 33-Year-Old Man Presented with Abdominal Pain and Vomiting Starting a Day Ago
Jong Han Choi
The Korean Journal of Medicine.2023; 98(6): 289. CrossRef - Comorbidity Patterns and Management in Inpatients with Endocrine Diseases by Age Groups in South Korea: Nationwide Data
Sung-Soo Kim, Hun-Sung Kim
Journal of Personalized Medicine.2023; 14(1): 42. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite