- Current
- Browse
- Collections
-
For contributors
- For Authors
- Instructions to authors
- Article processing charge
- e-submission
- For Reviewers
- Instructions for reviewers
- How to become a reviewer
- Best reviewers
- For Readers
- Readership
- Subscription
- Permission guidelines
- About
- Editorial policy
Articles
- Page Path
- HOME > Diabetes Metab J > Volume 48(2); 2024 > Article
-
Original ArticleDrug/Regimen Two-Year Therapeutic Efficacy and Safety of Initial Triple Combination of Metformin, Sitagliptin, and Empagliflozin in Drug-Naïve Type 2 Diabetes Mellitus Patients
-
Young-Hwan Park
 , Minji Sohn, So Yeon Lee, Soo Lim
, Minji Sohn, So Yeon Lee, Soo Lim -
Diabetes & Metabolism Journal 2024;48(2):253-264.
DOI: https://doi.org/10.4093/dmj.2023.0128
Published online: January 26, 2024
- 1,778 Views
- 284 Download
Department of Internal Medicine, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea
-
Corresponding author: Soo Lim Department of Internal Medicine, Seoul National University Bundang Hospital, Seoul National University College of Medicine, 82 Gumi-ro 173beon-gil, Bundang-gu, Seongnam 13620, Korea E-mail: limsoo@snu.ac.kr
Copyright © 2024 Korean Diabetes Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Background
- We investigated the long-term efficacy and safety of initial triple therapy using metformin, a dipeptidyl peptidase-4 inhibitor, and a sodium-glucose cotransporter-2 inhibitor, in patients with type 2 diabetes mellitus.
-
Methods
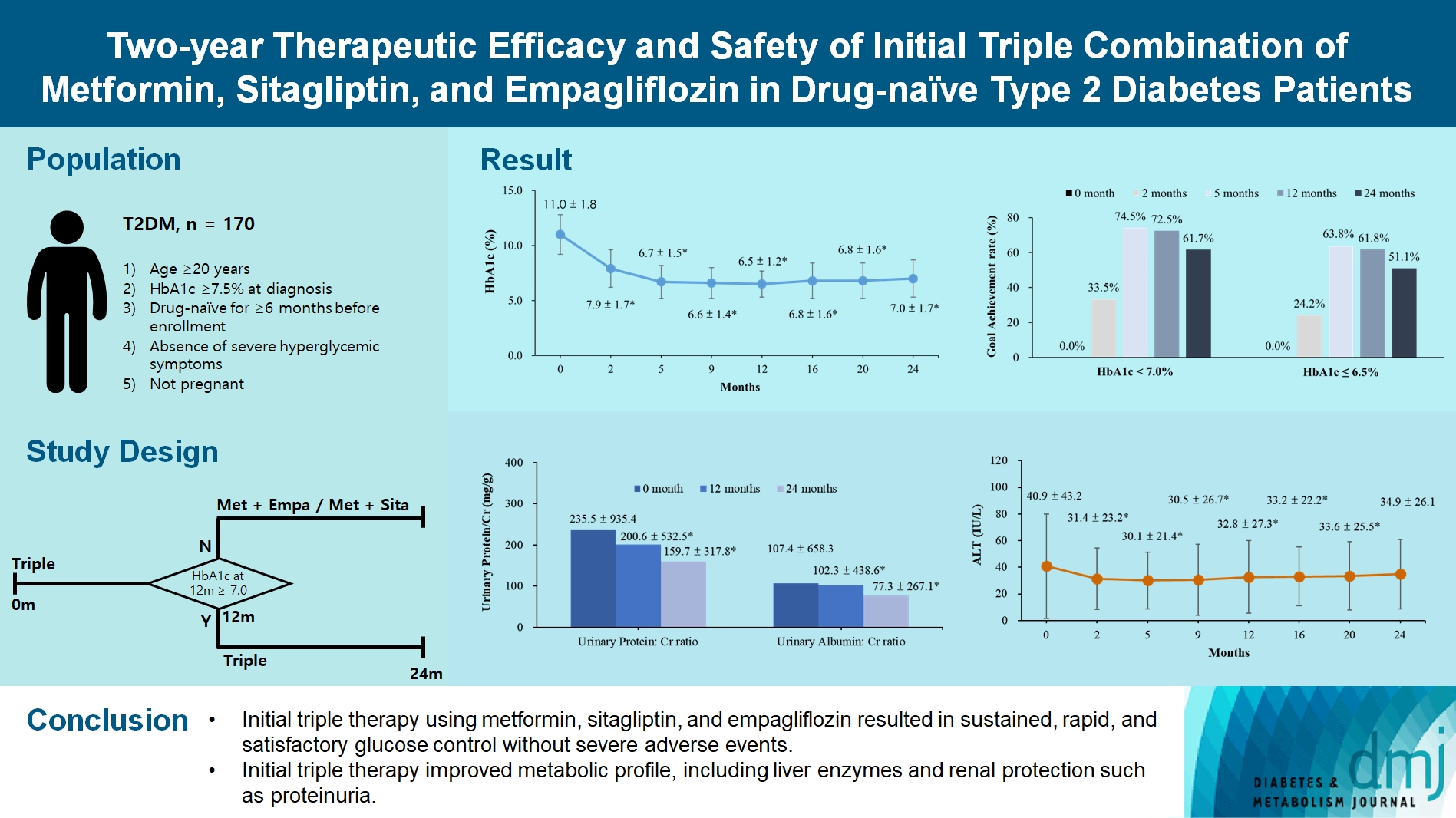
- We enrolled 170 drug-naïve patients with glycosylated hemoglobin (HbA1c) level >7.5% who had started triple therapy (metformin, sitagliptin, and empagliflozin). Glycemic, metabolic, and urinary parameters were measured for 24 months.
-
Results
- After 24 months, HbA1c level decreased significantly from 11.0%±1.8% to 7.0%±1.7%. At 12 and 24 months, the rates of achievement of the glycemic target goal (HbA1c <7.0%) were 72.5% and 61.7%, respectively, and homeostasis model assessment of β-cell function and insulin resistance indices improved. Whole-body fat percentage decreased by 1.08%, and whole-body muscle percentage increased by 0.97% after 24 months. Fatty liver indices and albuminuria improved significantly. The concentration of ketone bodies was elevated at the baseline but decreased after 24 months. There were no serious adverse events, including ketoacidosis.
-
Conclusion
- Initial triple combination therapy with metformin, sitagliptin, and empagliflozin led to achievement of the glycemic target goal, which was maintained for 24 months without severe hypoglycemia but with improved metabolic function and albuminuria. This combination therapy may be a good strategy for drug-naïve patients with type 2 diabetes mellitus.
Highlights
- Landmark clinical trials in the management of type 2 diabetes mellitus (T2DM) have reported that intensive glycemic control reduces the risk of microvascular complications [1,2]. Other studies have reported that intensive glycemic control in the early period of diabetes leads to a significantly lower incidence of macrovascular complications [2,3]. Therefore, achievement of optimal glycemic control is an important aim in the management of T2DM. However, the current data indicate poor attainment of glycemic targets in clinical practice [4]. The traditional sequential treatment paradigm for T2DM, which comprises stepwise addition of antidiabetic agents to initial metformin therapy in response to increased glycosylated hemoglobin (HbA1c) level, is probably the major reason for delays in reaching the glycemic goal and the development of complications [5,6].
- More active therapy that uses a combination of antidiabetic agents with complementary mechanisms of action, and that targets multiple physiological defects, is an alternative approach to T2DM treatment. The initial dual combination therapy in the early stages of T2DM has been reported to hasten the achievement of glycemic goals, to have a more durable effect, and to preserve β-cell function better than the sequential stepwise approach [7-9]. Compared with metformin monotherapy, initial combination therapy with dipeptidyl peptidase-4 (DPP4) inhibitors and metformin induced greater reductions in HbA1c and fasting glucose levels [10]. Combination therapy using metformin and a DPP4 inhibitor (vildagliptin) has been shown to have long-term benefits in drug-naïve patients with T2DM [11].
- Given these findings, international consensus has recognized the need for combination therapy for glucose-lowering in patients with a high HbA1c level [12]. International and Korean clinical guidelines recommend combination therapy when the HbA1c level is >7.5% in the initial assessment [13,14]. However, there are limited data on whether the benefit-risk profile of initial combination therapy is superior to that of the traditional sequential treatment, and for which patients’ initial combination therapy is appropriate.
- Few studies have focused on initial triple combination therapy. Abdul-Ghani et al. [15] reported that combination therapy comprising metformin, pioglitazone (a thiazolidinedione), and exenatide in patients with newly diagnosed T2DM was more effective and resulted in fewer hypoglycemic events than sequential add-on therapy comprising metformin, sulfonylurea, and basal insulin. Our group has reported that initial triple combination therapy comprising metformin, sitagliptin, and lobeglitazone (a thiazolidinedione) resulted in a higher percentage of patients who achieved their target goal over conventional therapy and had fewer adverse events [16]. However, concern has arisen because thiazolidinedione and some DPP4 inhibitors may increase the risk of heart failure [17].
- Sodium-glucose cotransporter-2 (SGLT2) inhibitors, a novel class of antidiabetic medication, were introduced in 2010. A randomized controlled trial reported that combination therapy comprising sitagliptin and ertugliflozin (an SGLT2 inhibitor) reduced HbA1c level, body weight, and blood pressure more than the individual agents [18]. In our pilot study, the initial combination of metformin, sitagliptin, and empagliflozin significantly reduced glucose level and did not induce adverse events in drug-naïve Korean patients with T2DM and with an HbA1c level >9% [19]. However, there are limited long-term different using different drug classes in drug-naïve patients [20]. Because of the complementary mechanism of action, investigation of initial triple combination therapy with these new drug classes would be informative. The aim of the present study was to evaluate the efficacy and safety of an initial triple regimen with metformin, sitagliptin, and empagliflozin in patients with T2DM.
INTRODUCTION
- Study design
- This study was a prospective, observational study and was approved by an independent ethics committee/Institutional Review Board (B-2008/630-104). Written informed consent was acquired from the participants before data collection. Study participants were selected from drug-naïve patients with newonset T2DM who visited the diabetes clinic at Seoul National University Bundang Hospital from 2017 to 2021 and who met the following criteria: (1) age ≥20 years; (2) HbA1c ≥7.5% at diagnosis; (3) drug-naïve for ≥6 months before enrollment; (4) absence of severe hyperglycemic symptoms; and (5) not pregnant. Patients with severe hyperglycemic symptoms who required insulin therapy were excluded.
- Participants started the initial combination therapy of metformin 1,000 mg/day, sitagliptin 100 mg/day, and empagliflozin 10 mg/day at the baseline and were followed for 2 years. Patients were hospitalized for close observation if they consented. The patients visited the clinic at 2, 5, 9, and 12 months in the first year and at 16, 20, and 24 months in the second year. Anthropometric and biochemical variables were measured at every visit.
- For patients with an HbA1c level exceeding 8.0% in the initial 6 months, the metformin dosage could be augmented by 25% to 50%, and the empagliflozin dosage could be escalated by 25 mg, subject to the physician’s discretion. The dose of empagliflozin was guided to be maintained at 10 mg throughout the study period, because previous studies reported that no significant difference in the glucose-lowering efficacy of empagliflozin between 10 and 25 mg [21,22]. If the HbA1c level did not achieve the desired glycemic target (<7.0%), the initial triple therapy was sustained. For those patients who met their glycemic goals at the 12-month visit, the medication regimen was either reduced to two agents (reduced group) or remained unchanged (maintained group) based on the physician’s judgment. In instances where patients experienced a temporary rise in glucose levels for any reason during the study, short-term insulin administration was recommended for safety considerations. Upon verification of achieving the glycemic target at 12 months, either empagliflozin or sitagliptin was discontinued, with the decision based on the patient’s body weight and the physician’s assessment.
- Anthropometric and biochemical parameters
- At every visit, the efficacy indicators (HbA1c, fasting plasma glucose, postload 2-hour glucose, and fasting insulin levels), body composition (body weight, muscle mass, and fat mass), ketone body levels (β-hydroxybutyrate and acetoacetate), proteinuria (urinary protein/creatinine and urinary albumin/creatinine ratios), organ function, and uric acid level were measured using standard methods.
- Height and body weight were measured using standard methods with the participant in light clothing. Body mass index (BMI) was calculated by dividing the participant’s weight (kg) by height squared (m2). Waist circumference (WC) was measured at the umbilical level. Systolic and diastolic blood pressure were measured with the participant in a seated position using an electronic blood pressure meter (UA-1020 device, A&D, Tokyo, Japan). Blood pressure was measured twice, 5 minutes apart, and the mean value was used in the analysis.
- Plasma glucose concentration was measured using the glucose oxidase method (747 Clinical Chemistry Analyzer, Hitachi, Tokyo, Japan). HbA1c level was measured using a Variant II Turbo HPLC Analyzer (Bio-Rad, Hercules, CA, USA) in a National Glycohemoglobin Standardization Program level II-certified laboratory. Fasting plasma C-peptide and insulin levels were measured by radioimmunoassay (Linco, St. Louis, MO, USA).
- Serum aspartate aminotransferase (AST), alanine aminotransferase (ALT), and creatinine levels were measured using an Architect Ci8200 analyzer (Abbott Laboratories, Abbott Park, IL, USA). The estimated glomerular filtration rate (eGFR) was calculated using the creatinine-based Chronic Kidney Disease Epidemiology Collaboration equation (CKD-EPI). Serum free fatty acid, total cholesterol, triglyceride, high-density lipoprotein cholesterol (HDL-C), and low-density lipoprotein cholesterol (LDL-C) levels were measured using a 747 Clinical Chemistry Analyzer (Hitachi). Urinary albumin concentration was measured using turbidimetry (502X, A&T, Tokyo, Japan), and urinary creatinine was measured using the Jaffe method (Hitachi 7170, Hitachi). The ratio of urinary protein or albumin to creatinine concentration (mg/g) was used to identify proteinuria and albuminuria, respectively. To estimate pancreatic β-cell function and insulin resistance, the homeostasis model assessment of insulin resistance (HOMA-IR) and β-cell function (HOMA-β) indices were calculated [23].
- The nonalcoholic fatty liver disease (NAFLD) liver fat score was calculated using the following equation: 1.18×metabolic syndrome+0.45×diabetes (2, if yes; 0, if no)+0.15×fasting insulin (μIU/L)+0.04×AST (IU/L)–0.94×(AST/ALT)–2.89 [24]. Metabolic syndrome was defined according to National Cholesterol Education Program Adult Treatment Panel III guideline [25] using ethnic-specific cutoff values for WC [26].
- Safety parameters were assessed including the adverse events of gastrointestinal discomfort, urinary tract infection, genital infection, ketoacidosis, and hypoglycemia. Hypoglycemic events were recorded based on the patients’ hypoglycemic symptoms and self-monitored plasma glucose level <70 mg/dL (3.9 mmol/L).
- Statistical analysis
- All patients who were enrolled in the analysis completed at least one follow-up. Patients who were lost to follow-up were considered as censored data. All available data were included in the analysis. The summary statistics are shown as mean with standard deviation. All indicators were compared between the baseline and after treatment using the paired t-test. Data with wide variation were analyzed after log transformation and included ketone body levels, urinary protein/creatinine ratio, and urinary albumin/creatinine ratio. Subgroup analysis was performed in patients grouped according to the change in drug regimen after 12 months and at the end of the observation period. The changes in outcomes over time within each group were analyzed using analysis of variance (ANOVA) and the post hoc Duncan test. All data analysis was performed using R software version 4.1.3 (The R Foundation for Statistical Computing, Vienna, Austria).
METHODS
- Baseline characteristics of study participants
- The baseline characteristics of the study participants are shown in Table 1. The 170 study participants (age 51.0±13.1 years) included 67.6% men (n=115, age 49.2±12.7 years) and 32.4% women (n=55, age 54.6±13.2 years). The baseline HbA1c levels did not differ between men and women (11.0%±1.9% and 11.1%±1.6%, respectively). The baseline total ketone body levels were elevated across the broad range of 25.0 to 9,150.0 μmol/L. The total ketone body levels were higher in patients with baseline HbA1c >10.0% (n=78) than in those with baseline HbA1c ≤10.0% (n=34) (757.9±1,510.0 μmol/L vs. 244.7± 317.1 μmol/L, P<0.05). Of the 170 patients in the study, there were 50 (29.4%) patients with hypertension, 48 (28.2%) patients with dyslipidemia, three (1.8%) patients with coronary artery disease, and six (3.5%) patients with stroke. A total of 82 (48.2%) patients hospitalized in the beginning and 112 (65.9%) patients finished the last visit.
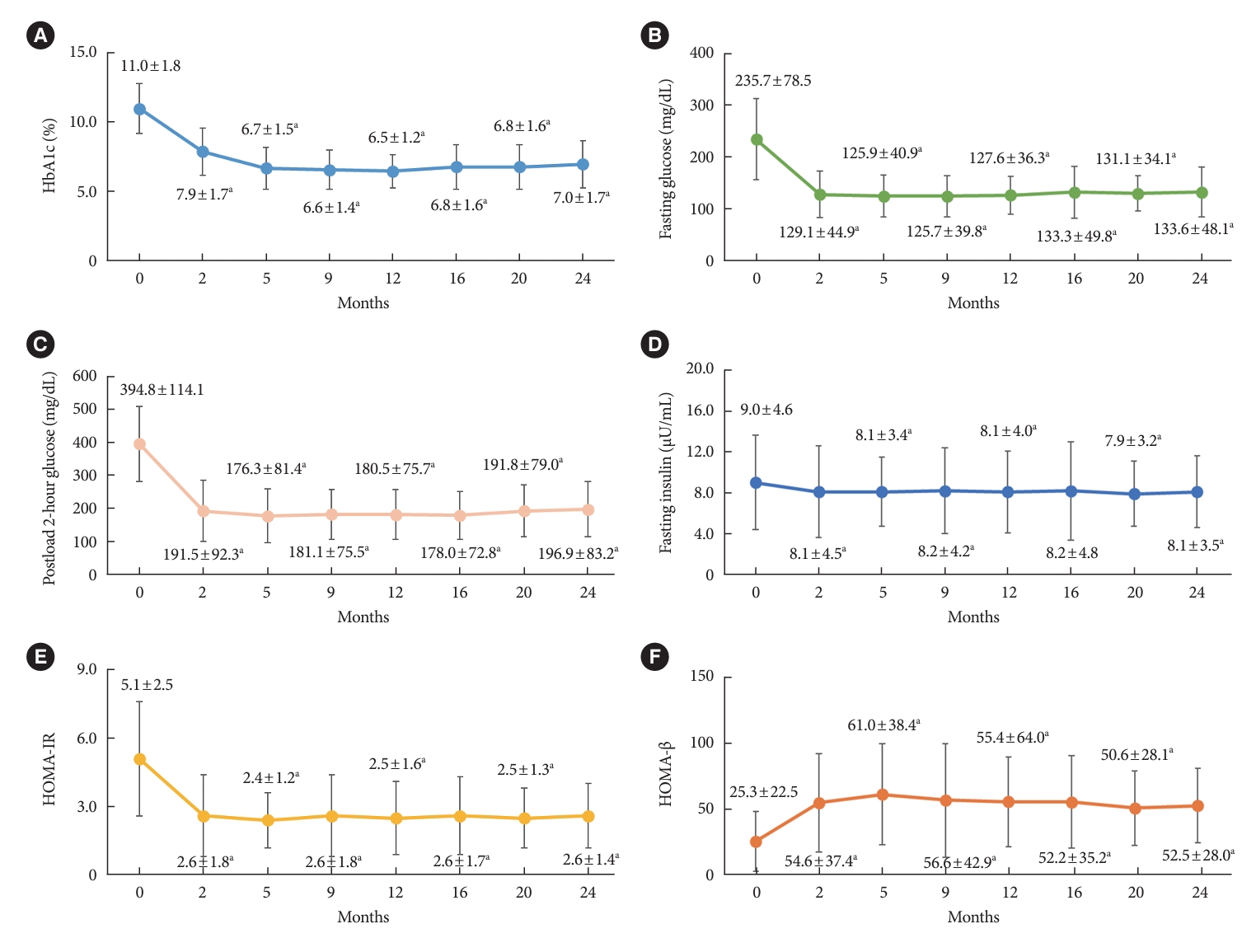
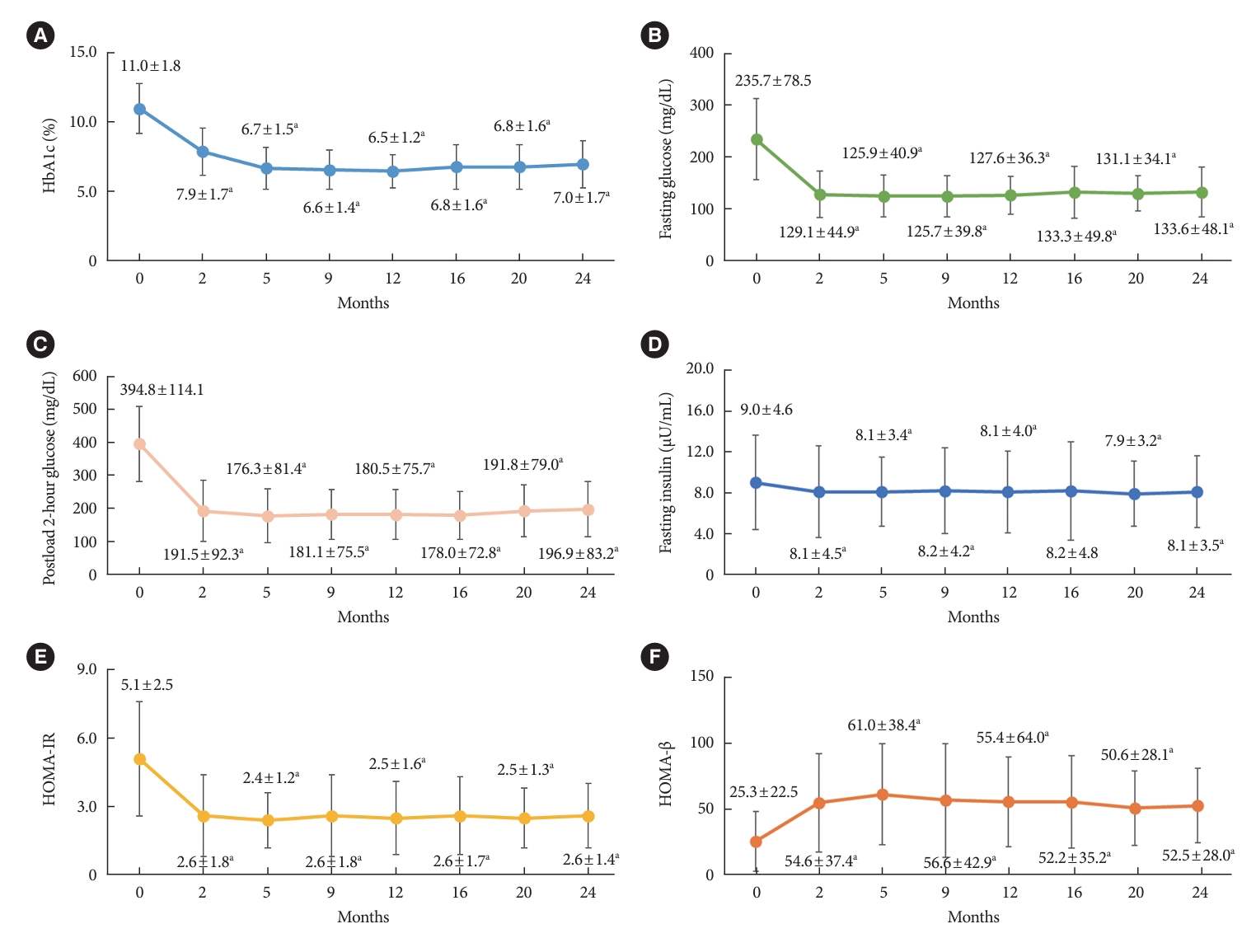
- Changes in parameters related to glycemic regulation The HbA1c levels at the baseline and at 2, 5, 9, 12, 16, 20, and 24 months are shown in Fig. 1A. Two patients received insulin therapy due to an increase in glucose concentrations temporarily. The high baseline HbA1c level decreased significantly from 11.0%±1.8% to 7.9%±1.7% (P<0.05) at 2 months, and to 6.7%±1.5% at 5 months, and it remained lower at 7.0%±1.7% at 24 months (P<0.05). The rates of achievement of the HbA1c target <7.0% were 72.5% at 12 months and 61.7% at 24 months (Supplementary Fig. 1). For the stricter HbA1c target <6.5%, the rates of target goal achievement were 61.8% at 12 months and 51.1% at 24 months.
- Similarly, both the fasting plasma and postload 2-hour glucose concentrations decreased significantly (P<0.05). The fasting plasma glucose concentration decreased by 101.4 mg/dL, from 235.7±78.5 mg/dL at the baseline to 133.6±48.1 mg/dL at 24 months (Fig. 1B). The postload 2-hour glucose concentration also decreased by 181.8 mg/dL, from 394.8±114.1 mg/dL at the baseline to 196.9±83.2 mg/dL at 24 months (Fig. 1C).
- Changes in insulin resistance and β-cell function
- The initial triple therapy decreased the fasting insulin level significantly from 9.0±4.6 μIU/mL at the baseline to 8.1±4.5 μIU/mL at 2 months and remained stable thereafter (Fig. 1D). The HOMA-IR indices also decreased from 2 months and were maintained to the end of the study (Fig. 1E). The HOMA-β indices increased sequentially until 5 months and remained stable at the level of 56.6%±42.9% from 9 months (Fig. 1F). These changes indicate improved β-cell function.
- Changes in body weight, body mass index, and body composition
- Body weight and BMI did not change significantly (Fig. 2A and B), but body composition changed significantly after the triple therapy (Fig. 2C and D). Whole-body fat percentage decreased significantly by 1.08% from 30.0%±8.1% at the baseline to 27.6%±7.6% at 24 months (Fig. 2D). Whole-body muscle percentage showed the opposite trend and increased significantly by 0.97% from 66.1%±7.7% at the baseline to 68.3%± 7.2% at 24 months.
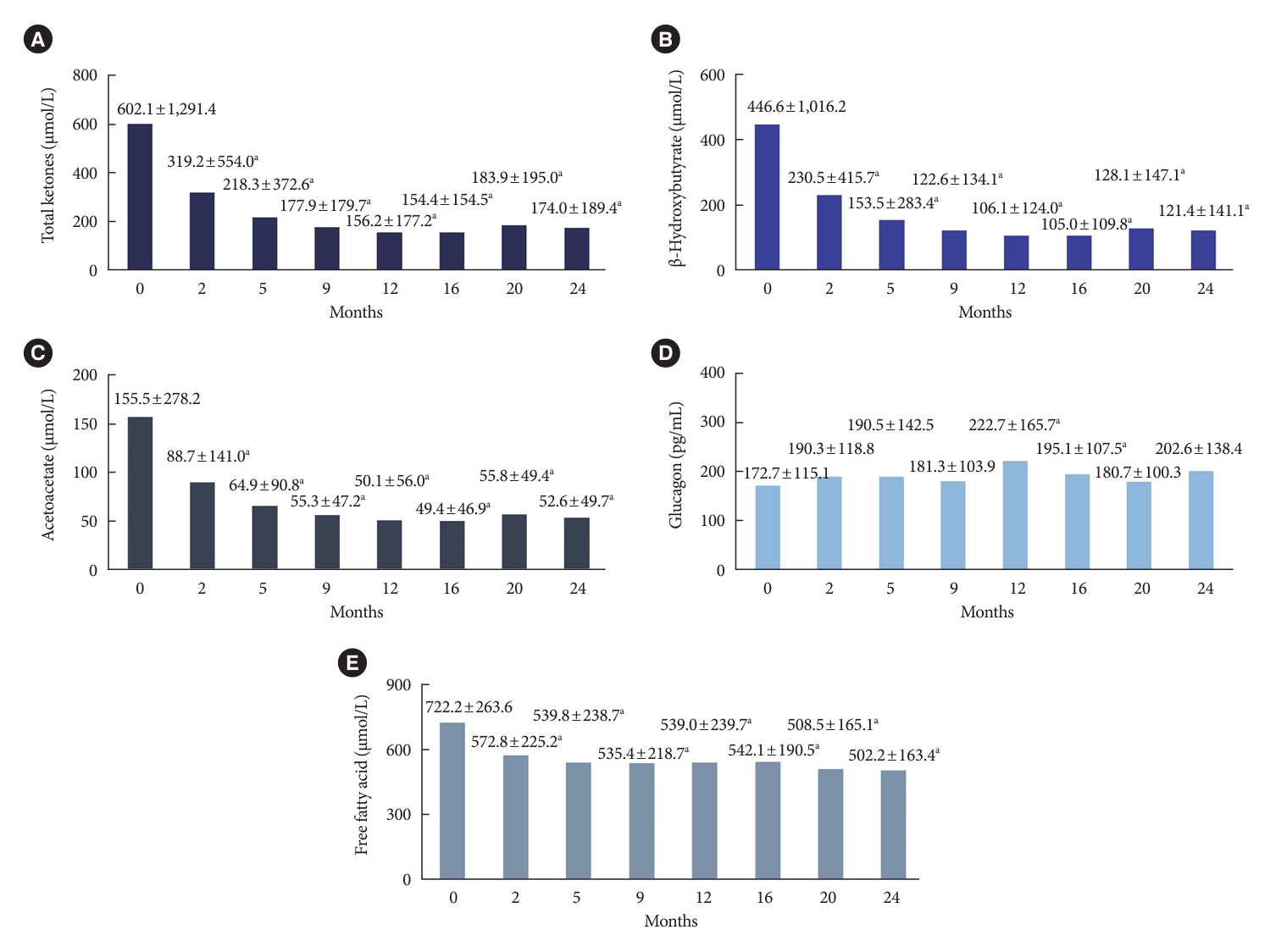
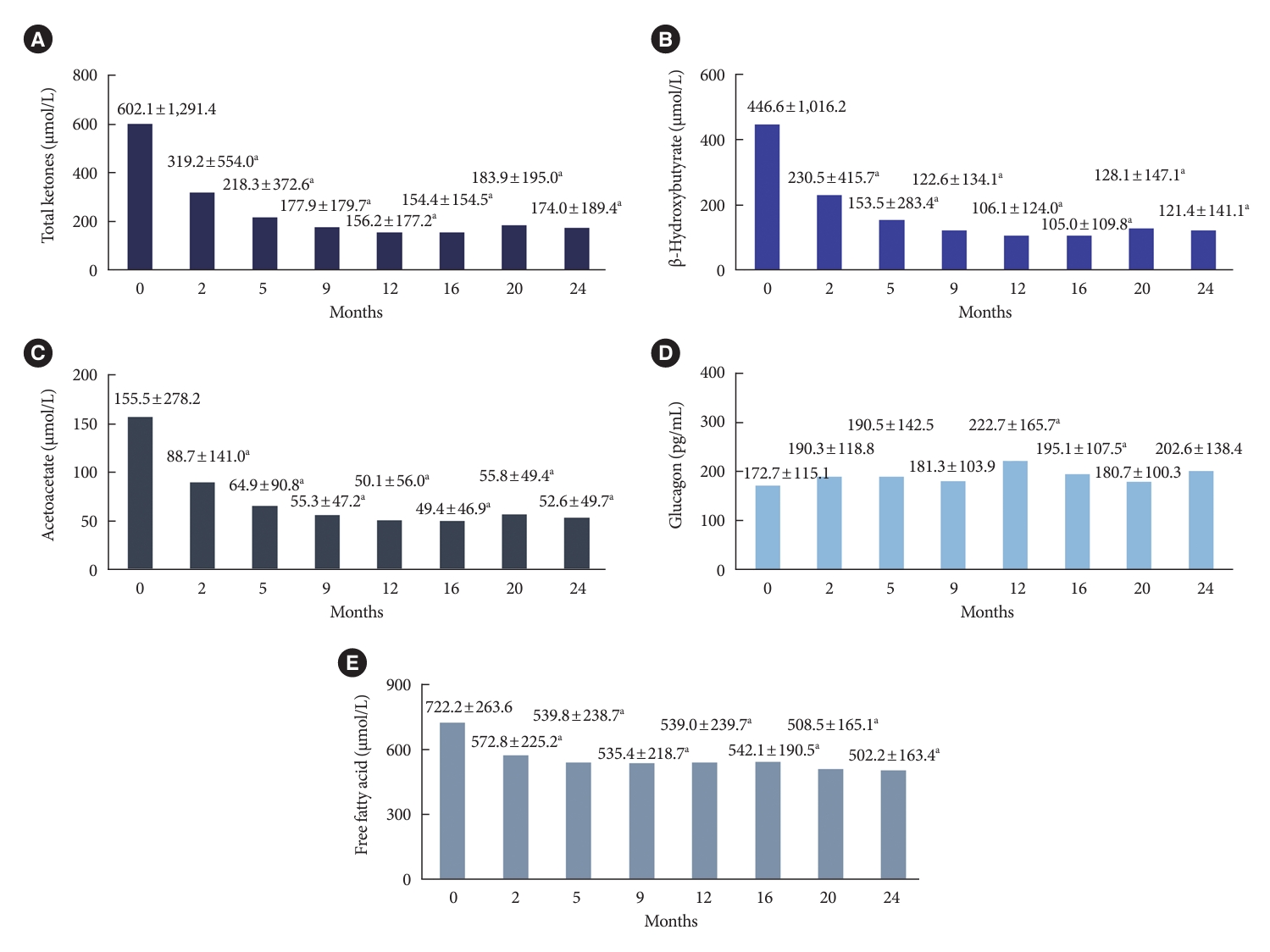
- Changes in ketone body and glucagon levels
- The initial triple therapy with metformin, sitagliptin, and empagliflozin decreased ketone body levels (Fig. 3A-C). The total ketone body concentration was elevated at the baseline and decreased significantly from 602.1±1,291.4 μmol/L to 174.0± 189.4 μmol/L at 24 months (Fig. 3A). Similarly, the levels of β-hydroxybutyrate and acetoacetate also decreased significantly after 24 months (Fig. 3B and C).
- The ketone body concentration showed different trends according to the baseline HbA1c level. In patients with baseline HbA1c >10.0%, the total concentration of ketone bodies decreased significantly from 757.9±1,510.0 μmol/L at the baseline to 184.6±213.2 μmol/L at 24 months (Supplementary Fig. 2). The total concentration of ketone bodies in patients with HbA1c ≤10.0% (n=34) also decreased, but only slightly and not significantly, from 244.7±317.1 μmol/L at the baseline to 153.1±132.2 μmol/L at 24 months (Supplementary Fig. 2D).
- We analyzed the data further according to the median ketone concentration: ≥200 μmol/L and <200 μmol/L (Supplementary Fig. 3). The ketone body concentration in patients with high initial total ketone body level (≥200 μmol/L) decreased substantially by 847 μmol/L, from 1,078±1,683 μmol/L at the baseline to 231±247 μmol/L at 24 months (Supplementary Fig. 3A). However, the ketone body concentration did not change significantly in those with an initial baseline level <200 μmol/L (Supplementary Fig. 3D). Glucagon concentration remained stable except for slight increases at 12 and 16 months (Fig. 3D).
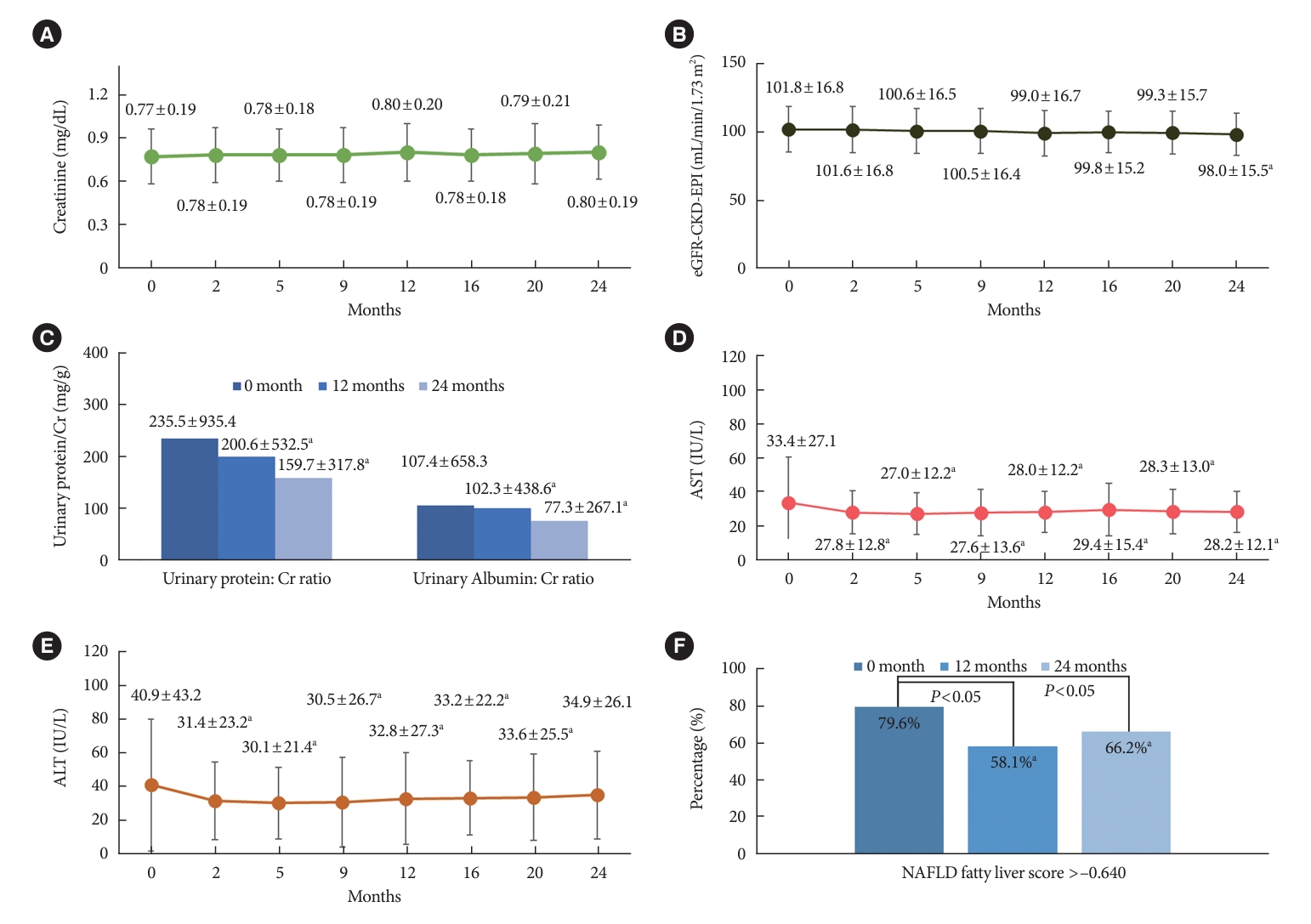
- Changes in renal function
- The changes in renal function indicators creatinine concentrations, eGFR-CKD-EPI, and urinary protein/creatinine and albumin/creatinine ratios are shown in Fig. 4A-C. The eGFR-CKD-EPI decreased slightly but significantly by 2.3 mL/min/1.73 m2 (Fig. 4B). It is noteworthy that both the urinary protein/creatinine and albumin/creatinine ratios decreased significantly from the baseline to 24 months (Fig. 4C).
- Changes in liver function
- The AST level decreased from 33.4±27.1 IU/L at the baseline to 27.8±12.8 IU/L at 2 months and was maintained for 24 months (Fig. 4D). The ALT level decreased significantly until 16 months; at 24 months, the decrease in ALT level was nearly maintained, but the level did not differ significantly from the baseline value (Fig. 4E). The NAFLD fatty liver score decreased significantly after 24 months from 79.3% at the baseline to 58.1% at 12 months and 66.2% at 24 months (P<0.05 for each comparison) (Fig. 4F).
- Safety
- In this study, 27 adverse events were reported in 170 subjects (16%). The most frequent adverse events were urinary tract genital infection and hepatic enzyme elevation (n=4 each) (Supplementary Table 1). Three patients experienced a hypoglycemic event in this study. No patients experienced severe hypoglycemia or nocturnal hypoglycemia. No other serious adverse events were observed during the study period.
- Subgroup analysis
- A total of 112 patients of the 170 were followed for 24 months; 37 received metformin and empagliflozin, 26 received metformin and sitagliptin, and 49 continued the triple therapy. The baseline characteristics did not differ between these three groups, except for body weight and BMI, which were significantly lower in the metformin and sitagliptin group than in the other groups (Supplementary Table 2).
- Changes in the clinical and biochemical parameters in these three groups are shown in Supplementary Fig. 4. In all groups, the reduced HbA1c levels were maintained for 24 months (Supplementary Fig. 4A). Body weight increased after empagliflozin discontinuation and led to greater changes in body weight in the metformin and sitagliptin group than in the other two groups (Supplementary Fig. 4B). The eGFR-CKD-EPI levels were maintained in the patients who continued empagliflozin administration compared to those with metformin and sitagliptin alone (Supplementary Fig. 4D).
RESULTS
- In the drug-naïve patients with decompensated T2DM, initial triple therapy using metformin, sitagliptin, and empagliflozin resulted in sustained, rapid, and satisfactory glucose control without severe adverse events. With this initial triple therapy, the HbA1c level decreased from 11.0%±1.8% at the baseline to 7.0%±1.7% at 24 months. Fasting plasma glucose levels also decreased significantly at 2 months. These glycemic benefits were maintained for 24 months and are linked to favorable changes in the surrogate markers for insulin resistance and β-cell function as reported [27].
- Over 70% of patients who were treated with sulfonylurea or insulin eventually failed to achieve the target HbA1c level (<7.0%) over 9 years in the UK Prospective Diabetes Study [28]. By contrast, in the present study, the target goal achievement rate was >70% for glycemic target after this initial triple therapy (Supplementary Fig. 1A). In terms of β-cell function, which can be significantly impaired by glucotoxicity, there was greater improvement in HOMA-β in the patients with initial HbA1c ≥9.5% compared to those with initial HbA1c <9.5% (29.9%±7.8% vs. 18.2%±21.1%, P<0.05).
- SGLT2 inhibitors are known to increase serum concentrations of ketone bodies in patients with T2DM [29,30]. Intriguingly, the initial triple therapy including empagliflozin in this study decreased both glucose and ketone levels, particularly in the patients with high ketone levels at baseline (>200 μmol/L). It can be speculated that it was mainly due to the improvement of severe hyperglycemia, which is commonly accompanied by high ketone level. The changes in ketone bodies exhibited different trends according to the baseline HbA1c level. In patients with baseline HbA1c >10.0%, the total concentration of ketone bodies decreased significantly whereas in those with HbA1c ≤10.0%, its reduction was modest and not significant. Intriguingly, the ketone body concentration in the patients with high initial level (≥200 μmol/L) decreased substantially whereas it did not change significantly in those with an initially low level (<200 μmol/L). In addition, concomitant administration of sitagliptin, a DPP4 inhibitor, which is known to decrease glucagon secretion from pancreatic α-cells, might be able to contribute to decrease in ketone body concentration [31].
- The initial triple therapy induced favorable changes in the metabolic profile. Body fat percent decreased and muscle percent increased, which is expected because of SGLT2 inhibition (Fig. 2) [32]. Whole-body muscle percentage increased significantly from 5 months and was maintained at 24 months. These findings suggest that favorable alterations in body composition may be expected from this triple combination therapy.
- Previous studies have reported a slight increase in LDL-C level after SGLT2 inhibitor therapy [33]. By contrast, our initial triple therapy significantly improved the lipid profile by decreasing LDL-C and triglyceride levels and increasing HDL-C levels (Table 1). This difference may stem from the concomitant treatment with a DPP4 inhibitor or general improvements in glucose and lipid metabolism induced by the triple therapy. In addition, the plasma free fatty acid levels also decreased (Fig. 3E).
- SGLT2 inhibitors provide protection against kidney injurytection effects of an SGLT2 inhibitor. For example, the eGFRCKD-EPI and urinary protein/creatinine and albumin/creatinine ratios remained stable for 24 months. eGFR-CKD-EPI declines at a rate of 1.4 mL/min/1.73 m2/year among people without diabetes, at 1.8 mL/min/1.73 m2/year in those with undiagnosed diabetes, and at 2.5 mL/min/1.73 m2/year in those with diagnosed diabetes [35]. In our study, eGFR-CKD-EPI decreased by 2.32 mL/min/1.73 m2 over the 24 months of the initial triple therapy, which is slightly lower than the rate in people without diabetes.
- A range of liver diseases often accompany T2DM [36]. Insulin resistance is thought to be a common pathophysiological mechanism of both T2DM and NAFLD [37]. In a previous report [38], initial triple therapy reduced the concentrations of hepatic function markers AST and ALT within the normal range up to 5 months. Improvements in fatty liver markers were reported by a study of an SGLT2 inhibitor [38], a finding that may relate to reductions in both liver and abdominal fat. The triple therapy showed beneficial effects on liver fat stores [39]. The principle behind the initial triple therapy management of NAFLD involves an indirect effect through improvements in insulin resistance and glycemia, and it may also relate to the treatment of T2DM [40].
- The initial triple therapy was well tolerated, and no patient withdrew because of adverse events. The rate of hypoglycemia was lower than in other studies [41]. No serious adverse events, such as hypoglycemia, genitourinary infection, ketoacidosis, or retinopathy progression, were observed during the 24-month study period.
- Reducing the number of medications in diabetes management is a major concern from both the remission and drugrelated side effects perspectives [42]. It was reported that 12 weeks of treatment with metformin, dapagliflozin, and insulin triple therapy was not long enough to justify stopping the medication because HbA1c level rebounded in >50% of the patients [43]. However, it should be noted that they involved patients who had already been diagnosed with diabetes for an average of 3 years and were mostly taking glucose-lowering medications at the start of the study. In contrast, in our study, the reduced HbA1c level was well maintained after omitting either an SGLT2 inhibitor or a DPP4 inhibitor after good glycemic control for 12 months with initial triple therapy (Supplementary Fig. 4). Further long-term and well-designed studies are needed to support this idea.
- This study has limitations. First, this was a single-arm study that did not allow comparison with different regimens. Second, the power of the subgroup analyses may have been limited because the study was not designed primarily to investigate differences according to the changes in regimens.
- In conclusion, the initial combination therapy of metformin, sitagliptin, and empagliflozin for drug-naïve patients with T2DM with a high HbA1c level decreased glucose level rapidly and markedly without inducing clinically significant adverse events. It is noteworthy that the improved glycemic regulation lasted up to 24 months without any rebound in HbA1c level. Further benefits such as improved insulin sensitivity, β-cell function, body composition, and metabolic profile including blood lipid levels, liver enzymes, and renal protection were also identified. These findings suggest that initial triple combination therapy targeting different pathophysiological abnormalities in T2DM is a viable option for inducing normoglycemia rapidly and safely in patients with T2DM and high HbA1c level.
DISCUSSION
SUPPLEMENTARY MATERIALS
Supplementary Table 2.
Supplementary Fig. 1.
Supplementary Fig. 2.
Supplementary Fig. 3.
Supplementary Fig. 4.
-
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
AUTHOR CONTRIBUTIONS
Conception or design: S.L.
Acquisition, analysis, or interpretation of data: Y.H.P., M.S., S.Y.L., S.L.
Drafting the work or revising: Y.H.P., M.S., S.Y.L.
Final approval of the manuscript: Y.H.P., M.S., S.Y.L., S.L.
-
FUNDING
This work was supported by Seoul National University Bundang Hospital.
NOTES
-
Acknowledgements
- None



| Variable | Baseline (n=170) | 12 months (n=135) | 24 months (n=112) |
|---|---|---|---|
| Body weight, kg | 73.3±16.4 | 73.4±15.8 | 73.7±15.4 |
| BMI, kg/m2 | 25.9±4.4 | 25.6±4.3 | 25.9±4.0 |
| Systolic blood pressure, mm Hg | 131.6±15.0 | 131.4±16.4 | 132.7±16.0 |
| Diastolic blood pressure, mm Hg | 80.3±10.7 | 80.8±11.4 | 79.7±12.9 |
| HbA1c, % | 11.0±1.8 | 6.5±1.2a | 7.0±1.7a |
| Fasting glucose, mg/dL | 235.7±78.5 | 127.6±36.3a | 133.6±48.1a |
| Fasting insulin, μIU/mL | 9.0±4.6 | 8.1±4.0 | 8.1±3.5 |
| Fasting C-peptide, ng/mL | 3.0±1.7 | 2.6±1.4a | 2.4±1.1a |
| Fasting glucagon, pg/mLb | 172.7±115.1 | 222.7±165.7a | 202.6±138.4 |
| HOMA-IR | 5.1±2.5 | 2.5±1.6a | 2.6±1.4a |
| HOMA-β | 25.3±22.6 | 55.4±34.0a | 52.5±28.0a |
| Total cholesterol, mg/dL | 197.8±53.9 | 173.4±45.4a | 170.9±40.3a |
| Triglycerides, mg/dL | 195.8±214.3 | 137.6±89.4a | 153.4±118.7a |
| HDL-C, mg/dL | 48.7±11.9 | 51.0±11.0a | 50.8±11.0a |
| LDL-C, mg/dL | 119.9±40.4 | 105.0±34.5a | 104.9±34.6a |
| Serum creatinine, mg/dL | 0.77±0.19 | 0.80±0.20 | 0.80±0.19 |
| eGFR-CKD-EPI, mL/min/1.73 m2 | 101.8±16.8 | 99.0±16.7 | 98.0±15.5a |
| Uric acid, mg/dL | 4.7±1.5 | 5.0±1.5a | 5.3±1.6a |
| AST, IU/L | 33.4±27.1 | 28.0±12.2a | 28.2±12.1a |
| ALT, IU/L | 40.9±43.2 | 32.8±27.3a | 34.9±26.1 |
| Total ketone, μmol/Lb | 602.1±1,291.4 | 156.2±177.2a | 174.0±189.4a |
| β-Hydroxybutyrate, μmol/Lb | 446.6±1,016.2 | 106.1±124.0a | 121.4±141.1a |
| Acetoacetate, μmol/Lb | 155.5±278.2 | 50.1±56.0a | 52.6±49.7a |
| Urinary protein/Cr ratio, mg/gb | 235.5±935.4 | 200.6±532.5a | 159.7±317.8a |
| Urinary albumin/Cr ratio, mg/gb | 107.4±658.3 | 102.3±438.6a | 77.3±267.1a |
| WBC, 1012/L | 7.4±2.2 | 8.9±5.8 | 7.3±2.1 |
| Hemoglobin, g/dL | 14.9±1.8 | 14.3±2.4 | 14.7±2.2 |
| Hematocrit, % | 43.9±4.9 | 43.1±7.0 | 45.1±3.9 |
| Platelets, 109/L | 250.5±73.7 | 241.8±120.3 | 247.3±54.5 |
Values are presented as mean±standard deviation.
BMI, body mass index; HbA1c, glycosylated hemoglobin; HOMA-IR, homeostasis model assessment of insulin resistance; HOMA-β, homeostasis model assessment of β-cell function; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; eGFRCKD-EPI, estimated glomerular filtration rate by Chronic Kidney Disease Epidemiology Collaboration equation; AST, aspartate aminotransferase; ALT, alanine aminotransferase; Cr, creatinine; WBC, white blood cell.
a P<0.05,
b Logarithmically transformed values were used for comparisons of fasting concentrations of glucagon, total ketone bodies, β-hydroxybutyrate, acetoacetate, urinary protein/creatinine ratio, and urinary albumin/creatinine ratio.
- 1. Action to Control Cardiovascular Risk in Diabetes Study Group, Gerstein HC, Miller ME, Byington RP, Goff DC Jr, Bigger JT, et al. Effects of intensive glucose lowering in type 2 diabetes. N Engl J Med 2008;358:2545-59.ArticlePubMedPMC
- 2. Holman RR, Paul SK, Bethel MA, Matthews DR, Neil HA. 10-Year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med 2008;359:1577-89.ArticlePubMed
- 3. Gaede P, Lund-Andersen H, Parving HH, Pedersen O. Effect of a multifactorial intervention on mortality in type 2 diabetes. N Engl J Med 2008;358:580-91.ArticlePubMed
- 4. Juarez DT, Ma C, Kumasaka A, Shimada R, Davis J. Failure to reach target glycated a1c levels among patients with diabetes who are adherent to their antidiabetic medication. Popul Health Manag 2014;17:218-23.ArticlePubMedPMC
- 5. Cersosimo E, Johnson EL, Chovanes C, Skolnik N. Initiating therapy in patients newly diagnosed with type 2 diabetes: combination therapy vs a stepwise approach. Diabetes Obes Metab 2018;20:497-507.ArticlePubMedPDF
- 6. Inzucchi SE, Bergenstal RM, Buse JB, Diamant M, Ferrannini E, Nauck M, et al. Management of hyperglycaemia in type 2 diabetes, 2015: a patient-centred approach. Update to a position statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetologia 2015;58:429-42.ArticlePubMedPDF
- 7. Zinman B. Initial combination therapy for type 2 diabetes mellitus: is it ready for prime time? Am J Med 2011;124(1 Suppl):S19-34.ArticlePubMed
- 8. Cahn A, Cefalu WT. Clinical considerations for use of initial combination therapy in type 2 diabetes. Diabetes Care 2016;39(Suppl 2):S137-45.ArticlePubMedPMCPDF
- 9. Phung OJ, Sobieraj DM, Engel SS, Rajpathak SN. Early combination therapy for the treatment of type 2 diabetes mellitus: systematic review and meta-analysis. Diabetes Obes Metab 2014;16:410-7.ArticlePubMed
- 10. Wu D, Li L, Liu C. Efficacy and safety of dipeptidyl peptidase-4 inhibitors and metformin as initial combination therapy and as monotherapy in patients with type 2 diabetes mellitus: a meta-analysis. Diabetes Obes Metab 2014;16:30-7.ArticlePubMed
- 11. Matthews DR, Paldanius PM, Proot P, Chiang Y, Stumvoll M, Del Prato S, et al. Glycaemic durability of an early combination therapy with vildagliptin and metformin versus sequential metformin monotherapy in newly diagnosed type 2 diabetes (VERIFY): a 5-year, multicentre, randomised, double-blind trial. Lancet 2019;394:1519-29.ArticlePubMed
- 12. Davies MJ, D’Alessio DA, Fradkin J, Kernan WN, Mathieu C, Mingrone G, et al. Management of hyperglycemia in type 2 diabetes, 2018: a consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2018;41:2669-701.ArticlePubMedPMCPDF
- 13. American Diabetes Association Professional Practice Committee. 9. Pharmacologic approaches to glycemic treatment: standards of medical care in diabetes-2022. Diabetes Care 2022;45(Suppl 1):S125-43.ArticlePubMedPDF
- 14. Ko SH, Hur KY, Rhee SY, Kim NH, Moon MK, Park SO, et al. Antihyperglycemic agent therapy for adult patients with type 2 diabetes mellitus 2017: a position statement of the Korean Diabetes Association. Diabetes Metab J 2017;41:337-48.ArticlePubMedPMCPDF
- 15. Abdul-Ghani MA, Puckett C, Triplitt C, Maggs D, Adams J, Cersosimo E, et al. Initial combination therapy with metformin, pioglitazone and exenatide is more effective than sequential add-on therapy in subjects with new-onset diabetes: results from the Efficacy and Durability of Initial Combination Therapy for Type 2 Diabetes (EDICT): a randomized trial. Diabetes Obes Metab 2015;17:268-75.PubMedPMC
- 16. Lim S, Ku EJ, Lee SY, Lee JH, Lee JE, Kim KM, et al. Therapeutic efficacy and safety of initial triple combination of metformin, sitagliptin, and lobeglitazone in drug-naive patients with type 2 diabetes: initial triple study. BMJ Open Diabetes Res Care 2020;8:e000807.PubMedPMC
- 17. Scirica BM, Bhatt DL, Braunwald E, Steg PG, Davidson J, Hirshberg B, et al. Saxagliptin and cardiovascular outcomes in patients with type 2 diabetes mellitus. N Engl J Med 2013;369:1317-26.ArticlePubMed
- 18. Pratley RE, Eldor R, Raji A, Golm G, Huyck SB, Qiu Y, et al. Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with type 2 diabetes mellitus inadequately controlled with metformin: the VERTIS FACTORIAL randomized trial. Diabetes Obes Metab 2018;20:1111-20.PubMedPMC
- 19. Lim S, Sohn M, Shin Y, Ferrannini E. Initial combination of metformin, sitagliptin, and empagliflozin in drug-naive patients with type 2 diabetes: safety and metabolic effects. Diabetes Obes Metab 2022;24:757-62.PubMed
- 20. Ji L, Chan JC, Yu M, Yoon KH, Kim SG, Choi SH, et al. Early combination versus initial metformin monotherapy in the management of newly diagnosed type 2 diabetes: an East Asian perspective. Diabetes Obes Metab 2021;23:3-17.
- 21. Wu Q, Liu M, Fang Z, Li C, Zou F, Hu L, et al. Efficacy and safety of empagliflozin at different doses in patients with type 2 diabetes mellitus: a network meta-analysis based on randomized controlled trials. J Clin Pharm Ther 2022;47:270-86.ArticlePubMedPDF
- 22. Ozcelik S, Celik M, Vural A, Aydin B. The effect of low and high dose empagliflozin on HbA1c and lipid profile in type 2 diabetes mellitus: a real-world data. North Clin Istanb 2019;7:167-73.PubMedPMC
- 23. Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC. Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985;28:412-9.ArticlePubMedPDF
- 24. Jeong S, Kim K, Chang J, Choi S, Kim SM, Son JS, et al. Development of a simple nonalcoholic fatty liver disease scoring system indicative of metabolic risks and insulin resistance. Ann Transl Med 2020;8:1414.ArticlePubMedPMC
- 25. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001;285:2486-97.ArticlePubMed
- 26. Kim BY, Kang SM, Kang JH, Kang SY, Kim KK, Kim KB, et al. 2020 Korean Society for the Study of Obesity guidelines for the management of obesity in Korea. J Obes Metab Syndr 2021;30:81-92.ArticlePubMedPMC
- 27. Hou X, Liu J, Song J, Wang C, Liang K, Sun Y, et al. Relationship of hemoglobin A1c with β cell function and insulin resistance in newly diagnosed and drug naive type 2 diabetes patients. J Diabetes Res 2016;2016:8797316.ArticlePubMedPMCPDF
- 28. Turner RC, Cull CA, Frighi V, Holman RR. Glycemic control with diet, sulfonylurea, metformin, or insulin in patients with type 2 diabetes mellitus: progressive requirement for multiple therapies (UKPDS 49). UK Prospective Diabetes Study (UKPDS) Group. JAMA 1999;281:2005-12.ArticlePubMed
- 29. Polidori D, Iijima H, Goda M, Maruyama N, Inagaki N, Crawford PA. Intra- and inter-subject variability for increases in serum ketone bodies in patients with type 2 diabetes treated with the sodium glucose co-transporter 2 inhibitor canagliflozin. Diabetes Obes Metab 2018;20:1321-6.ArticlePubMedPMCPDF
- 30. Shin Y, Choi H, Lim S. Comparison betweeen dapagliflozin add-on therapy and insulin dose escalation in patients with uncontrolled type 2 diabetes treated with insulin: DVI study. Diabetes Res Clin Pract 2021;175:108843.ArticlePubMed
- 31. Omar B, Ahren B. Pleiotropic mechanisms for the glucose-lowering action of DPP-4 inhibitors. Diabetes 2014;63:2196-202.ArticlePubMedPDF
- 32. Szekeres Z, Toth K, Szabados E. The effects of SGLT2 inhibitors on lipid metabolism. Metabolites 2021;11:87.ArticlePubMedPMC
- 33. Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, Hantel S, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med 2015;373:2117-28.ArticlePubMed
- 34. Neuen BL, Young T, Heerspink HJ, Neal B, Perkovic V, Billot L, et al. SGLT2 inhibitors for the prevention of kidney failure in patients with type 2 diabetes: a systematic review and meta-analysis. Lancet Diabetes Endocrinol 2019;7:845-54.ArticlePubMed
- 35. Warren B, Rebholz CM, Sang Y, Lee AK, Coresh J, Selvin E, et al. Diabetes and trajectories of estimated glomerular filtration rate: a prospective cohort analysis of the atherosclerosis risk in communities study. Diabetes Care 2018;41:1646-53.ArticlePubMedPMCPDF
- 36. Hickman IJ, Macdonald GA. Impact of diabetes on the severity of liver disease. Am J Med 2007;120:829-34.ArticlePubMed
- 37. Rhee EJ. Nonalcoholic fatty liver disease and diabetes: an epidemiological perspective. Endocrinol Metab (Seoul) 2019;34:226-33.ArticlePubMedPMCPDF
- 38. Seino Y, Inagaki N, Haneda M, Kaku K, Sasaki T, Fukatsu A, et al. Efficacy and safety of luseogliflozin added to various oral antidiabetic drugs in Japanese patients with type 2 diabetes mellitus. J Diabetes Investig 2015;6:443-53.ArticlePubMedPMCPDF
- 39. Johansson L, Hockings PD, Johnsson E, Dronamraju N, Maaske J, Garcia-Sanchez R, et al. Dapagliflozin plus saxagliptin add-on to metformin reduces liver fat and adipose tissue volume in patients with type 2 diabetes. Diabetes Obes Metab 2020;22:1094-101.ArticlePubMedPMCPDF
- 40. Dharmalingam M, Yamasandhi PG. Nonalcoholic fatty liver disease and type 2 diabetes mellitus. Indian J Endocrinol Metab 2018;22:421-8.ArticlePubMedPMC
- 41. Diabetes Control and Complications Trial Research Group, Nathan DM, Genuth S, Lachin J, Cleary P, Crofford O, et al. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med 1993;329:977-86.ArticlePubMed
- 42. Rea F, Ciardullo S, Savare L, Perseghin G, Corrao G. Comparing medication persistence among patients with type 2 diabetes using sodium-glucose cotransporter 2 inhibitors or glucagon-like peptide-1 receptor agonists in real-world setting. Diabetes Res Clin Pract 2021;180:109035.ArticlePubMed
- 43. McInnes N, Hall S, Sultan F, Aronson R, Hramiak I, Harris S, et al. Remission of type 2 diabetes following a short-term intervention with insulin glargine, metformin, and dapagliflozin. J Clin Endocrinol Metab 2020;105:dgaa248.ArticlePubMedPDF
 PubReader
PubReader ePub Link
ePub Link Cite
Cite