The Correlation and Accuracy of Glucose Levels between Interstitial Fluid and Venous Plasma by Continuous Glucose Monitoring System
Article information
Abstract
Background
Clinical experience with the continuous glucose monitoring systems (CGMS) is limited in Korea. The objective of this study is to evaluate the accuracy of the CGMS and the correlation between interstitial fluid and venous plasma glucose level in Korean healthy male subjects.
Methods
Thirty-two subjects were served with glucose solution contained same amount of test food's carbohydrate and test foods after separate overnight fasts. CGMS was performed over 3 days during hopitalization for each subjects. Venous plasma glucose measurements were carried out during 4 hours (0, 0.25, 0.5, 0.75, 1, 2, 4 hours) just before and after glucose solution and test food load. The performance of the CGMS was evaluated by comparing its readings to those obtained at the same time by the hexokinase method using the auto biochemistry machine (Hitachi 7600-110). Also, correlations between glucose recorded with CGMS and venous plasma glucose value were examined.
Results
CGMS slightly underestimated the glucose value as compared with the venous plasma glucose level (16.3 ± 22.2 mg/dL). Correlation between CGMS and venous plasma glucose values throughout sensor lifetime is 0.73 (regression analysis: slope = 1.08, intercept = 8.38 mg/dL). Sensor sensitivity can deteriorate over time, with correlations between venous blood glucose and CGMS values dropping from 0.77 during 1st day to 0.65 during 2nd and 3rd day.
Conclusion
The accuracy of data provided by CGMS may be less than expected. CGMS sensor sensitivity is decreased with the passage of time. But, from this study, CGMS can be used for glucose variability tendency monitoring conveniently to the Korean.
INTRODUCTION
For the past 15 years, the use of short acting insulin and long-acting insulin, insulin pump development, and regular self-monitoring of blood glucose have played positive roles in reaching the desired level of glycated hemoglobin in diabetics. However, the fear of patients who still have hypoglycemia is one complicated element of blood glucose level regulation that cannot be overlooked [1]. In other words, normal blood glucose regulation is becoming the limiting factor in hypoglycemia in patients with diabetes [2].
In this sense, compared to the usual method of checking blood glucose levels 3 to 4 times per day, a continuous glucose monitoring system (CGMS), a system that provides relatively accurate information regarding blood glucose patterns, duration, variations, maximum and minimum levels, allows patients to be aware of their blood glucose levels at all times. The continuous measurement throughout a single day or 2 to 3 days provides insight to the patterns of blood glucose levels and gives warnings to recognize sudden low or high blood glucose levels and helps in preventing fatal episodes [2-4]. Furthermore, the CGMS is easy to use for patients. A great benefit is insertion and wearing the equipment involves minimal discomfort.
Using CGMS, when implemented previous prospective studies were examined, the goal glycated hemoglobin level was reached more quickly than before CGMS introduction [2,5-10], and complications were prevented. However, this benefit was only reported in one study. Precisely assessed studies on blood glucose regulation were very uncommon [1]. Looking at the situation in South Korea, only 17% of diabetics measure their blood glucose regularly at medical institutions [11]. Recently, raised interest or initiation of maintenance of diabetes has been occurring. Owing to the increased education of patients and medical professionals about diabetes, it is estimated that more patients are measuring their blood glucose regularly at medical institutions. In addition, in some diabetes centers, using CGMS, diurnal changes in interstitial fluid levels were measured. However limitations include: the increase in elderly, eastern traditions, difficulty mounting a new medical device, financial problems, and domestic problems which make it difficult for patients to use. Therefore, clinical experience for the use of CGMS is limited, so the reality is that various experiences and clinical applications are very difficult.
In this study, the authors evaluated the accuracy of CGMS and the relationship between the interstitial fluid and venous blood glucose level in healthy adults. Additionally, we compared differences of the blood glucose patterns according to the experimental diets, with the use and confirmation of flaws in the CGMS.
METHODS
Subjects
The subjects selected for this clinical trial were healthy Korean volunteers who satisfied all the selection criteria: 1) male aged 20 to 40 years, 2) body weight is 50 kg or more and whithin 30% of their ideal body weight {ideal body weight = (height [cm] - 100) × 0.9}, and 3) agreement of study enrollment. Informed consent was obtained from each subject. Exclusion criteria include the following: 1) individuals with illness of the liver, kidneys, nervous system, respiratory, endocrine, blood, tumors, mental illness, or a history of cardiovascular disease, 2) individuals with a history of gastrointestinal diseases (e.g., Crohn's disease) that can influence nutrient absorption, gastrointestinal surgery (excluding simple appendectomy or hernia surgery), 3) blood test findings aspartate transaminase (AST)/alanine transaminase (ALT) > 1.25 times the upper limit of the normal range, 4) individuals having a systolic blood pressure under 100 mm Hg and over 150 mm Hg, or individuals having a diastolic blood pressure under 65 mm Hg and over 95 mm Hg, 5) individuals with hypersensitivity to experimental diets or having a medical history of clinical allergic reactions, 6) individuals who took prescribed drugs or eastern medicines two weeks before the beginning of the study, or individuals who took over-the-counter (OTC) medication or vitamin supplements (However, candidates may be able to participate at the discretion of the examinees), 7) individuals who have participated in other clinical trials two months prior to the beginning of this study, 8) individuals who have donated blood up to one month prior to the study, or individuals who have donated plasma within the two weeks prior to the beginning of the study, 9) individuals who drink 21 drinks/week or individuals who cannot abstain from alcohol consumption or more during clinical trials, for any other reason that the examiner thought that participants' participation would be irrelevant. A 4 × 4 cross-examination was carried out on a total of 32 patients. Statistical administration occurred in groups of eight.
Methods
The study was performed in open-label, 4-treatment, 4-order, 4-time frame crossover design (Table 1); appropriate candidates were selected through an interview, physical exam, and disease screening 4 weeks (D-28 to D-1) prior to the clinical trial and a random assignment was carried out one day prior (D-1) to the first day of the study.
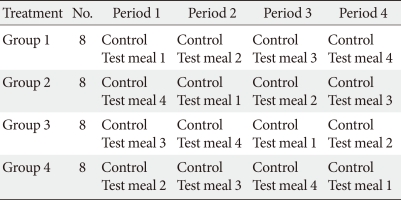
Open label, 4-treatment, 4-sequence, 4-perioid crossover study
For the first period of clinical trial (period 1), study subjects were admitted to the Clinical Trial Center for Functional Foods in Chonbuk National University Hospital by 7:00 PM on the 1st day. The subjects fasted with the exception of drinking water after the initial dinner that was provided by the center. At approximately 9:00 AM on the 2nd day, all the subjects who had been fasting consumed a control diet based on their randomly assigned group. A control diet was composed of the same amount of glucose with the carbohydrate content in corresponding test meal. Caloric and nutritional composition of each test meal is as follows: Korean 1 (Bibimbap) 588 kcal (carbohydrates 86.1 g, protein 24.6 g, and fat 16.53 g), Korean 2 (Kimbap) 598.7 kcal (carbohydrates 83.1 g, protein 27.6 g, and fat 17.14 g), Western 1 (pork cutlet) 602.2 kcal (carbohydrates 66.4 g, protein 28.4 g, and fat 23.2 g), Western 2 (hamburger) 586 kcal (carbohydrates 63.2 g, protein 30.6 g, and fat 23.2 g). The ingredients of the test meal were produced in the same region to ensure the consistency of the quality. They were also stored for a minimal amount of time within the expiration date. The cooking methods were also kept consistent by establishing a standard method for meal preparation regarding intensity of the cooking fire and cooking time. This standard was used for each preparation. The study subjects consumed the provided control diet within 2 minutes.
They were prohibited from consuming anything besides water after dinner on the 2nd day and provided the test meal on 9 AM in the next morning according to the group. The menu of each test meal was designed to include representative dishes for common types of cuisine: Korean 1 (Bibimbap), Korean 2 (Kimbap), Western 1 (pork cutlet), and Western 2 (hamburger) (the study subjects were instructed to consume the test meal within 15 minutes). After the end of the period 1, all the subjects were discharged and 6-day's resting period was followed by the period 2. For the period 2, subjects were admitted again and provied the control diet and test meal according to the same method in period 1. Period 3 and 4 were carried out in sequence with intervening 6-day's resting period.
The self-monitoring of blood glucose unit used for continuous blood glucose measurement needed for the study was a CGMS model from Medtronic (Northridge, CA, USA). Data was collected by inserting the blood sugar sensor under the skin using plasma calibration with an auto biochemistry machine (Hitachi 7600-11; Hitachi, Tokyo, Japan) which was measured and analyzed using the hexokinase method. For this process, blood glucose measurements were taken 4 times a day and inputted into the CGMS. Continuous blood glucose measurements were taken on day one (and on the 2nd, 8th, 9th, 15th, 16th, 22nd, 23rd day) between hour 0 (before the meal) and hour 4 every 5 minutes. Blood samples for measurement of blood glucose and insulin was taken on day one (and 2nd, 8th, 9th, 15th, 16th, 22nd, 23rd day) at hour 0 (before the meal), hour 0.25, hour 0.5, hour 0.75, hour 1, hour 2, and hour 4. A blood sample of 1 mL was taken from brachial veins without the use of a catheter due to the characteristics of the research methods.
Statistical analysis
Statistical analysis was performed using the following methods using a significance level of 0.05 (average ± standard deviation) with SPSS (SPSS Inc., Chicago, IL, USA), SAS (SAS Institute, Cary, NC, USA) and/or S-plus (TIBCO, Palo Alto, CA, USA) statistical software. Demographic statistical analysis of participants of the clinical trial was carried out to ensure random sampling. Participant age, height, body weight, and alcohol and caffeine consumption information was collected for demographic statistical analysis.
Analysis of variance (ANOVA) was used for continuous variables, and Fisher's exact test was used for categorical variables. The correlation and significance between the glucose level measured from the reference sample of venous blood, and that from CGMS were analyzed using linear regression analysis.
Each measured level was marked as a distribution point using a Clarke error grid analysis; areas A and B are clinically acceptable regions and areas C, D, and E are regions which are considered unsafe or unacceptable.
RESULTS
Clinical characteristics of the participants
Thirty-two adult males were randomly assigned to participate in this study. Mean age was 23.9 ± 1.5 years, mean height was 173.9 ± 5.3 cm, mean body weight was 64.8 ± 6.3 kg, fasting plasma glucose/insulin was 88.3 ± 5.6 mg/dL/3.6 ± 1.7 uU/mL, respectively, blood urea nitrogen (BUN)/Creatinine was 13.7 ± 2.8 mg/dL/0.97 ± 0.1 mg/dL, AST/ALT was 20.3 ± 8.6 IU/L/17.9 ± 13.4 IU/L, and the lipid profile (cholesterol/triglyceride/HDL/LDL) was 159.6 ± 26.6 mg/dL/103.3 ± 40.9 mg/dL/51.9 ± 8.0 mg/dL/96.4 ± 26.9 mg/dL, respectively. The mean value for body mass index was 20.8 ± 1.5 (Table 2). Personal medical history, physical examination, and baseline blood examination showed no associated diseases.
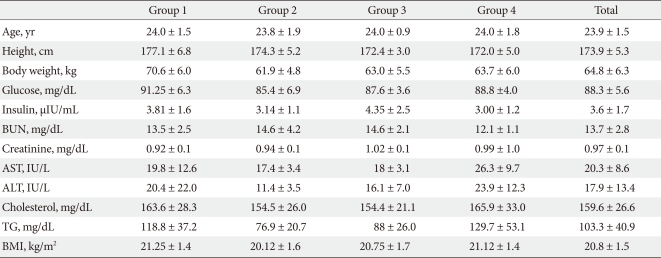
Baseline characteristics of the patients
The comparison of the glucose profiles from CGMS and venous plasma glucose values of each group
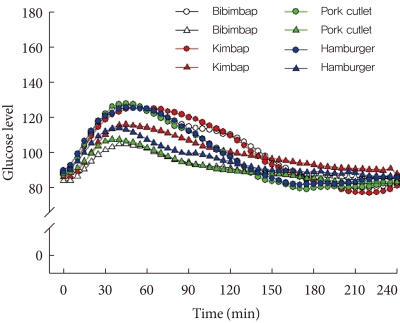
Fig. 1 shows the glucose profiles from CGMS and venous plasma glucose for each group, and the patterns and relationship between them. Values of postprandial venous plasma glucose levels of all groups were between 130 to 190 mg/dL. Plasma glucose 4 hours after eating was measured to be 60 to 90 mg/dL. The highest blood glucose measurement was 171 mg/dL, and the lowest blood glucose measurement was 71 mg/dL. The CGMS showed that peak postprandial glucose level was 120 to 140 mg/dL which was lower than that from plasma and the time to the peak glucose level was 45 to 75 minutes which was longer than 30 to 60minutes in plasma value. With the CGMS, the highest value was measured to be 131 mg/dL, and the lowest value was measured to be 71.6 mg/dL. The overall distribution pattern of intravenous glucose and CGMS values were similar in each group.
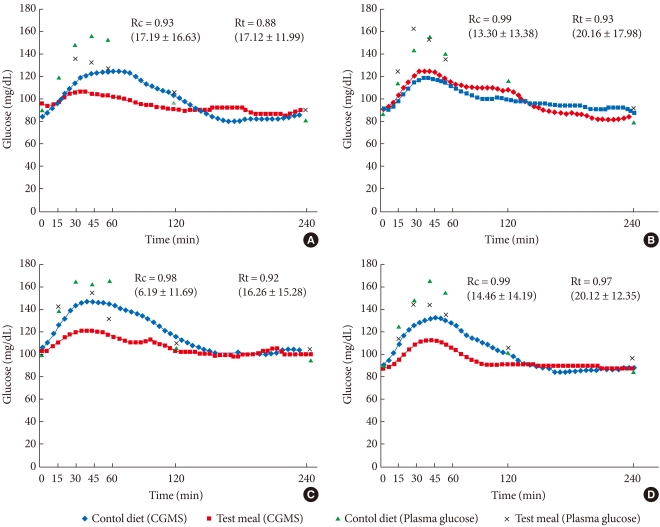
(A) group 1, (B) group 2, (C) group 3, and (D) group 4. The relation between continuous glucose monitoring system (CGMS) and venous blood glucose levels according to the subject groups. CGMS slightly underestimated the glucose value as compared with the venous plasma glucose level. "Time-lag" is observed. However, between each group were similar to venous glucose and CGMS aspects. Data was shown as mean ± standard deviation. Rc: Control , Rt: Test meal (R: Glucose from CGMS vs. Blood plasma glucose).
The comparison of the glucose level according to the control diet and test meal
Looking at the CGMS and venous plasma glucose patterns from different types of diets (Fig. 2), the pattern of venous plasma glucose in all control diet and test meal reached approximately 100 to 190 mg/dL 30 to 45 minutes after consumption and then decreased in 60 minutes after meal, and normal fasting glucose level were seen 4 hours after meal. Additionally, the control diet resulted in the highest postprandial blood glucose level, and also the lowest postprandial venous plasma glucose level in all four groups, but it had no statistical significance.
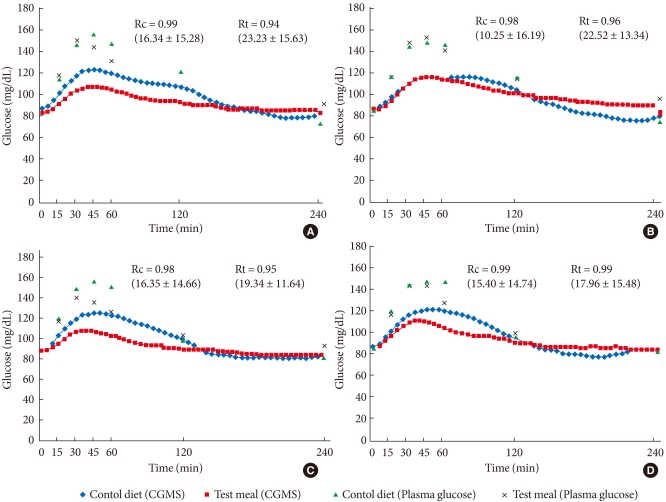
(A) Korean meal 1, (B) Korean meal 2, (C) Western meal 1, and (D) Western meal 2. The relation between continuous glucose monitoring system (CGMS) and venous plasma glucose levels according to the meals. When compared by each diet, venous glucose and CGMS levels showed similar patterns that did not differ significantly. Data was shown as mean ± standard deviation. Rc: Control , Rt: Test meal (R: Glucose from CGMS vs. Blood plasma glucose).
Additionally, glucose value distribution measured with CGMS showed the similar pattern of postprandial increament in plasma glucose level, however, time to peak level was 45 to 60 minutes. Four hours after eating, the glucose level were similar to that from plasma again (Fig. 3). The highest and lowest glucose level in CGMS were also seen in the control diet and there was no significant difference in the value from CGMS and plasma in each group.
The glucose levels measured by continuous glucose monitoring system between controls (O) and treatment (Δ) groups according to the time passage.
The relationship and correlation between the glucose profiles from CGMS and venous plasma glucose measurement values
During the entire experimental period for all of the groups, when comparing the glucose level measured with CGMS and venous plasma glucose level, postprandial blood glucose patterns and even fasting plasma glucose level patterns decreased in a similar fashion. The time lag phenomenon in the peak postprandial glucose level between the CGMS value and plasma glucose were seen in gll group and all kinds of diet. Additionally, the difference between each of the CGMS and venous plasma glucose values for hyperglycemia period (45 to 60 minutes after eating), and hyperglycemia period (0 to 30 minuites after eating and 2 to 4 hours after eating) 34 ± 8.23 mg/dL, and 2.9 ± 4.94 mg/dL respectively, which confirmed that the accuracy in the hyperglycemic period was declining. The value from CGMS was lower than venous plasma glucose in all the time-section (16.3 ± 22.2 mg/dL). The correlation value between CGMS and venous plasma glucose was 0.73 (Fig. 4; regression analysis: slope = 1.08, intercept = 8.38 mg/dL). Additionally, correlation of these values, on the 1st day of clinical trials was 0.77, and on the 2nd day, it decreased to 0.65 (Figs. 5 and 6). These results were analyzed by error grid analysis (n = 1,568). Area A and area B are located at 95.4%, and CGMS's usefulness was confirmed (Fig. 7).
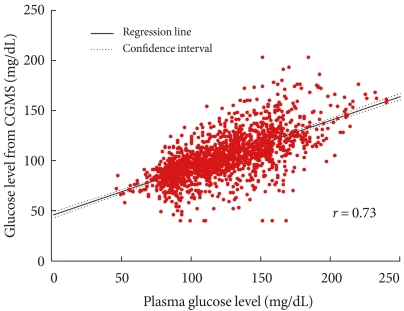
Correlation between continuous glucose monitoring system (CGMS) and venous plasma glucose levels (regression analysis: slope = 1.08, intercept = 8.38 mg/dL).

Correlation between continuous glucose monitoring system (CGMS) and venous plasma glucose levels (1st day, regression analysis: slope = 1.08, intercept = 8.38 mg/dL).

Correlation between continuous glucose monitoring system (CGMS) and venous plasma glucose levels (2nd day, regression analysis: slope = 1.08, intercept = 8.38 mg/dL).
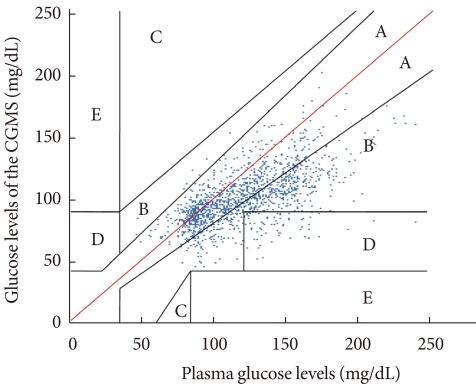
Correlation between continuous glucose monitoring system (CGMS) and venous plasma glucose levels using the Clarke error grid analysis (n = 1,568); 95.4% measures were within zones A and B.
DISCUSSION
One benefit of the CGMS is that it can provide more information on the fluctuations of blood glucose. In other words, when blood glucose cannot be pin pointed, CGMS provides more benefits than intermittent methods of measuring blood glucose [10]. This benefit can greatly reduce the incidence of complications in uncontrolled blood glucose, and patients' concerns are minimized, and it allows for more active blood glucose regulation. However, as previously mentioned, utilizing CGMS to care for patients may not be practical. In reality, clinical experience in utilizing CGMS is minimal in Korea.
Through this clinical trial, authors discovered that the result of CGMS was very similar to the venous plasma glucose level, and the correlation between CGMS and the value of venous plasma glucose level was relatively accurate. These points adequately explained the general benefits of the CGMS. As a result, previous reports regarding the accuracy of the CGMS are considered to be similar [12-16], and it appears that using the CGMS in the future in Korean patients with diabetes can occur without difficulty.
There are reports that state there is no proof that CGMS is better at regulating blood glucose and metabolism when measuring and comparing venous blood glucose levels [17], but there are reports that show the benefits of CGMS in practice in reaching target glycated hemoglobin levels and adjusting it to appropriate levels [1,2,5-10]. Therefore, it is thought that the domestic application of CGMS should be more active, so that research and reporting similar to this can be more active.
However, when this study was compared with the results of the main study that was published prior to this, some were able to confirm the significance level and the decline of the accuracy on the error grid in zones A and B at 98.4% [12] vs. 95.4%. However, there were a relatively small number of subjects and a short follow-up period. A study involving more patients would be required for further explanation.
When the CGMS measured values and venous plasma glucose concentration of each group is compared, no significant difference was observed in the overall changes of blood glucose. Although blood glucose values measured with CGMS was not statistically significant, it showed a lower trend, which in this study; target participants were not patients with chronic diseases including diabetes, but healthy adult male patients. In addition, a comparison with diabetes patients must also be made. CGMS did not show statistically significant differences between implementing control diet and experimental diet for each diet group and intravenous glucose. Also, we think this because this is a study implemented by targeting non-diabetes healthy male subjects. In the future, the importance of the glycemic index and glycemic load of this diet group is studied, but it is thought to be utilizable.
When CGMS results were compared with the venous plasma glucose concentrations, CGMS's time lag was observed. Glucose achieves equilibrium through interstitial fluid in the blood through this, and at this time, it is a physiological process [18]. It is assumed that CGMS measurement values during hypoglycemia or sudden pattern changes may be imprecise [19].
In addition, the sensor's sensitivity decreased over time, and the accuracy decline was observed. These results have been reported in previous CGMS clinical trials [12,13]: bleeding and irritation of the skin between sensors [18], adsorption of tissue around the sensor, localized accumulation of inflamed cells, and fibrous encapsulation are thought to have caused these results [20-22]. Using corticosteroid spray on the sensors for all treatments can reduce these problems [9]. Further clinical trials are required to confirm this.
In conclusion, this study investigated the data obtained from a CGMS and venous plasma glucose level, which was confirmed to have a high correlation. There was no statistical difference observed in the changing patterns in blood glucose from food types and experimental diets, and it was confirmed that there are still problems such as the decrease in time lag and sensor sensitivity. Additionally, it is reported that CGMS was performed in many previous studies involving diabetes patient groups; especially type 1 diabetics, pregnant patients, and special cases such as patients on dialysis. In this clinical trial, healthy adults were used because the accuracy of the correlation between changes in glucose is more credible. However, since it is used as such on diabetes patients, there are limits to the interpretation of the results. Additionally, the number of participants in this study was small. For increased reliability and representation of the clinical trials, more personnel are needed. Others cannot comment on the accuracy of all CGMS's between CGMS machines; and because differences could not be assessed, future studies should include the CGMS used in this study so each machine's correlation and accuracy can be compared. However, through this clinical trial, the authors were able to confirm that CGMS would be very useful in the domestic market to figure out changes in blood glucose and distribution states as levels of blood glucose measured by CGMS were very similar to venous blood. Therefore, continuous research should be conducted so that CGMS can be used as a method to increase the success of reaching target blood glucose level and also to determine appropriate controlling methods for blood glucose.