
- Current
- Browse
- Collections
-
For contributors
- For Authors
- Instructions to authors
- Article processing charge
- e-submission
- For Reviewers
- Instructions for reviewers
- How to become a reviewer
- Best reviewers
- For Readers
- Readership
- Subscription
- Permission guidelines
- About
- Editorial policy
Articles
- Page Path
- HOME > Diabetes Metab J > Volume 46(5); 2022 > Article
-
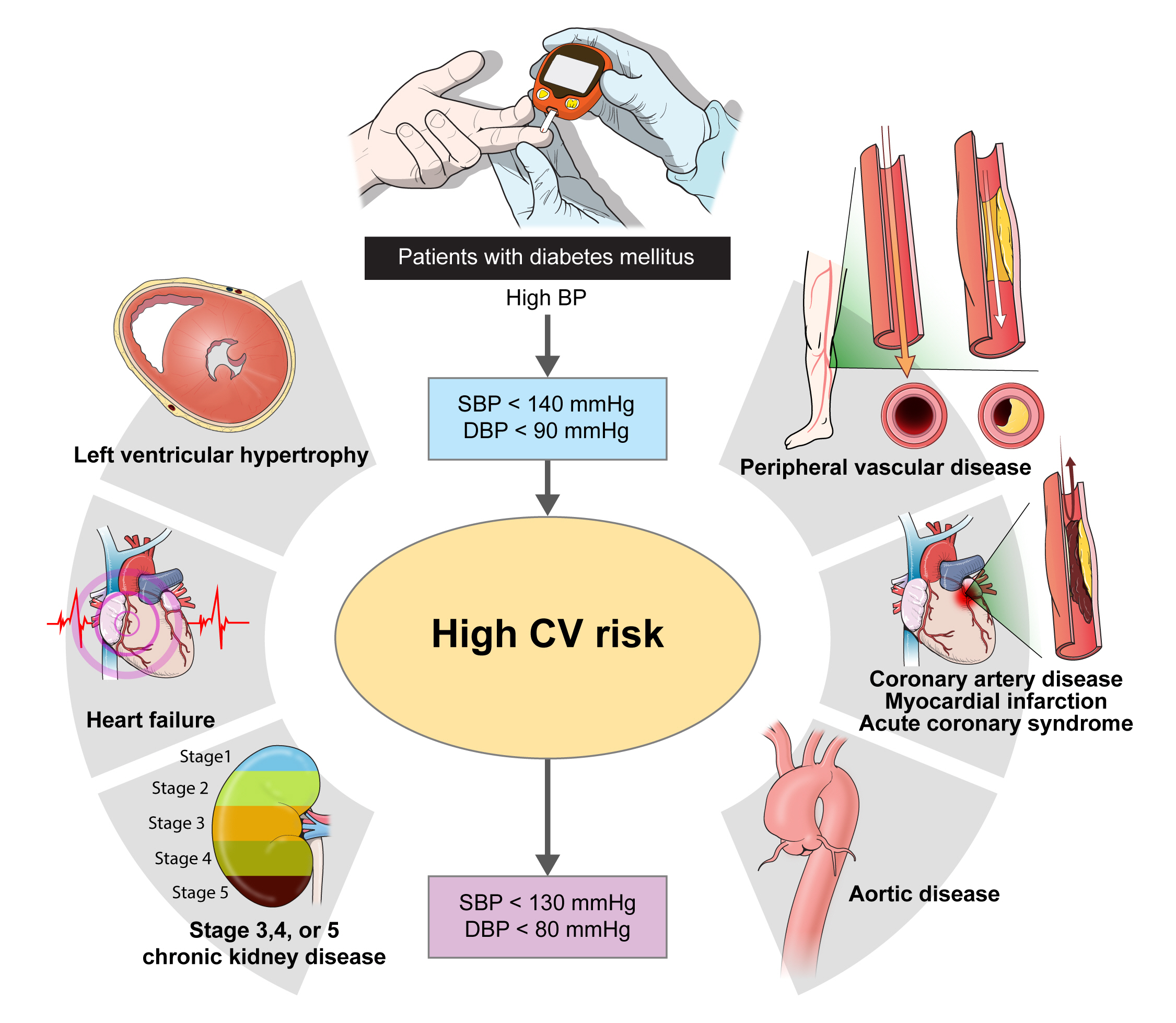
ReviewPathophysiology Blood Pressure Target in Type 2 Diabetes Mellitus
-
Hyun-Jin Kim1
 , Kwang-il Kim2, on Behalf of the Policy Committee of Korean Society of Hypertension
, Kwang-il Kim2, on Behalf of the Policy Committee of Korean Society of Hypertension -
Diabetes & Metabolism Journal 2022;46(5):667-674.
DOI: https://doi.org/10.4093/dmj.2022.0215
Published online: September 19, 2022
1Division of Cardiology, Department of Internal Medicine, Hanyang University College of Medicine, Seoul, Korea
2Division of Geriatrics, Department of Internal Medicine, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea
- Corresponding author: Kwang-il Kim https://orcid.org/0000-0002-6658-047X Division of Geriatrics, Department of Internal Medicine, Seoul National University Bundang Hospital, Seoul National University College of Medicine, 82 Gumi-ro 173beongil, Bundang-gu, Seongnam 13620, Korea E-mail: kikim907@snu.ac.kr
• Received: June 25, 2022 • Accepted: July 26, 2022
Copyright © 2022 Korean Diabetes Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
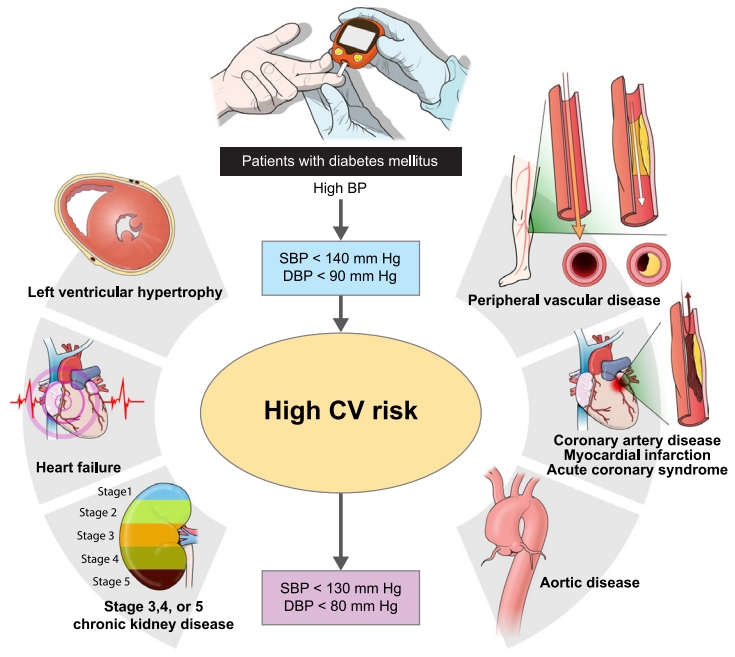
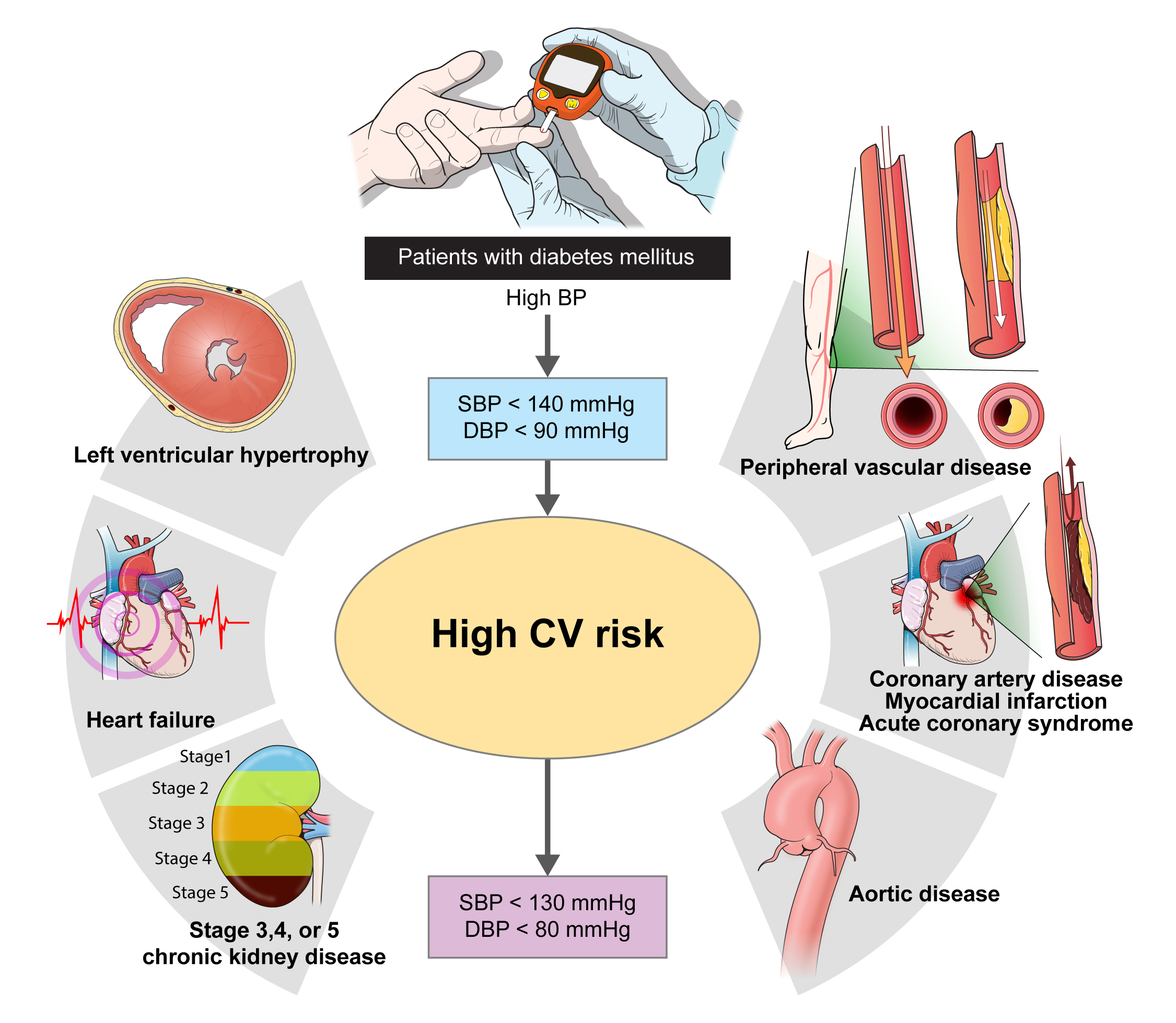
Figure & Data
References
Citations
Citations to this article as recorded by 
- Recent evidence on target blood pressure in patients with hypertension
Hack-Lyoung Kim
Cardiovascular Prevention and Pharmacotherapy.2024; 6(1): 17. CrossRef - Using Generative AI to Improve the Performance and Interpretability of Rule-Based Diagnosis of Type 2 Diabetes Mellitus
Leon Kopitar, Iztok Fister, Gregor Stiglic
Information.2024; 15(3): 162. CrossRef - Additive interaction of family medical history of diabetes with hypertension on the diagnosis of diabetes among older adults in India: longitudinal ageing study in India
Waquar Ahmed
BMC Public Health.2024;[Epub] CrossRef - Emerging roles of interferon-stimulated gene-15 in age-related telomere attrition, the DNA damage response, and cardiovascular disease
María González-Amor, Beatriz Dorado, Vicente Andrés
Frontiers in Cell and Developmental Biology.2023;[Epub] CrossRef - Effects of Diabetes and Voluntary Exercise on IgA Concentration and Polymeric Immunoglobulin Receptor Expression in the Submandibular Gland of Rats
Jaebum Park, Yuko Yamamoto, Kouki Hidaka, Satoko Wada-Takahashi, Shun-suke Takahashi, Toshiya Morozumi, Nobuhisa Kubota, Makiko Saita, Juri Saruta, Wakako Sakaguchi, Masahiro To, Tomoko Shimizu, Yuko Mikuni-Takagaki, Keiichi Tsukinoki
Medicina.2023; 59(4): 789. CrossRef - A diabetes update
Zachary Bloomgarden
Journal of Diabetes.2023; 15(7): 542. CrossRef - CARDIOPROTECTIVE AND METABOLIC EFFECTS OF ANTIHYPERTENSIVE THERAPY IN PATIENTS WITH SUCH COMORBIDITIES AS ARTERIAL HYPERTENSION, TYPE 2 DIABETES MELLITUS, AND OBESITY
I. P. Dunaieva, N. O. Kravchun, І. A. Ilchenko
Bulletin of Problems Biology and Medicine.2023; 1(2): 211. CrossRef - Hypertensive Heart Failure
Filippos Triposkiadis, Pantelis Sarafidis, Alexandros Briasoulis, Dimitrios E. Magouliotis, Thanos Athanasiou, John Skoularigis, Andrew Xanthopoulos
Journal of Clinical Medicine.2023; 12(15): 5090. CrossRef - 2023 Clinical Practice Guidelines for Diabetes
Min Kyong Moon
The Journal of Korean Diabetes.2023; 24(3): 120. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite- Figure
-

- Related articles
-
- Change Profiles and Functional Targets of MicroRNAs in Type 2 Diabetes Mellitus Patients with Obesity
- Intensified Multifactorial Intervention in Patients with Type 2 Diabetes Mellitus
- Not Control but Conquest: Strategies for the Remission of Type 2 Diabetes Mellitus
- Real-World Analysis of Therapeutic Outcome in Type 1 Diabetes Mellitus at a Tertiary Care Center



