Urinary Neutrophil Gelatinase-Associated Lipocalin Levels in Comparison with Glomerular Filtration Rate for Evaluation of Renal Function in Patients with Diabetic Chronic Kidney Disease
Article information
Abstract
Background
Neutrophil gelatinase-associated lipocalin (NGAL) is a promising biomarker of acute kidney injury. There is a growing body of evidence suggesting that NGAL is also a marker of kidney disease and severity in chronic kidney disease (CKD). We studied the utility of urinary NGAL in more accurately predicting renal function in patients with diabetic CKD.
Methods
We studied possible relationships between urinary NGAL, estimated glomerular filtration rate (eGFR), and proteinuria in diabetic CKD patients and in healthy populations.
Results
Urinary NGAL levels were significantly higher in CKD patients than in healthy controls (96.0 [2.7 to 975.2] ng/mL vs. 18.8 [1.3 to 81.9] ng/mL, P=0.02), and the GFR was lower among CKD patients (49.3 [13.1 to 78.3] mL/min/1.73 m2 vs. 85.6 [72 to 106.7] mL/min/1.73 m2, P<0.0001). The urinary NGAL level showed a significant inverse correlation with GFR (r=-0.5634, P<0.0001). The correlation analyses between urinary protein level and urinary NGAL levels and GFR were as follows: urine protein and urinary NGAL (r=0.3009, P=0.0256), urine protein and GFR (r=-0.6245, P<0.0001), urine microalbumin and urinary NGAL (r=0.1794, P=0.2275), and urine microalbumin and GFR (r=-0.5190, P=0.0002).
Conclusion
From these results, we concluded that urinary NGAL is a reliable marker of renal function in diabetic CKD patients. However, urinary NGAL did not provide more accurate information regarding renal function than GFR.
INTRODUCTION
Neutrophil gelatinase-associated lipocalin (NGAL) is a member of the lipocalin family that is expressed at low levels in several human tissues and rapidly released from renal tubular cells in response to various insults to the kidney [1,2]. Serum and urinary NGAL are arguably the most promising emerging biomarkers for early detection of acute kidney injury (AKI) [3-7]. Several recent studies have also defined the role of NGAL in chronic kidney disease (CKD) and showed serum and urinary NGAL levels are a marker of kidney disease and severity in CKD [8-12]. In addition, though all forms of CKD are also associated with tubulointerstitial injury, regardless of whether the primary pathology is glomerular or otherwise, it is now widely accepted that in some CKD-associated diseases, such as diabetic nephropathy, the rate of deterioration in renal function and the overall outcome are more accurately associated with the degree of renal tubulointerstitial damage than with the severity of glomerular lesions. These factors suggest that NGAL may have unique predictive value in diabetic nephropathy.
In our study, we assessed urinary NGAL levels in diabetic CKD in order to study whether urinary NGAL is a sensitive biomarker of kidney function in this disease.
METHODS
This study was a single-center, cross-sectional study of patients with diabetic CKD. This study included 56 samples from 31 diabetic CKD patients for whom a serum creatinine and random urine protein test had been requested and 36 samples from healthy populations seen at Dong-A University Hospital between June 2009 and September 2010. Inclusion criterion was the presence of stage 3 to 5 CKD according to the National Kidney Foundation's classification. Patients who were free of cancer and liver, thyroid, or infectious diseases at the time of the study were included. The average duration of diabetes for this group was 14.3 years. The healthy population consisted of samples obtained from the people who visited the hospital for periodic medical checkups and proved to have no specific clinical or laboratory problems. Informed consent was obtained and urine samples were collected. Fresh serum and urine samples were tested for creatinine, glomerular filtration rate (GFR), urinary albumin, and protein at the requested time. Urine protein and albumin were measured by TBA-200FR (TBA-200FR; Toshiba Medical Systems, Tokyo, Japan) and urine albumin/creatinine ratio (UACR) was calculated. The GFR level was calculated using the MDRD formula: MDRD=186×(serum creatinine [mg/dL])-1.154×age-0.203 [13]. A correction factor of 0.742 was used for women. Urine samples were then stored at -70℃ until further testing. Urinary NGAL was measured simultaneously by ARCHITECT NGAL assay (Abbott Laboratories, Abbott Park, IL, USA) implemented on an Abbott Architect immunoanalyzer. All charts of CKD patients and healthy individuals were reviewed. Correlations between urinary NGAL and other variables were evaluated by Pearson's or Spearman's test as appropriate. The statistical analysis was performed using MedCalc version 9.3 (MedCalc Software, Mariakerke, Belgium). P values of less than 0.05 were regarded as statistically significant.
RESULTS
The characteristics of the study cohort are presented in Table 1. Mean age of the patients (11 females and 20 males [ratio, 1:2]) was 62.4±10.2 years. Mean serum creatinine was 1.66±0.82 mg/dL with a mean GFR of 49.3±17.5 mL/min/1.73 m2 (range, 13.1 to 78.3). The mean urinary NGAL level of the CKD patients was significantly higher than that measured in healthy controls (96.0 [2.7 to 975.2] ng/mL vs. 18.8 [1.3 to 81.9] ng/mL, P=0.02) and GFR was lower than those in healthy controls (49.3 [13.1 to 78.3] mL/min/1.73 m2 vs. 85.6 [72 to 106.7] mL/min/1.73 m2, P<0.0001) (Fig. 1).
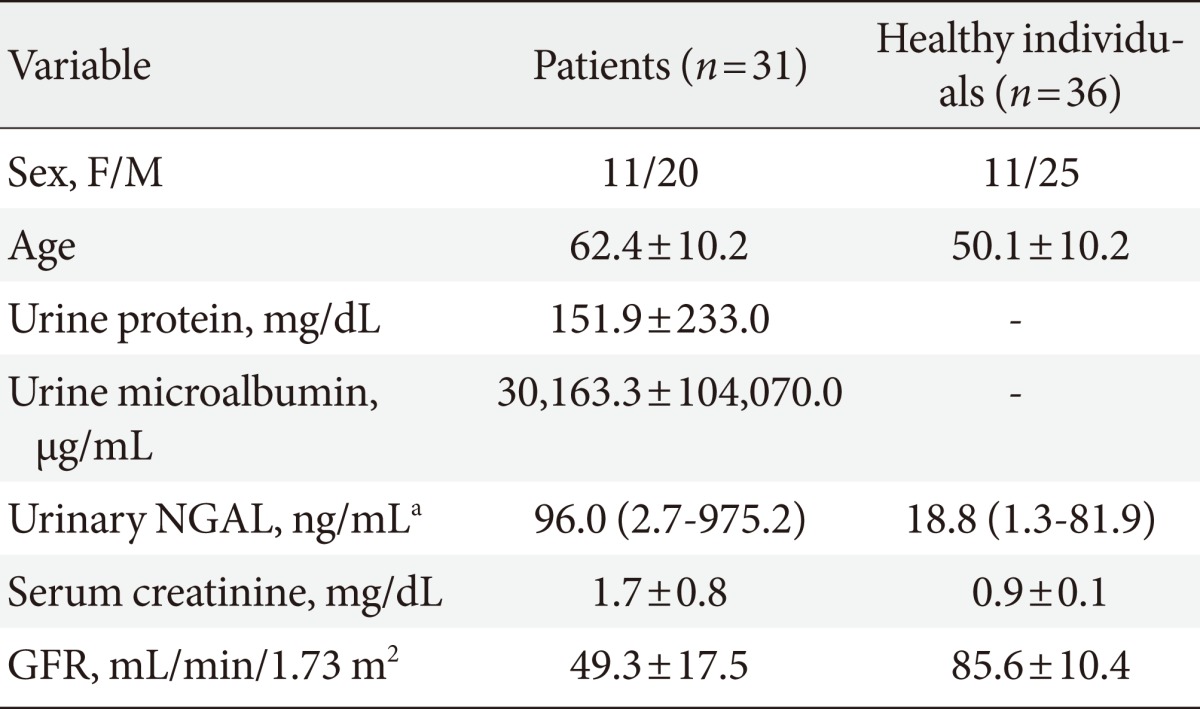
Demographic data of 31 patients and 36 healthy individuals

Urinary neutrophil gelatinase-associated lipocalin (NGAL) levels and glomerular filtration rate (GFR) in patients and healthy populations. (A) NGAL levels: 18.8 (1.3 to 81.9) ng/mL vs. 96.0 (2.7 to 975.2) ng/mL (P=0.02). (B) GFR: 49.3 (13.1 to 78.3) mL/min/1.73 m2 vs. 85.6 (72 to 106.7) mL/min/1.73 m2 (P<0.0001). CKD, chronic kidney disease.
Correlation between GFR and urinary NGAL levels
The correlation analyses between GFR and urinary NGAL levels in CKD patients are presented in Fig. 2. The urinary NGAL level showed a significant inverse correlation with GFR in CKD patients (r=-0.5634, P<0.0001).
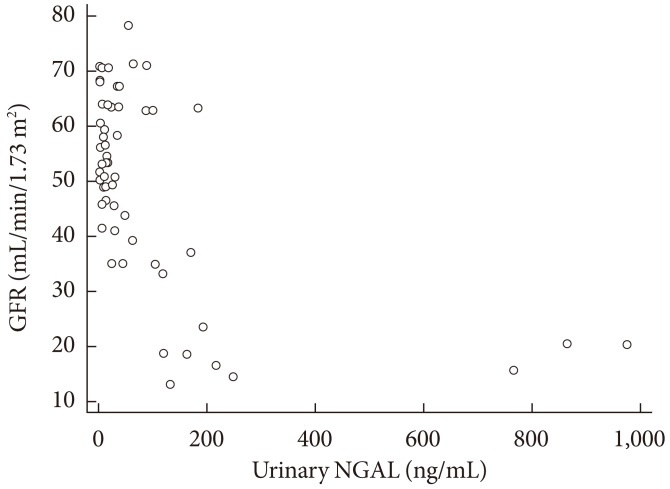
Correlation analysis between glomerular filtration rate (GFR) and urinary neutrophil gelatinase-associated lipocalin (NGAL) in chronic kidney disease patients (r=-0.5634, P<0.0001).
Correlation between urinary protein level and urinary NGAL and GFR
The correlation analyses between urinary protein and urinary NGAL levels in CKD patients are presented in Fig. 3. The correlation between urinary protein and urinary NGAL levels and GFR in patients were as follows: urine protein and urinary NGAL (r=0.3009, P=0.0256), urine protein and GFR (r=-0.6245, P<0.0001), urine albumin and urinary NGAL (r=0.1794, P=0.2275), and urine albumin and GFR (r=-0.5190, P=0.0002). The urinary NGAL level was significantly correlated with the amount of urinary protein excretion in CKD patients. GFR, like urinary NGAL, also showed a strong correlation with the extent of urinary protein, including albumin, but the level of correlation with GFR was even greater in CKD patients in our study. In addition, only GFR showed a negative correlation with UACR (r=0.5497, P=0.0001). Urinary NGAL, however, was not correlated with UACR.
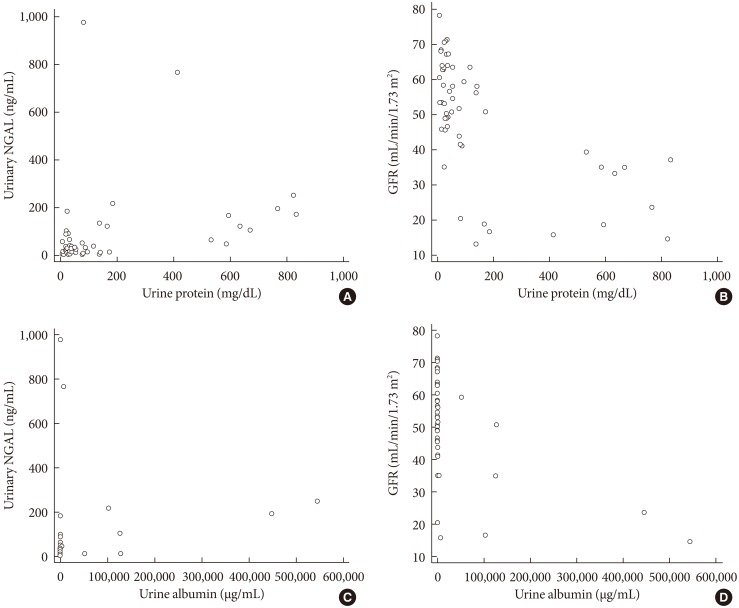
Correlation analyses for urine protein and urinary neutrophil gelatinase-associated lipocalin (NGAL) levels and glomerular filtration rate (GFR) in chronic kidney disease patients. Correlations were analyzed between urinary protein level and urinary NGAL level (A) (r=0.3009, P=0.0256), urine protein and GFR (B) (r=-0.6245, P<0.0001), urine albumin and urinary NGAL (C) (r=0.1794, P=0.2275), and urine albumin and GFR (D) (r=-0.5190, P=0.0002).
Correlation between the age, sex, and GFR and urinary NGAL in the control group
In the analyses with the control subjects, no significant correlation was observed between urinary NGAL levels and other variables (Fig. 4).
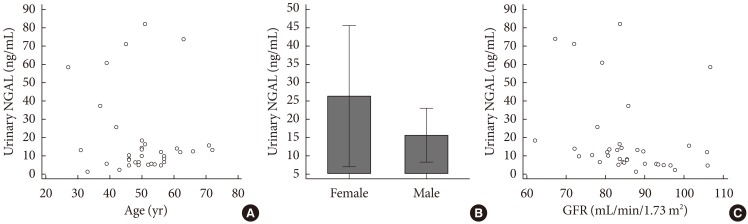
Correlation between age (A) (r=-0.1488, P=0.3866), sex (B) (P=0.1823), and glomerular filtration rate (GFR) (C) (r=-0.2621, P=0.1226) and urinary neutrophil gelatinase-associated lipocalin (NGAL) in healthy populations.
DISCUSSION
Many clinical studies have demonstrated the utility of NGAL as a specific, sensitive, and early predictor of AKI [3-7]. In CKD, there are also many reports suggesting that NGAL is also a novel, independent marker of disease progression that provides a good reflection of the severity of renal disease. A variety of clinical settings have been examined, including cardiac surgery, contrast administration, septic shock, intensive care units, the emergency department, and even renal transplantation [7,14-22]. In one study of CKD patients secondary to renal dysplasia, obstructive uropathy, and glomerular and cystic diseases, plasma NGAL concentrations were inversely associated with GFR [8]. Another study in subjects with CKD (due to chronic glomerulonephritis) showed that mean urinary NGAL concentrations were higher in CKD patients (378.28±111.13 µg/L vs. 7.38±3.26 µg/L in controls, P=0.01). Furthermore, urinary NGAL concentrations were significantly correlated with GFR (r=-0.528, P=0.04) and proteinuria (r=0.294, P=0.01) [10]. In a study of 80 non-diabetic patients with CKD stages 2 to 4, 80 kidney transplant recipients, and 32 healthy control subjects, the investigators found that serum NGAL values were significantly higher in kidney allograft recipients and patients with CKD compared with healthy controls. NGAL rose gradually, reaching the highest value in advanced CKD [22]. In addition, Bolignano et al. [12] measured NGAL in a cohort of patients affected by non-advanced CKD with stable renal function. A strict, independent, and inverse correlation with GFR was described for both serum and urinary NGAL, suggesting that urinary and serum NGAL predicted CKD progression independent of age and GFR. Recently, several reports showed conflicting results concerning the correlation between increased tubular makers, including urinary NGAL, and disease progression in diabetic patients. Fu et al. [23] measured several markers of renal damage, especially tubular markers, including urinary NGAL. In one study including 101 type 2 diabetic patients, they categorized patients into three groups according to their UACR and compared tubular markers with renal indices, such as UACR and GFR. Urinary NGAL showed a positive correlation with UACR and a negative correlation with GFR [24]. In our study, urinary NGAL also showed a negative correlation with GFR. However, there was no statistically significant correlation between urinary NGAL and UACR. In the study of Fu et al., they categorized patients into two groups according to GFR and excluded the lower GFR group, and they observed that higher urinary tubular damage markers were found in type 2 diabetic patients with glomerular hyperfiltration (GHF) than in the normal GFR and control groups. GHF is known to play a crucial role in the progression of diabetic nephropathy and has been regarded as a risk factor for the development of microalbuminuria. However, in contrast to that previous study, the present study included patients with diabetic CKD and overt albuminuria, and their baseline GFR was 49.3 mL/min/1.73 m2. GHF has been regarded as a risk factor for the initiation and development of microalbuminuria. This explains why our study did not show an effect of GHF when evaluating tubular damage markers, such as urinary NGAL, even though NGAL was negatively correlated with GFR. However, few studies have reported that tubular damage markers are not predictive of the decline in GFR in diabetic patients. Nielsen et al. [25] reported a lack of an independent correlation between these biomarkers and GFR in diabetic patients. Their study included type 1 diabetic patients with overt nephropathy, but our study included type 2 diabetic patients and showed a negative correlation between urinary NGAL and GFR without adjustment.
The results of our study showed that urinary NGAL levels were significantly elevated in diabetic CKD patients compared to the normal control group. These results were consistent with previous reports indicating increased serum and urinary NGAL levels in CKD patients with decreased GFR [8,10-12]. A significant inverse correlation was also observed between urinary NGAL level and GFR in CKD patients, similar to what has previously been described elsewhere [10-12]. We also analyzed for a correlation between NGAL and the amount of urinary excretion of protein, including albumin. Previous reports have shown a direct correlation between proteinuria and urinary NGAL level [10,11,26]. Consistent with these reports, we observed a significant correlation between urinary NGAL levels and the level of urinary protein excretion, excluding albumin, in CKD patients. These results suggest that NGAL could be a marker of renal function in patients with diabetic CKD.
We also analyzed the correlation between GFR and the amount of urinary protein excretion and observed a significant correlation with the amount of urinary protein excretion, including both albumin and protein, and the levels of correlation were higher than for urinary NGAL. Fig. 1 shows that GFR was significantly lower in CKD patients than in healthy controls, and the level of difference was higher than for urinary NGAL. Therefore, our study did not demonstrate that the rate of deterioration in renal function in diabetic CKD patients is more accurately associated with the degree of renal tubulointerstitial damage than with the severity of glomerular lesions. Though there are many studies suggesting that creatinine and GFR based on creatinine show low accuracy for measuring of renal function, GFR is still thought to be a reliable marker for estimating renal function in our study [27,28].
Our study has some potential limitations. The small population in our study, selection of the control group, ethnic differences, and differences in methods for evaluating urinary NGAL may have influenced the results. Additionally, the pathogenesis of diabetic kidney disease is complex and multifactorial. The duration of diabetes among the patients varied and hemodynamic changes could occur in the glomeruli causing glomerular hyperfiltration and altered vascular endothelial tone, which are related to GFR and urinary NGAL levels [29]. Medications were not evaluated in this study. Our study only included diabetic CKD patients and healthy individuals. In addition, urinary NGAL and the serum creatinine were measured only once in a small population, and we could not rule out intra-patient variability or analyze for correlation between urinary NGAL and disease progression. However, our results were similar to results of previous reports that have demonstrated a strong correlation between GFR and urinary NGAL and that urinary NGAL is not influenced by age and gender.
In conclusion, we conclude that urinary NGAL is a reliable marker of renal function in diabetic CKD patients. Despite a good correlation between GFR and the amount of urinary protein excretion and urinary NGAL, urinary NGAL provided no additional information regarding renal function compared with GFR as a routine laboratory test for diabetic CKD patients. Future studies in different clinical settings with larger numbers of patients and healthy individuals are necessary to clarify the effectiveness of urinary NGAL in determining renal function and disease progression.
ACKNOWLEDGMENTS
This work was supported by the Dong-A University research fund.
Notes
No potential conflict of interest relevant to this article was reported.