- Current
- Browse
- Collections
-
For contributors
- For Authors
- Instructions to authors
- Article processing charge
- e-submission
- For Reviewers
- Instructions for reviewers
- How to become a reviewer
- Best reviewers
- For Readers
- Readership
- Subscription
- Permission guidelines
- About
- Editorial policy
Articles
- Page Path
- HOME > Diabetes Metab J > Volume 48(1); 2024 > Article
-
Original ArticleDrug/Regimen Comparative Efficacy of Rosuvastatin Monotherapy and Rosuvastatin/Ezetimibe Combination Therapy on Insulin Sensitivity and Vascular Inflammatory Response in Patients with Type 2 Diabetes Mellitus
-
Ji Hye Han1*
 , Kyong Hye Joung1,2*, Jun Choul Lee3, Ok Soon Kim1, Sorim Choung4, Ji Min Kim1,2, Yea Eun Kang1, Hyon-Seung Yi1,5, Ju Hee Lee1, Bon Jeong Ku1, Hyun Jin Kim1
, Kyong Hye Joung1,2*, Jun Choul Lee3, Ok Soon Kim1, Sorim Choung4, Ji Min Kim1,2, Yea Eun Kang1, Hyon-Seung Yi1,5, Ju Hee Lee1, Bon Jeong Ku1, Hyun Jin Kim1 -
Diabetes & Metabolism Journal 2024;48(1):112-121.
DOI: https://doi.org/10.4093/dmj.2022.0402
Published online: January 3, 2024
1Division of Endocrinology and Metabolism, Department of Internal Medicine, Chungnam National University College of Medicine, Daejeon, Korea
2Division of Endocrinology and Metabolism, Department of International Medicine, Chungnam National University Sejong Hospital, Sejong, Korea
3Division of Endocrinology and Metabolism, Department of Internal Medicine, Eulji University School of Medicine, Daejeon, Korea
4Department of Medical Science, Chungnam National University College of Medicine, Daejeon, Korea
5Laboratory of Endocrinology and Immune System, Chungnam National University College of Medicine, Daejeon, Korea
-
Corresponding authors: Hyun Jin Kim Division of Endocrinology and Metabolism, Department of Internal Medicine, Chungnam National University College of Medicine, 282 Munhwa-ro, Jung-gu, Daejeon 35015, Korea E-mail: kimhj43@cnuh.co.kr
-
Bon Jeong Ku Division of Endocrinology and Metabolism, Department of Internal Medicine, Chungnam National University College of Medicine, 282 Munhwa-ro, Jung-gu, Daejeon 35015, Korea E-mail: bonjeong@cnu.ac.kr
- *Ji Hye Han and Kyong Hye Joung contributed equally to this study as first authors.
Copyright © 2024 Korean Diabetes Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Background
- Type 2 diabetes mellitus (T2DM) induces endothelial dysfunction and inflammation, which are the main factors for atherosclerosis and cardiovascular disease. The present study aimed to compare the effects of rosuvastatin monotherapy and rosuvastatin/ezetimibe combination therapy on lipid profile, insulin sensitivity, and vascular inflammatory response in patients with T2DM.
-
Methods
- A total of 101 patients with T2DM and dyslipidemia were randomized to either rosuvastatin monotherapy (5 mg/day, n=47) or rosuvastatin/ezetimibe combination therapy (5 mg/10 mg/day, n=45) and treated for 12 weeks. Serum lipids, glucose, insulin, soluble intercellular adhesion molecule-1 (sICAM-1), and peroxiredoxin 4 (PRDX4) levels were determined before and after 12 weeks of treatment.
-
Results
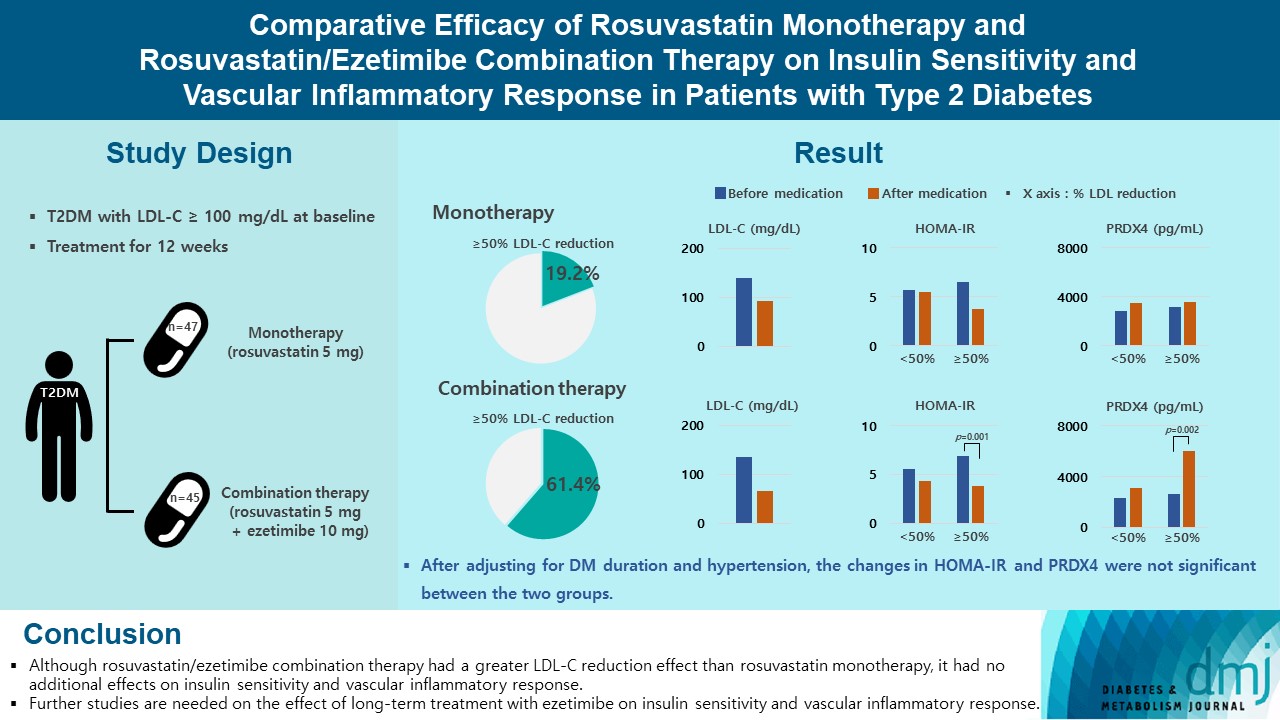
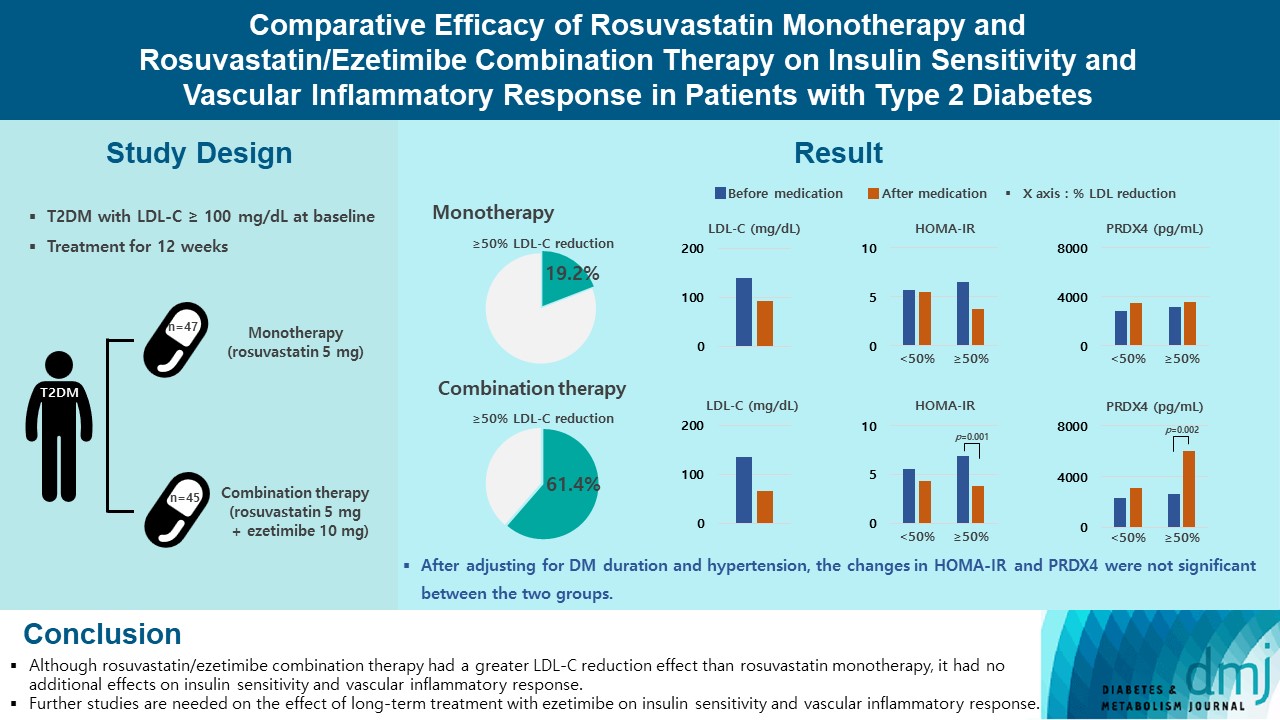
- The reduction in low density lipoprotein cholesterol (LDL-C) by more than 50% from baseline after treatment was more in the combination therapy group. The serum sICAM-1 levels increased significantly in both groups, but there was no difference between the two groups. The significant changes in homeostasis model assessment of insulin resistance (HOMA-IR) and PRDX4 were confirmed only in the subgroup in which LDL-C was reduced by 50% or more in the combination therapy group. However, after adjusting for diabetes mellitus duration and hypertension, the changes in HOMA-IR and PRDX4 were not significant between the two groups.
-
Conclusion
- Although rosuvastatin/ezetimibe combination therapy had a greater LDL-C reduction effect than rosuvastatin monotherapy, it had no additional effects on insulin sensitivity and vascular inflammatory response. Further studies are needed on the effect of long-term treatment with ezetimibe on insulin sensitivity and vascular inflammatory response.
- Type 2 diabetes mellitus (T2DM) induces endothelial dysfunction and inflammation via several different pathways following atherosclerosis. Endothelial dysfunction and inflammation are the main mechanisms underlying cardiovascular disease, diabetic nephropathy, and diabetic retinopathy [1-3]. Oxidative stress and vascular inflammation are major factors in the progression of T2DM and its vascular complications. Associated biomarkers can be used as parameters to determine treatment efficacy [4].
- Majority of the clinical guidelines initially recommend the use of a statin in patients with dyslipidemia and diabetes. In cases wherein the target levels for low density lipoprotein cholesterol (LDL-C) are not achieved with statin treatment alone, combination therapy with ezetimibe is recommended [5,6]. Statins inhibit 3-hydroxy-3-methylglutaryl coenzyme A reductase, decreasing cholesterol production in the liver. Meanwhile, ezetimibe is a cholesterol absorption inhibitor that functions in the small intestine through direct binding with Niemann-Pck C1-like 1, avoiding the reabsorption of intrinsic cholesterol, which is released to the intestine as bile acid, resulting in its excretion. The combination therapy of statin and ezetimibe lowers the level of LDL-C by 15% to 20% more than that achieved by statin monotherapy; furthermore, it exhibits additional cardiovascular benefits [7]. Impaired Reduction of Outcomes: Vytorin Efficacy International Trial (IMPROVE-IT) demonstrated that combination therapy of ezetimibe with simvastatin can better reduce LDL-C levels and result in 6.4% lower rates of major adverse cardiovascular events than that observed with simvastatin monotherapy in patients with acute coronary syndrome. The benefits were profound, particularly in patients with diabetes having a hazard ratio of 0.86 [8]. Since side effects, such as hepatotoxicity, myopathy, and elevated serum glucose, are frequently associated with a high dose of statin or the use of a potent statin, combination therapy with ezetimibe can allow for lower dose of statin and similar reduction in the level of LDL-C [9]. However, limited studies have investigated the effect of ezetimibe and statin combination therapy on insulin resistance, and vascular inflammation. Studies evaluating the benefits of combination therapy beyond those of lowering LDL-C levels or cardiovascular benefits are needed [10].
- The aim of this study was to compare the efficacy of 5 mg rosuvastatin monotherapy with that of 5 mg rosuvastatin/10 mg ezetimibe combination therapy on lipid parameters, insulin resistance, and vascular inflammation response-related biomarkers in patients with T2DM.
INTRODUCTION
- Study design
- Among the patients with T2DM who visited the outpatient clinic of the Endocrinology Department of Chungnam National University Hospital from May 2017 to December 2018, those with LDL-C levels ≥100 mg/dL at baseline were included in the study. Exclusion criteria involved ongoing treatment with a lipid-lowering agent, ongoing hormone replacement therapy post-menopause, serum aspartate transaminase or alanine transaminase levels more than two times the normal highest value, serum creatine phosphokinase level more than three times the normal highest value, malignant neoplasm, uncontrolled hypothyroidism, and hypersensitivity or resistance to rosuvastatin or ezetimibe. After screening, 101 participants were randomized into the rosuvastatin group (n=47) administered rosuvastatin 5 mg/day and the rosuvastatin/ezetimibe group (n=45) administered rosuvastatin 5 mg/day with ezetimibe 10 mg/day.
- This study was carried out in compliance with the Declaration of Helsinki. Written informed consent was obtained from all participants, and the study was approved by the Internal Review Board (IRB) of Chungnam National University Hospital (CNUH 2016-06-032).
- Biochemical data
- After fasting for a minimum of 8 hours, blood samples were collected in ethylenediaminetetraacetic acid tubes, and the lipid profiles, including high density lipoprotein cholesterol (HDL-C), LDL-C, total cholesterol, and triglycerides (TGs), were measured using a blood chemistry analyzer (Hitachi 747, Hitachi, Tokyo, Japan). Insulin was quantified using an immunoradiometric assay kit (Insource INS-IRMA Kit, DIAsource, Louvain-la-Nerve, Belgium). Glycosylated hemoglobin (HbA1c) level was measured using high-performance liquid chromatography (BioRad, Hercules, CA, USA). The homeostasis model assessment of insulin resistance (HOMA-IR) and homeostasis model assessment of β-cell function (HOMA-β) levels were calculated using the following equations:
- Serum levels of soluble intercellular adhesion molecule-1 (sICAM-1) and peroxiredoxin 4 (PRDX4) were measured using the quantitative sandwich enzyme immunoassay technique with enzyme-linked immunosorbent assay kits (Human ICAM-1/CD54 Allele-specific Immunoassay kit, Catalog number: DCD 540, R&D Systems, Abingdon, England; Human PRDX4 ELISA kit, Catalog number: KA2121, Abnova, Taipei, Taiwan).
- Statistical analyses
- Values for all the parameters were calculated as the mean±standard deviation. A P value of <0.05 was considered statistically significant. The Student’s t-test and chi-square test were used to compare data between the two groups. The paired samples t-test and analysis of covariance were used to compare the biochemical data at baseline and after 12 weeks of treatment. For biochemical analyses, variations values obtained before and after 12 weeks of treatment in each group were compared using the Wilcoxon signed-rank test and analysis of covariance (ANCOVA). Statistical analyses were performed using SPSS version 25.0 (SPSS Inc., Chicago, IL, USA).
METHODS
- Recruitment and treatment flow
- Supplementary Fig. 1 shows the recruitment process of the study patients. We recruited patients with T2DM who visited Endocrinology Department of Chungnam National University Hospital from May 2017 to December 2018. Nine participants dropped out because of skin allergic reactions, myalgia, or were lost to follow-up. Ninety-two participants were included in the final analysis. Blood samples were obtained from all participants for the measurement of biochemical markers at baseline and after 12 weeks of treatment.
- Baseline characteristics
- Table 1 shows the baseline characteristics of the study participants. The mean age is not significantly different between the rosuvastatin and the rosuvastatin/ezetimibe groups. Sex, height, weight, and body mass index are not significantly different between the two groups. The diabetes mellitus (DM) duration is longer in the rosuvastatin group than in the rosuvastatin/ezetimibe group (P=0.037). A higher number of participants in the rosuvastatin group are on anti-hypertensive medication than those in the rosuvastatin/ezetimibe group (P=0.049). Differences between the two groups for lipid profile and other parameters, including HbA1c, HOMR-IR, HOMA-β, sICAM-1, and PRDX4, are statistically insignificant.
- Changes in lipid parameters
- LDL-C levels decreased in both groups after treatment (Table 2). Variations in LDL-C levels were −47.60±30.38 mg/dL (−33.78%±19.92%) and −69.38±25.46 mg/dL (−50.86%±16.51%) in the rosuvastatin and rosuvastatin/ezetimibe groups, respectively (P<0.001) (Supplementary Table 1 and Supplementary Fig. 2A). The number of patients with LDL-C levels below 100 mg/dL after 12 weeks was 33 (70.2%) and 43 (95.6%) in the rosuvastatin and rosuvastatin/ezetimibe groups, respectively. The number of patients with LDL-C levels under 70 mg/dL after 12 weeks was 11 (23.4%) and 27 (60.0%) in the rosuvastatin and the rosuvastatin/ezetimibe groups, respectively (data not shown). In the rosuvastatin and rosuvastatin/ezetimibe groups, 19.15% and 62.22% patients, respectively, exhibited at least 50% reduction in LDL-C levels after 12 weeks (Supplementary Fig. 2B). In addition, serum TGs levels decreased in both groups after treatment. However, no difference was found in serum HDL-C levels (Table 2).
- Changes in parameters related to glucose metabolism
- Although changes in serum glucose and HbA1c levels before and after treatment in both groups were not significant, serum insulin levels decreased in the rosuvastatin/ezetimibe group (P<0.001) and not in the rosuvastatin group (P=0.186) (Table 2). The changes in insulin before and after treatment also showed a significant difference between both groups (P=0.048) (Supplementary Table 1). However, after calibration with the change in LDL-C levels, the difference was not significant (P=0.148) (Supplementary Table 1). HOMA-IR and HOMA-β also decreased only in the rosuvastatin/ezetimibe group (HOMA-IR, P=0.002; HOMA-β, P=0.005) (Table 2); however, the changes before and after treatment were similar in both groups (Supplementary Table 1).
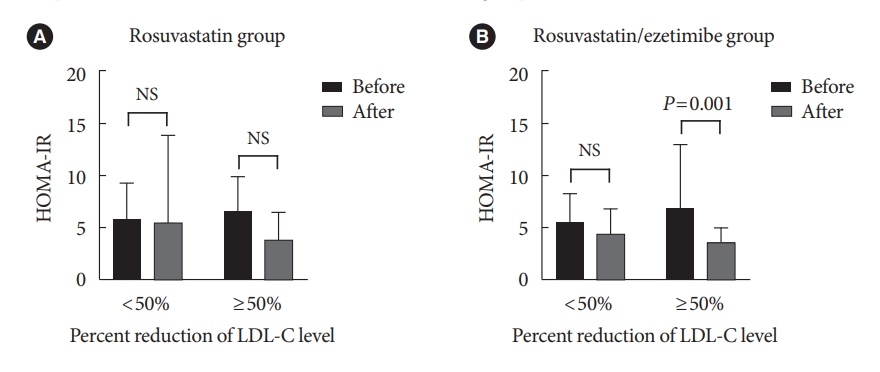
- To evaluate the effect of lowering LDL-C levels on the change in HOMA-IR level, subgroup analysis was performed (Fig. 1). Each group was divided based on post-treatment percent decrease in LDL-C levels. By dividing all the patients into two subgroups according to percent decrease in LDL-C levels after treatment, HOMA-IR levels decreased only in the subgroup with ≥50% reduction in LDL-C levels (P=0.001), and no difference was observed in HOMA-IR levels in the subgroup with <50% reduction in LDL-C levels (Table 3). In the rosuvastatin group, no difference was observed before and after treatment in both the subgroups (Table 3 and Fig. 1A). In the rosuvastatin/ezetimibe group, HOMA-IR levels decreased only in the subgroup with ≥50% reduction in LDL-C levels (P=0.001) (Table 3 and Fig. 1B). Because DM duration and hypertension could affect the change in HOMA-IR, we checked whether there were differences in DM duration and hypertension between subgroups divided by percent change of LDL-C after treatment. There was no difference between subgroups in each group (Table 3 and Supplymentary Table 2). In addition, after calibration with DM duration and hypertension, the difference was not significant between the two subgroups with ≥50% reduction in LDL-C levels (P=0.689) (data not shown).
- Change in the levels of serum PRDX4 and sICAM-1
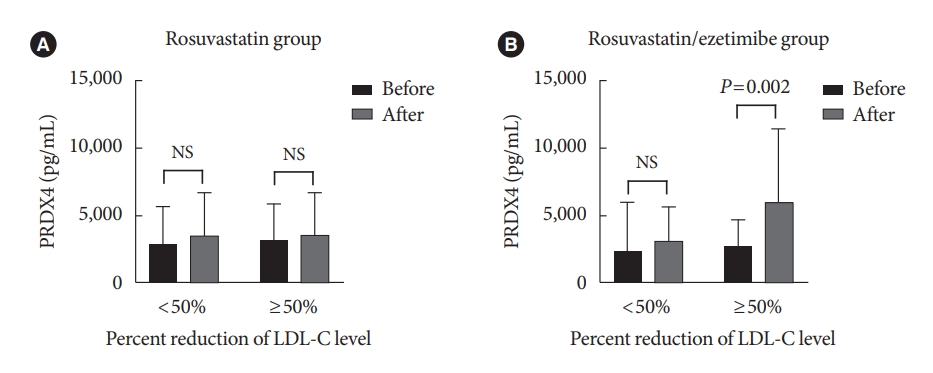
- We measured the serum levels of PRDX4, an antioxidative protein, to evaluate its effect on oxidative stress. Serum PRDX4 levels were unchanged in the rosuvastatin group (P=0.324) but increased in the rosuvastatin/ezetimibe group (P=0.007) (Table 2). The change in serum PRDX4 levels between the two groups was statistically insignificant (P=0.102) (Supplementary Table 1). Dividing all the patients into two subgroups according to percent decrease in LDL-C levels after treatment, serum PRDX4 levels increased only in the subgroup with ≥50% reduction in LDL-C levels (P=0.004), and no difference was observed in LDL-C levels in the subgroup with <50% reduction in LDL-C levels (P=0.090) (Table 4). In the rosuvastatin group, the serum PRDX4 levels were similar before and after treatment (Fig. 2A). In the rosuvastatin/ezetimibe group, serum PRDX4 levels increased only in the subgroup with ≥50% reduction in LDL-C levels (P=0.002) (Fig. 2B). However, after calibration with DM duration and hypertension, there was no difference between subgroups in each group (Table 4) and between the two subgroups with ≥50% reduction in LDL-C levels (P=0.103) (data not shown).
- Levels of serum sICAM-1, a maker of endothelial activation, increased in both the groups (rosuvastatin group, P=0.003; rosuvastatin/ezetimibe group, P=0.001), and the change in serum sICAM-1 levels was similar between the two groups (P=0.232) (Table 2 and Supplementary Table 1).
RESULTS
- In this study, both rosuvastatin/ezetimibe combination therapy and rosuvastatin monotherapy for 12 weeks resulted in significantly reduced levels of LDL-C and TGs in patients with T2DM and dyslipidemia. As expected, the reduction in LDL-C by more than 50% from baseline after treatment was more in the combination therapy group. In both groups, changes in fasting glucose and HbA1c levels were not statistically significant after treatment. However, fasting insulin, calculated HOMA-IR, and HOMA-β were significantly reduced after treatment, only in the combination therapy group. Serum sICAM levels were significantly increased in both groups, but serum PRDX4 levels were significantly increased only in the combination therapy group. Moreover, after adjusting for the effect of reducing LDL-C, changes in HOMA-IR and PRDX4 before and after treatment were statistically significant only in the combination therapy group in which LDL-C level was reduced by more than 50%. However, after adjusting for DM duration and hypertension, the changes in HOMA-IR and PRDX4 were not significant.
- Statins are drugs that lower LDL-C by inhibiting the ratelimiting enzyme in the cholesterol synthesis pathway of hepatocytes and are strongly recommended for primary and secondary prevention of atherosclerotic cardiovascular disease [11,12]. Cardiovascular risk factors, such as hyperglycemia, hypertension, and dyslipidemia cause oxidative stress and low-grade inflammation leading to the inactivation of nitric oxide (NO) [13,14]. NO inactivation induces an imbalance between vasodilators and vasoconstrictors derived endothelial cells (ECs), resulting in endothelial dysfunction [15]. The cardiovascular protective effect of statins is not only due to their lipid-lowering properties but is also related to their effect on improving endothelial function by up-regulating endothelial nitric oxide synthase expression and NO bioavailability. Several clinical studies have demonstrated the effect of statins on ECs by flow mediated dilatation, which is the most common method to measure vascular endothelial function [16,17]. However, the method for measuring flow mediated dilatation, which requires specialized skills, has limitations when being used for evaluating the endothelial function of patients in hospital [18,19].
- PRDXs, which consist of six Prdx isoforms in mammalian cells, are newly identified proteins with a pivotal antioxidative function. These enzymes specifically react with H2O2 and act as regulatory sensors during the transduction of intracellular signaling. PRDX4 is a secretable peroxidase [20,21], and is considered a strong candidate biomarker than other isoforms. A study in mice also revealed that PRDX4 suppresses the induction of atherosclerosis [22]. In addition to the direct association with atherosclerosis, many studies have been conducted on the association between PRDX4 and diabetes. Some studies reported that circulating PRDX4 levels are correlated with the risk of T2DM [23] and the severity of atherosclerosis in T2DM patients with peripheral atherosclerotic disease [24]. Further, studies on PRDX4 by one research group showed that PRDX4 inhibits the progression of type 1 diabetes and improves insulin resistance and fatty liver, resulting in protection from T2DM [25,26]. In addition, a recent study showed that the expression of PRDX4 was higher in proliferating than non-proliferating islet β-cells [27]. In the present study, serum PRDX4 levels were unchanged in the rosuvastatin monotherapy group but increased in the rosuvastatin/ezetimibe combination therapy group after drug treatment. Additionally, in subgroup analysis according to LDL-C reduction (<50% vs. ≥50%), serum PRDX4 levels increased after treatment only in the subgroup in which LDL-C was reduced by more than 50% in the rosuvastatin/ezetimibe combination therapy group and not in patients receiving rosuvastatin monotherapy. Because there was not a statistically significant difference in changes in PRDX4 between the two groups after adjusting for DM duration and hypertension, we cannot conclude that ezetimibe causes increased PRDX4 levels. These results suggest that additional studies targeting patients without hypertension and with a short duration of diabetes are needed to confirm the effect of ezetimibe on insulin sensitivity and oxidative stress.
- ICAM-1, a cell surface glycoprotein and an adhesion receptor, can be found as sICAM-1 in several inflammatory disorders such as atherosclerosis, coronary heart disease, or sepsis [28-30]. sICAM-1 has been shown to promote both pro- and anti-inflammatory responses. At low levels, sICAM-1 led to the release of inflammatory cytokines through activation of nuclear factor κB and extracellular signaling regulated kinase [31]. However, at high levels, sICAM-1 induced EC migration and angiogenesis [32,33], competitively interrupted leukocyte-EC interactions [34] and accelerated the pro-repair activity of immune cells [35]. Statins have been known to affect the expression of ICAM-1. Some studies reported that ICAM-1 was inhibited by statin therapy [36-38]; however, others reported an increased expression [39,40]. Although there are only a few studies on the effect of ezetimibe on ICAM-1, the available results are also controversial. One study reported that ICAM-1 increased following rosuvastatin monotherapy and rosuvastatin/ezetimibe combination therapy but was less in the combination therapy [41]. However, another study reported that ICAM-1 decreased following simvastatin monotherapy and simvastatin/ezetimibe combination therapy but was higher in the combination therapy [42]. In the present study, sICAM-1 levels increased in both groups, with no significant difference in the change in serum sICAM-1 levels between the two groups. These results are inconsistent with previous studies, which could be justified by the difference in participants and patients with relatively long duration of diabetes and by type of statin. Baseline serum sICAM-1 levels in other studies were lower than those in this study, which is assumed to influence this result. To further evaluate this variation, a variable duration and longer treatment study is needed.
- There are concerns about the long-term safety of statin therapy, such as an increased risk of new-onset T2DM [43]. Although the mechanism of statin-induced diabetes is not clear, several clinical studies have accumulated evidence that long-term, high-intensive statin treatment significantly increases the risk of new-onset T2DM [44,45]. Several studies have reported that reduced insulin sensitivity and insulin secretion might result in statin-induced diabetes [43,46], with other studies suggesting that combining ezetimibe with statin might counteract the decrease in insulin sensitivity [47,48]. When HOMA-IR is improved by a certain therapy or factor, HOMA-β is generally expected to be unchanged or improved. However, in our study, both HOMA-IR and HOMA-β were decreased only in the rosuvastatin/ezetimibe combination therapy group in which LDL-C was reduced by more than 50% from baseline. After adjusting for DM duration and hypertension, there was not a statistically significant difference in HOMA-IR change between the two groups. These results suggest that ezetimibe effects on insulin sensitivity might be influenced by several factors such as baseline insulin resistance and insulin secretory capacity. This is a shortcoming to our study in that it failed to clearly determine the reason for these results, and additional research is needed.
- To the best of our knowledge, this is the first study to evaluate the effects of combined therapy of rosuvastatin and ezetimibe on insulin sensitivity and vascular inflammatory response in patients with T2DM. However, this study has several limitations. First, our study targeted a small number of patients (only 92 participants) in a single center for a short period of time (12 weeks). Second, there was a difference in DM duration and occurrence of hypertension between study groups. Third, we measured only two factors associated with vascular inflammation. In the process of vascular inflammation or/and atherosclerosis, the active pathway is different depending on the state of inflammation, and the markers reflecting this state are also changed accordingly. Therefore, it is likely that the difference between the two groups in basic characteristics, including the disease duration and comorbidity, had a significant impact on our results. In the future, large sample size and long duration multicenter studies, with well-matched population including diabetes duration, may provide more reliable results. Moreover, further studies are needed to evaluate the effects of ezetimibe on insulin sensitivity, oxidative stress, and endothelial function by identifying more diverse biomarkers.
- In conclusion, although rosuvastatin/ezetimibe combination therapy had a greater LDL-C reducing effect than rosuvastatin monotherapy, it had no additional effects on insulin sensitivity and vascular inflammatory response. However, considering that insulin resistance and PRDX4 were improved when LDL-C level was significantly reduced in the combination therapy group with a short duration of diabetes and low prevalence of hypertension, further studies targeting patients without hypertension and with a short duration of diabetes might be needed to confirm the effect of ezetimibe on insulin sensitivity, oxidative stress, and vascular inflammation.
DISCUSSION
SUPPLEMENTARY MATERIALS
Supplementary Table 1.
Supplementary Table 2.
Supplementary Fig. 1.
Supplementary Fig. 2.
-
CONFLICTS OF INTEREST
Hyon-Seung Yi has been associate editor of the Diabetes & Metabolism Journal since 2022. He was not involved in the review process of this article. Otherwise, there was no conflict of interest.
-
AUTHOR CONTRIBUTIONS
Conception or design: J.H.H., K.H.J., B.J.K., H.J.K.
Acquisition, analysis, or interpretation of data: J.H.H., J.C.L., O.S.K., S.C., J.M.K., Y.E.K., H.S.Y., J.H.L.
Drafting the work or revising: J.H.H., K.H.J., H.J.K., B.J.K.
Final approval of the manuscript: J.H.H., K.H.J., H.J.K.
-
FUNDING
Hyun Jin Kim was supported by research fund of Chungnam National University. Kyong Hye Joung was supported by Yuhan Coporation Research Fund, 2019. The funders had no role in the study design, data collection and analysis, decision to publish or preparation of the manuscript.
NOTES
-
Acknowledgements
- None
| Characteristic | Rosuvastatin 5 mg/day (n=47) | Rosuvastatin 5 mg+Ezetimibe 10 mg/day (n=45) | P valuea |
|---|---|---|---|
| Age, yr | 57.15±11.78 | 55.04±11.73 | 0.393 |
| Male sex | 19 (40.43) | 23 (51.11) | 0.304 |
| Height, cm | 162.91±7.99 | 162.38±9.49 | 0.774 |
| Weight, kg | 69.67±15.14 | 69.37±17.16 | 0.932 |
| BMI, kg/m2 | 26.34±4.99 | 26.08±4.98 | 0.803 |
| DM duration, mo | 75.48±89.73 | 41.84±56.69 | 0.037 |
| HTN | 23 (48.9) | 13 (28.9) | 0.049 |
| LDL-C, mg/dL | 139.13±25.27 | 135.18±22.57 | 0.432 |
| Triglyceride, mg/dL | 175.40±88.67 | 182.33±107.82 | 0.737 |
| HDL-C, mg/dL | 49.64±10.91 | 48.36±14.96 | 0.639 |
| Fasting plasma glucose, mg/dL | 161.85±77.30 | 146.98±52.45 | 0.289 |
| HbA1c, % | 7.18±1.44 | 6.95±1.49 | 0.445 |
| Fasting insulin, mIU/L | 14.95±7.24 | 17.01±11.75 | 0.311 |
| HOMA-IR | 5.87±3.48 | 6.35±5.09 | 0.604 |
| HOMA-β | 84.34±85.50 | 91.05±75.32 | 0.693 |
| CPK, U/L | 93.47±63.54 | 101.93±46.90 | 0.471 |
| AST, U/L | 20.07±5.86 | 20.47±7.80 | 0.782 |
| ALT, U/L | 22.85±11.91 | 23.64±18.26 | 0.805 |
| sICAM-1, ng/mL | 138.00±50.09 | 133.49±56.39 | 0.685 |
| PRDX4, pg/mL | 2,907.65±2,758.11 | 2,524.10±2,764.72 | 0.585 |
Values are presented as mean±standard deviation or number (%).
BMI, body mass index; DM, diabetes mellitus; HTN, hypertension; LDL-C, low density lipoprotein cholesterol; HDL-C, high density lipoprotein cholesterol; HbA1c, glycosylated hemoglobin; HOMA-IR, homeostasis model assessment of insulin resistance; HOMA-β, homeostasis model assessment of β-cell function; CPK, creatine phosphokinase; AST, aspartate aminotransferase; ALT, alanine aminotransferase; sICAM-1, soluble intercellular adhesion molecule-1; PRDX4, peroxiredoxin-4.
a P valve from Student’s t-test and chi-square test between rosuvastatin group and rosuvastatin/ezetimibe group.
| Variable |
Rosuvastatin 5 mg/day (n=47) |
Rosuvastatin 5 mg+Ezetimibe 10 mg/day (n=45) |
||||
|---|---|---|---|---|---|---|
| Before | After | P valuea | Before | After | P valuea | |
| LDL-C, mg/dL | 139.13±25.27 | 91.53±30.06 | <0.001 | 135.18±22.57 | 65.80±21.80 | <0.001 |
| Triglyceride, mg/dL | 175.40±88.67 | 135.38±62.55 | <0.001 | 182.33±107.82 | 132.56±74.37 | 0.001 |
| HDL-C, mg/dL | 49.64±10.92 | 51.04±11.55 | 0.184 | 48.36±14.96 | 49.33±14.33 | 0.421 |
| Fasting plasma glucose, mg/dL | 161.85±77.30 | 141.62±40.78 | 0.116 | 146.98±52.45 | 141.52±40.54 | 0.447 |
| HbA1c, % | 7.18±1.44 | 6.92±1.01 | 0.152 | 6.95±1.49 | 7.00±1.09 | 0.715 |
| Insulin, mIU/L | 14.95±7.24 | 13.05±12.32 | 0.186 | 17.01±11.75 | 10.79±3.36 | <0.001 |
| HOMA-IR | 5.87±3.48 | 5.14±7.65 | 0.473 | 6.35±5.09 | 3.86±1.93 | 0.002 |
| HOMA-β | 84.34±85.50 | 65.00±37.57 | 0.138 | 91.05±75.32 | 63.65±38.47 | 0.005 |
| sICAM-1, ng/mL | 138.01±50.09 | 157.67±59.62 | 0.003 | 133.49±56.39 | 166.03±97.68 | 0.001 |
| PRDX4, pg/mL | 2,907.65±2,758.11 | 3,508.60±3,130.87 | 0.324 | 2,524.10±2,764.72 | 4,826.22±4,707.62 | 0.007 |
Values are presented as mean±standard deviation.
LDL-C, low density lipoprotein cholesterol; HDL-C, high density lipoprotein cholesterol; HbA1c, glycosylated hemoglobin; HOMA-IR, homeostasis model assessment of insulin resistance; HOMA-β, homeostasis model assessment of β-cell function; sICAM-1, soluble intercellular adhesion molecule-1; PRDX4, peroxiredoxin-4.
a P valve from paired samples t-test between before and after treatment in each group.
| Variable | Reduction of LDL-C level | Change | P valuea | P valueb |
|---|---|---|---|---|
| Total (n=91) | <50% (n=55) | –0.54±6.55 | 0.544 | |
| ≥50% (n=36) | –3.19±5.27 | 0.001 | ||
| Rosuvastatin 5 mg/day (n=47) | <50% (n=38) | –0.27±7.44 | 0.826 | 0.975 |
| ≥50% (n=9) | –2.74±4.55 | 0.086 | ||
| Rosuvastatin 5 mg+Ezetimibe 10 mg/day (n=45) | <50% (n=17) | –1.15±4.00 | 0.149 | |
| ≥50% (n=27) | –3.33±5.56 | 0.001 |
Values are presented as mean±standard deviation.
HOMA-IR, homeostasis model assessment of insulin resistance; LDL-C, low density lipoprotein cholesterol.
a P valve from Wilcoxon signed-rank test between before and after treatment in each group,
b P valve from analysis of covariance (ANCOVA) after adjusted diabetes mellitus duration (month) and hypertension by group (rosuvastatin/rosuvastatin+ezemitibe) and reduction of LDL-C level (<50%/≥50%).
| Reduction of LDL-C level | Change | P valuea | P valueb | |
|---|---|---|---|---|
| Total (n=91) | <50% (n=55) | 706.10±3,193.38 | 0.090 | |
| ≥50% (n=36) | 2,602.97±4,946.42 | 0.004 | ||
| Rosuvastatin 5 mg/day (n=47) | <50% (n=38) | 677.35±3,478.81 | 0.189 | 0.119 |
| ≥50% (n=9) | 360.81±2,445.98 | 1.000 | ||
| Rosuvastatin 5 mg+Ezetimibe 10 mg/day (n=45) | <50% (n=17) | 751.27±2,811.07 | 0.272 | |
| ≥50% (n=27) | 3,387.72±5,393.65 | 0.002 |
Values are presented as mean±standard deviation.
PRDX4, peroxiredoxin 4; LDL-C, low density lipoprotein cholesterol.
a P valve from Wilcoxon signed-rank test between before and after treatment in each group,
b P valve from analysis of covariance (ANCOVA) after adjusted diabetes mellitus duration (month) and hypertension by group (rosuvastatin/rosuvastatin+ezemitibe) and reduction of LDL-C level (<50%/≥50%).
- 1. Lontchi-Yimagou E, Sobngwi E, Matsha TE, Kengne AP. Diabetes mellitus and inflammation. Curr Diab Rep 2013;13:435-44.ArticlePubMedPDF
- 2. Wellen KE, Hotamisligil GS. Inflammation, stress, and diabetes. J Clin Invest 2005;115:1111-9.ArticlePubMedPMC
- 3. Yun JS, Ko SH, Kim JH, Moon KW, Park YM, Yoo KD, et al. Diabetic retinopathy and endothelial dysfunction in patients with type 2 diabetes mellitus. Diabetes Metab J 2013;37:262-9.PubMedPMC
- 4. Tabit CE, Chung WB, Hamburg NM, Vita JA. Endothelial dysfunction in diabetes mellitus: molecular mechanisms and clinical implications. Rev Endocr Metab Disord 2010;11:61-74.ArticlePubMedPMCPDF
- 5. Stone NJ, Robinson JG, Lichtenstein AH, Bairey Merz CN, Blum CB, Eckel RH, et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2014;63(25 Pt B):2889-934.PubMed
- 6. Rhee EJ, Kim HC, Kim JH, Lee EY, Kim BJ, Kim EM, et al. 2018 Guidelines for the management of dyslipidemia in Korea. J Lipid Atheroscler 2019;8:78-131.ArticlePubMedPMCPDF
- 7. Hong N, Lee YH, Tsujita K, Gonzalez JA, Kramer CM, Kovarnik T, et al. Comparison of the effects of ezetimibe-statin combination therapy on major adverse cardiovascular events in patients with and without diabetes: a meta-analysis. Endocrinol Metab (Seoul) 2018;33:219-27.ArticlePubMedPMCPDF
- 8. Cannon CP, Blazing MA, Giugliano RP, McCagg A, White JA, Theroux P, et al. Ezetimibe added to statin therapy after acute coronary syndromes. N Engl J Med 2015;372:2387-97.PubMed
- 9. Rajpathak SN, Kumbhani DJ, Crandall J, Barzilai N, Alderman M, Ridker PM. Statin therapy and risk of developing type 2 diabetes: a meta-analysis. Diabetes Care 2009;32:1924-9.ArticlePubMedPMCPDF
- 10. Kater AL, Batista MC, Ferreira SR. Synergistic effect of simvastatin and ezetimibe on lipid and pro-inflammatory profiles in pre-diabetic subjects. Diabetol Metab Syndr 2010;2:34.ArticlePubMedPMCPDF
- 11. Sirtori CR. The pharmacology of statins. Pharmacol Res 2014;Oct;88:3-11.ArticlePubMed
- 12. Wilson PW, Polonsky TS, Miedema MD, Khera A, Kosinski AS, Kuvin JT. Systematic review for the 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. Circulation 2019;139:e1144-61.PubMed
- 13. Hadi HA, Carr CS, Al Suwaidi J. Endothelial dysfunction: cardiovascular risk factors, therapy, and outcome. Vasc Health Risk Manag 2005;1:183-98.PubMedPMC
- 14. Favero G, Paganelli C, Buffoli B, Rodella LF, Rezzani R. Endothelium and its alterations in cardiovascular diseases: life style intervention. Biomed Res Int 2014;2014:801896.ArticlePubMedPMCPDF
- 15. Forstermann U, Munzel T. Endothelial nitric oxide synthase in vascular disease: from marvel to menace. Circulation 2006;113:1708-14.ArticlePubMed
- 16. Strey CH, Young JM, Lainchbury JH, Frampton CM, Nicholls MG, Richards AM, et al. Short-term statin treatment improves endothelial function and neurohormonal imbalance in normocholesterolaemic patients with non-ischaemic heart failure. Heart 2006;92:1603-9.ArticlePubMedPMC
- 17. Landmesser U, Bahlmann F, Mueller M, Spiekermann S, Kirchhoff N, Schulz S, et al. Simvastatin versus ezetimibe: pleiotropic and lipid-lowering effects on endothelial function in humans. Circulation 2005;111:2356-63.ArticlePubMed
- 18. Chia PY, Teo A, Yeo TW. Overview of the assessment of endothelial function in humans. Front Med (Lausanne) 2020;7:542567.ArticlePubMedPMC
- 19. Sena CM, Pereira AM, Seica R. Endothelial dysfunction: a major mediator of diabetic vascular disease. Biochim Biophys Acta 2013;1832:2216-31.ArticlePubMed
- 20. Abbasi A, Corpeleijn E, Postmus D, Gansevoort RT, de Jong PE, Gans RO, et al. Peroxiredoxin 4, a novel circulating biomarker for oxidative stress and the risk of incident cardiovascular disease and all-cause mortality. J Am Heart Assoc 2012;1:e002956.ArticlePubMedPMC
- 21. El Eter E, Al Masri A, Habib S, Al Zamil H, Al Hersi A, Al Hussein F, et al. Novel links among peroxiredoxins, endothelial dysfunction, and severity of atherosclerosis in type 2 diabetic patients with peripheral atherosclerotic disease. Cell Stress Chaperones 2014;19:173-81.ArticlePubMedPMCPDF
- 22. Guo X, Yamada S, Tanimoto A, Ding Y, Wang KY, Shimajiri S, et al. Overexpression of peroxiredoxin 4 attenuates atherosclerosis in apolipoprotein E knockout mice. Antioxid Redox Signal 2012;17:1362-75.ArticlePubMedPMC
- 23. Abbasi A, Corpeleijn E, Gansevoort RT, Gans RO, Struck J, Schulte J, et al. Circulating peroxiredoxin 4 and type 2 diabetes risk: the Prevention of Renal and Vascular Endstage Disease (PREVEND) study. Diabetologia 2014;57:1842-9.ArticlePubMedPMCPDF
- 24. Al-Masri AA, El Eter E, Tayel S, Zamil H. Differential associations of circulating peroxiredoxins levels with indicators of glycemic control in type 2 diabetes mellitus. Eur Rev Med Pharmacol Sci 2014;18:710-6.PubMed
- 25. Ding Y, Yamada S, Wang KY, Shimajiri S, Guo X, Tanimoto A, et al. Overexpression of peroxiredoxin 4 protects against high-dose streptozotocin-induced diabetes by suppressing oxidative stress and cytokines in transgenic mice. Antioxid Redox Signal 2010;13:1477-90.ArticlePubMed
- 26. Nabeshima A, Yamada S, Guo X, Tanimoto A, Wang KY, Shimajiri S, et al. Peroxiredoxin 4 protects against nonalcoholic steatohepatitis and type 2 diabetes in a nongenetic mouse model. Antioxid Redox Signal 2013;19:1983-98.ArticlePubMedPMC
- 27. Vivoli A, Ghislain J, Filali-Mouhim A, Angeles ZE, Castell AL, Sladek R, et al. Single-cell RNA sequencing reveals a role for reactive oxygen species and peroxiredoxins in fatty acid-induced rat b-cell proliferation. Diabetes 2023;72:45-58.PubMed
- 28. Gross MD, Bielinski SJ, Suarez-Lopez JR, Reiner AP, Bailey K, Thyagarajan B, et al. Circulating soluble intercellular adhesion molecule 1 and subclinical atherosclerosis: the Coronary Artery Risk Development in Young Adults Study. Clin Chem 2012;58:411-20.ArticlePubMedPMCPDF
- 29. Luc G, Arveiler D, Evans A, Amouyel P, Ferrieres J, Bard JM, et al. Circulating soluble adhesion molecules ICAM-1 and VCAM-1 and incident coronary heart disease: the PRIME Study. Atherosclerosis 2003;170:169-76.ArticlePubMed
- 30. Zonneveld R, Martinelli R, Shapiro NI, Kuijpers TW, Plotz FB, Carman CV. Soluble adhesion molecules as markers for sepsis and the potential pathophysiological discrepancy in neonates, children and adults. Crit Care 2014;18:204.ArticlePubMedPMCPDF
- 31. Lawson C, Wolf S. ICAM-1 signaling in endothelial cells. Pharmacol Rep 2009;61:22-32.ArticlePubMed
- 32. Gho YS, Kleinman HK, Sosne G. Angiogenic activity of human soluble intercellular adhesion molecule-1. Cancer Res 1999;59:5128-32.PubMed
- 33. Kevil CG, Orr AW, Langston W, Mickett K, Murphy-Ullrich J, Patel RP, et al. Intercellular adhesion molecule-1 (ICAM-1) regulates endothelial cell motility through a nitric oxide-dependent pathway. J Biol Chem 2004;279:19230-8.ArticlePubMed
- 34. Rieckmann P, Michel U, Albrecht M, Bruck W, Wockel L, Felgenhauer K. Soluble forms of intercellular adhesion molecule-1 (ICAM-1) block lymphocyte attachment to cerebral endothelial cells. J Neuroimmunol 1995;60:9-15.ArticlePubMed
- 35. Kim JY, Kim DH, Kim JH, Lee D, Jeon HB, Kwon SJ, et al. Soluble intracellular adhesion molecule-1 secreted by human umbilical cord blood-derived mesenchymal stem cell reduces amyloid-b plaques. Cell Death Differ 2012;19:680-91.ArticlePubMedPMCPDF
- 36. Omi H, Okayama N, Shimizu M, Fukutomi T, Imaeda K, Okouchi M, et al. Statins inhibit high glucose-mediated neutrophil-endothelial cell adhesion through decreasing surface expression of endothelial adhesion molecules by stimulating production of endothelial nitric oxide. Microvasc Res 2003;65:118-24.ArticlePubMed
- 37. Chung HK, Lee IK, Kang H, Suh JM, Kim H, Park KC, et al. Statin inhibits interferon-gamma-induced expression of intercellular adhesion molecule-1 (ICAM-1) in vascular endothelial and smooth muscle cells. Exp Mol Med 2002;34:451-61.ArticlePubMedPDF
- 38. Blanco-Colio LM, Martin-Ventura JL, de Teresa E, Farsang C, Gaw A, Gensini G, et al. Elevated ICAM-1 and MCP-1 plasma levels in subjects at high cardiovascular risk are diminished by atorvastatin treatment. Atorvastatin on Inflammatory Markers study: a substudy of Achieve Cholesterol Targets Fast with Atorvastatin Stratified Titration. Am Heart J 2007;153:881-8.ArticlePubMed
- 39. Sadeghi MM, Collinge M, Pardi R, Bender JR. Simvastatin modulates cytokine-mediated endothelial cell adhesion molecule induction: involvement of an inhibitory G protein. J Immunol 2000;165:2712-8.ArticlePubMedPDF
- 40. Bernot D, Benoliel AM, Peiretti F, Lopez S, Bonardo B, Bongrand P, et al. Effect of atorvastatin on adhesive phenotype of human endothelial cells activated by tumor necrosis factor alpha. J Cardiovasc Pharmacol 2003;41:316-24.ArticlePubMed
- 41. Sun C, Zheng W, Liang L, Liu Z, Sun W, Tang R. Ezetimibe improves rosuvastatin effects on inflammation and vascular endothelial function in acute coronary syndrome patients undergoing PCI. J Interv Cardiol 2021;2021:2995602.ArticlePubMedPMCPDF
- 42. Krysiak R, Zmuda W, Okopien B. The effect of ezetimibe, administered alone or in combination with simvastatin, on lymphocyte cytokine release in patients with elevated cholesterol levels. J Intern Med 2012;271:32-42.ArticlePubMed
- 43. Adhyaru BB, Jacobson TA. Safety and efficacy of statin therapy. Nat Rev Cardiol 2018;15:757-69.ArticlePubMedPDF
- 44. Macedo AF, Douglas I, Smeeth L, Forbes H, Ebrahim S. Statins and the risk of type 2 diabetes mellitus: cohort study using the UK clinical practice pesearch datalink. BMC Cardiovasc Disord 2014;14:85.ArticlePubMedPMCPDF
- 45. Preiss D, Seshasai SR, Welsh P, Murphy SA, Ho JE, Waters DD, et al. Risk of incident diabetes with intensive-dose compared with moderate-dose statin therapy: a meta-analysis. JAMA 2011;305:2556-64.ArticlePubMed
- 46. Kain V, Kapadia B, Misra P, Saxena U. Simvastatin may induce insulin resistance through a novel fatty acid mediated cholesterol independent mechanism. Sci Rep 2015;5:13823.ArticlePubMedPMCPDF
- 47. Adachi H, Nakano H, Yamamoto K, Nakata M, Bekki H, Honma T, et al. Ezetimibe ameliorates atherogenic lipids profiles, insulin resistance and hepatocyte growth factor in obese patients with hypercholesterolemia. Lipids Health Dis 2015;14:1.ArticlePubMedPMCPDF
- 48. Cho Y, Kim RH, Park H, Wang HJ, Lee H, Kang ES. Effect of ezetimibe on glucose metabolism and inflammatory markers in adipose tissue. Biomedicines 2020;8:512.ArticlePubMedPMC
REFERENCES
Figure & Data
References
Citations
- Combining Ezetimibe and Rosuvastatin: Impacts on Insulin Sensitivity and Vascular Inflammation in Patients with Type 2 Diabetes Mellitus
Eun Roh
Diabetes & Metabolism Journal.2024; 48(1): 55. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite