Multiple Biomarkers Improved Prediction for the Risk of Type 2 Diabetes Mellitus in Singapore Chinese Men and Women
Article information

Abstract
Background
Multiple biomarkers have performed well in predicting type 2 diabetes mellitus (T2DM) risk in Western populations. However, evidence is scarce among Asian populations.
Methods
Plasma triglyceride-to-high density lipoprotein (TG-to-HDL) ratio, alanine transaminase (ALT), high-sensitivity C-reactive protein (hs-CRP), ferritin, adiponectin, fetuin-A, and retinol-binding protein 4 were measured in 485 T2DM cases and 485 age-and-sex matched controls nested within the prospective Singapore Chinese Health Study cohort. Participants were free of T2DM at blood collection (1999 to 2004), and T2DM cases were identified at the subsequent follow-up interviews (2006 to 2010). A weighted biomarker score was created based on the strengths of associations between these biomarkers and T2DM risks. The predictive utility of the biomarker score was assessed by the area under receiver operating characteristics curve (AUC).
Results
The biomarker score that comprised of four biomarkers (TG-to-HDL ratio, ALT, ferritin, and adiponectin) was positively associated with T2DM risk (P trend <0.001). Compared to the lowest quartile of the score, the odds ratio was 12.0 (95% confidence interval [CI], 5.43 to 26.6) for those in the highest quartile. Adding the biomarker score to a base model that included smoking, history of hypertension, body mass index, and levels of random glucose and insulin improved AUC significantly from 0.81 (95% CI, 0.78 to 0.83) to 0.83 (95% CI, 0.81 to 0.86; P=0.002). When substituting the random glucose levels with glycosylated hemoglobin in the base model, adding the biomarker score improved AUC from 0.85 (95% CI, 0.83 to 0.88) to 0.86 (95% CI, 0.84 to 0.89; P=0.032).
Conclusion
A composite score of blood biomarkers improved T2DM risk prediction among Chinese.
INTRODUCTION
The global prevalence of diabetes has increased explosively in the past three decades, particularly in Asian countries that have experienced rapid transitions in nutritional status and economic growth [1]. According to the International Diabetes Federation, a total of 425 million people had diabetes worldwide in 2017, with China ranking top (114.4 million) and Southeast Asia contributing to around one-fifth of world's population with diabetes [2]. Type 2 diabetes mellitus (T2DM) accounts for around 90% of diabetes cases [3], and several clinical trials have shown that intensive lifestyle modifications focusing on healthy diet and physical activity can prevent T2DM development [45]. Therefore, it is vital to identify individuals at higher T2DM risk so that intensive lifestyle and dietary interventions can be introduced to lower their risks of developing T2DM.
The etiology of T2DM involves complex yet poorly-understood interactions between genetic and environmental factors. Body mass index (BMI), family history of T2DM, fasting blood glucose and glycosylated hemoglobin (HbA1c) are clinical risk factors that are commonly used for identifying people at higher risk of developing T2DM [6]. However, the utility of these factors as predictors of T2DM in the general population is not high; for example, it has been estimated that less than 20% of obese Caucasians will progress to T2DM over the next few years [7], and genotype scores provide minimal improvement in the risk prediction on top of common risk factors [89]. In addition, by the time abnormal glucose regulation has been detected by blood measurements, a significant proportion of such individuals have already had complications due to the chronicity of T2DM progression [10]. In addition, diagnostic markers such as high blood glucose and HbA1c levels are outcome indicators of T2DM and provide limited insights into the underlying etiology [11].
Recent studies have shown that dysregulation of several metabolic pathways such as a failure of intracellular lipid homeostasis [12], abnormal adipocyte signaling [13], dyslipidemia [14], inflammation [15], and iron overload [16] preceded the development of T2DM. In addition, some biomarkers implicated in the abovementioned pathways, such as alanine transaminase (ALT) [17], fetuin-A [18], retinol-binding protein 4 (RBP4) [1920], adiponectin [21], triglyceride (TG) [2223], high density lipoprotein cholesterol (HDL-C) [2223], high-sensitivity C-reactive protein (hs-CRP) [24], and ferritin [25], have been found to be significantly associated with T2DM risk. Furthermore, epidemiological studies in Western populations have shown that combination of these biomarkers could improve T2DM prediction over traditional clinical risk factors [11262728293031], while such evidence is scarce in Asian populations. To our best knowledge, only one cross-sectional study has conducted joint analysis of multiple biomarkers for identifying T2DM in a Chinese population [32]. Compared with the Western populations, Asians develop T2DM at lower BMIs, have lower β-cell function and are more insulin resistant [33]. Thus, it is of scientific interest to assess whether joint analysis of multiple biomarkers could improve T2DM prediction in a prospective cohort study among Asian populations.
Thus, we conducted this nested case-control study within the Singapore Chinese Health Study to create a weighted biomarker score, and prospectively evaluate the association between the biomarker score and T2DM risk with adjustment for established T2DM risk factors. We further explored whether this biomarker score could improve T2DM prediction in this Chinese population.
METHODS
Study population
The Singapore Chinese Health Study is a population-based cohort study. At baseline between 1993 and 1998, a total of 63,257 Chinese living in Singapore (age range, 45 to 74 years) were recruited. At recruitment interviews, trained research staff collected information on medical history, diet intakes and lifestyle habits using structured questionnaires. From 1999 to 2004, we conducted the first follow-up interview by telephone, and re-interviewed 52,322 subjects to update their information on medical history and selected lifestyle habits. In addition, 32,535 participants consented and donated bio-specimens for the purpose of research. Subsequently, we carried out the second follow-up via phone from 2006 to 2010 and re-contacted 39,528 subjects, including 25,477 who donated their bio-specimens at the first follow-up. The Institutional Review Boards at the University of Pittsburgh and the National University of Singapore approved the study protocol (NUS-IRB Ref Code: 06-027), and all subjects signed the consent forms after hearing the full explanation of the purpose and nature of all procedures used. In addition, all procedures complied with the Declaration of Helsinki. The detailed description of the study design has been previously [34].
Ascertainment of T2DM and other covariates
At baseline and two follow-ups, we asked participants if a doctor had told them that they had diabetes. If participants answered yes, we also asked for the age of first diagnosis. We further validated the accuracy of the self-reported T2DM data in a separate study [35].
At recruitment, we collected information on age, body height and weight, education levels, smoking status, alcohol intakes, weekly activity levels, and history of hypertension, cardiovascular disease (CVD), stroke, and cancer. BMI was calculated using body weight (kg) divided by square of height (m).
Establishment of nested case-control study
Among subjects without physician-diagnosed T2DM, CVD and cancer during blood collection (1999 to 2004), 571 subjects reported that they were diagnosed with T2DM at the second follow-up visit (2006 to 2010), and thus were considered as incident T2DM cases for the current study. In the remaining subjects without T2DM at the second follow-up and had HbA1c <6.0%, controls were randomly chosen and matched with cases on a 1:1 ratio for age (±3 years), date of blood collection (±6 months), sex, and dialect group (Cantonese, Hokkien). The matching on dialect group was to reduce the confounding by culture, lifestyle, and genetic factors that may associated with different dialect group. A total of 86 pairs were excluded because either cases or controls in these pairs lacked the information for ferritin measurements. The final sample size for the current study was 485 case-control pairs. The flowchart of the study design is presented in Supplementary Fig. 1.
Laboratory measurements
We collected 20-mL morning blood from each consented participant at random time slots, and transported it to the laboratory with ice immediately. We separated the blood into different components including plasma, serum, red blood cells and buffy coat, and put all components in −80℃ freezers for long-term storage. For the current study, plasma samples from each case-control pair were analyzed in the same batch at the National University Hospital Reference Laboratory, Singapore.
Plasma levels of total cholesterol, HDL-C, TG, ALT, hs-CRP were determined by the colorimetric method (AU5800 Analyzer; Beckman Coulter, Brea, CA, USA). In addition, ferritin levels were measured by the Sandwich enzyme-linked immunosorbent assay (ELISA) method (Dxl 800 Analyzer; Beckman Coulter). Furthermore, levels of fetuin-A, adiponectin, and RBP4 were both determined via Sandwich ELISA (Bio-Rad Laboratories, Hercules, CA, USA). Moreover, HbA1c from the red blood cells was measured by the HPLC method (Bio-Rad Laboratories) in red blood cells. The within- and between-assay coefficients of variation of all measures were <10%.
Statistical analysis
Conditional logistic regression models were used to compute the odds ratio (OR) of each biomarker (quartiles) in association with T2DM risk. Model 1 was adjusted for age (years), education levels (none, primary, secondary, or higher), alcohol intakes (never or monthly, weekly, or daily), weekly physical activity levels (<0.5, 0.5 to 3.9, and ≥4.0 hr/wk), smoking status (never, ever smoker), BMI (kg/m2), history of hypertension and fasting status. Of note, since cases and controls were matched on age with a range of ±3 years, we adjusted for age as a continuous variable to further account for the residual confounding. Model 2 was further adjusted for all the blood biomarkers measured for this study. As a result, four biomarkers (TG-to-HDL ratio, ALT, ferritin, and adiponectin) were significantly associated with T2DM risk and were selected, and the biomarker score was derived using the equation: the biomarker score=k×(β1×biomarker1+β2×biomarker2+…+βk×biomarkerk)/(β1+β2+…+βk), where k=4 in this study [32]. To construct the composite score, we first used each biomarker as an ordinal variable, which has been used in studies to create weighted biomarker score [32] and genetic risk scores [3637]. The ordinal values of each biomarker in quartile categories (coded as 0, 1, 2, and 3 from the lowest to the highest quartile, except for adiponectin which was assigned reversely as 3, 2, 1, and 0 due to its inverse association with T2DM risk) were used as continuous variables in the conditional logistic regression models, and the corresponding weight of each biomarker was assigned by its respective β coefficient from the regression models. We chose quartile categories because they yielded better model fit compared to tertile and quintile categories. Subsequently, the association between the composite biomarker score and T2DM risk was assessed using multivariable conditional logistic regression models with adjustment for the abovementioned covariates in the total population. To test for the influence of potential selection bias, we further assessed the association both among T2DM cases with HbA1c <6.0% and <6.5% at baseline along with their matched controls. In addition, potential interactions between the biomarker score and age (<60 or ≥60 years), alcohol intakes (never or monthly, weekly or daily), weekly activity levels (<0.5 or ≥0.5 hr/wk), BMI (<23 or ≥23 kg/m2), and fasting status (yes, no) were tested by adding an interaction term (interaction variable×biomarker score) to the regression models. For stratified analyses by variables other than matching factors, unconditional logistic regression models with further adjustment for sex and dialect group were used. In addition, since our study did not have a validation cohort and thus may subject to overfitting, we used 10-fold cross validation method in the sensitivity analysis to evaluate the goodness-of-fit of the model, and used the root mean squared error as the assessment metric [38].
To assess the predictive performance of the biomarker score, we established three logistic regression models. Base model 1 was established using a forward selection procedure (P<0.05), and included age, history of hypertension, smoking status, and BMI. Sex and dialect group were not included in the prediction model because cases and controls were perfectly matched on these factors. Base model 2 additionally included the levels of random glucose and random insulin. Since HbA1c has been shown to outperform glucose levels in T2DM prediction [39], we further substituted the random glucose levels with HbA1c levels and established model 3. We have tested the added value of each individual biomarker and the biomarker score to each base model for T2DM prediction, and the improvement in the discrimination between the base models and the model plus the biomarker/biomarker score was compared by area under receiver operating characteristic curve (AUC) [40]. Moreover, net reclassification improvement (NRI) and integrated discrimination improvement (IDI) statistics were further used as complementary methods [4142]. NRI calculates the overall differences between higher predicted risk for T2DM cases and lower predicted risk for controls, where a higher value indicates better predictive capacity. Furthermore, Akaike information criterion (AIC) was used to evaluate the model fitness, where a lower value indicated better model fit. In addition, we repeated the abovementioned analyses only among cases with HbA1c <6.0% or <6.5% at baseline and their matched controls.
In the sensitivity analysis, we created another score using each biomarker as a continuous variable (per log change) which captured more information compared to treating biomarkers as ordinal variables. We compared the performance of the two scores in terms of association with and prediction for T2DM risk. We used STATA version 14.0 (Stata Corp., College Station, TX, USA) for all analyses, and considered two-sided P values <0.05 as statistically significant.
RESULTS
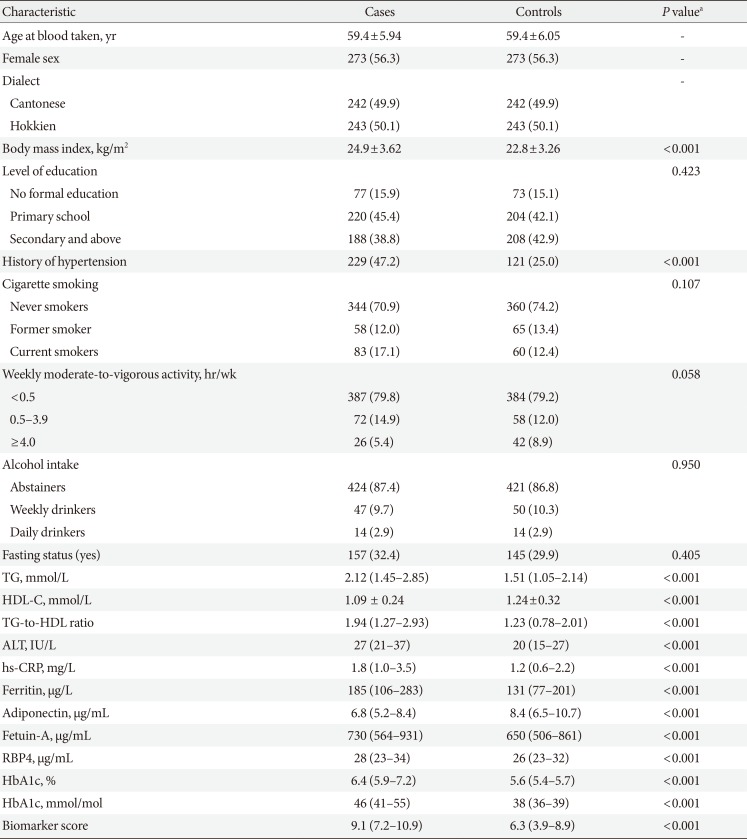
Compared with controls, cases had worse metabolic profiles: they were more likely to be heavier and hypertensive, as well as having higher levels of blood biomarkers that were T2DM risk factors (ALT, TG, TG-to-HDL ratio, hs-CRP, ferritin, fetuin-A, RBP4, HbA1c) and lower levels of protective biomarkers (adiponectin, HDL-C). However, distributions of other baseline characteristics such as education levels, weekly activity levels, smoking status, alcohol consumption, and fasting status of blood samples were similar between cases and controls (Table 1).

Baseline characteristics and biomarker levels of diabetes cases and matched controls, the Singapore Chinese Health Study
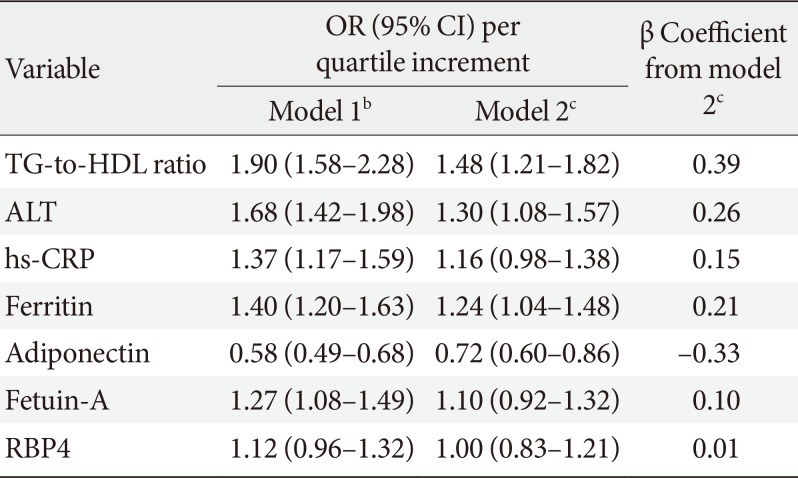
The associations between all biomarkers and T2DM risks are presented in Table 2. In a multivariable model that included all the biomarkers and potential confounders, hs-CRP (OR with per quartile increment was 1.16; 95% confidence interval [CI], 0.98 to 1.38), fetuin-A (OR with per quartile increment was 1.10; 95% CI, 0.92 to 1.32) and RBP4 (OR with per quartile increment was 1.00; 95% CI, 0.83 to 1.21) were not significantly associated with T2DM risk and thus were not included in the composite biomarker score. In addition, TG-to-HDL ratio, ALT and ferritin were positively associated with T2DM risk, and the respective OR (95% CI) per quartile increment was 1.48 (95% CI, 1.21 to 1.82), 1.30 (95% CI, 1.08 to 1.57), and 1.24 (95% CI, 1.04 to 1.48), while adiponectin was inversely associated with T2DM risk (OR with per quartile increment was 0.72; 95% CI, 0.60 to 0.86).

Associations between per quartile increment of all the biomarkers and risk of type 2 diabetes mellitusa
We created a biomarker score based on the four biomarkers with significant associations, using their β coefficients associated with per quartile increments. The biomarker score ranged from 0 to 12 with a median value of 8.0. The median of the score was 9.1 (interquartile range [IQR], 7.2 to 10.9) among cases and 6.3 (IQR, 3.9 to 8.9) among controls (P<0.001) (Table 1). The distribution of the biomarker score among cases and controls is shown in Fig. 1, and the distributions of the biomarker score and included biomarkers according to the quartiles of the biomarker score are shown in Supplementary Table 1.

Odds ratio for type 2 diabetes mellitus by the biomarker score and percentages of participants in each biomarker score category. The solid line represents the point estimates of relative risk for the association between the biomarker score and the risk of incident type 2 diabetes mellitus using conditional logistic regression model after adjustment for age at blood taken (years), smoking (never, ever smoker), alcohol intake (never, weekly, or daily), weekly activity (<0.5, 0.5 to 3, and ≥4 hr/wk), education level (primary school and below, secondary or above), history of hypertension (yes, no), body mass index (kg/m2), fasting status (yes, no), and levels of random glucose and random insulin, and the dotted lines represent the upper and lower bound of 95% confidence interval (CI). The light grey bars represent the percentage of controls within each category for the biomarker score (n=485), and the dark grey bars represent the percentage of cases within each category for the biomarker score (n=485).
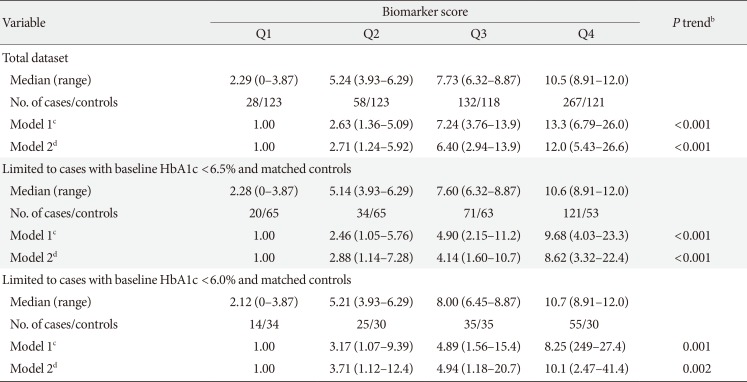
The association between the biomarker score established based on the ordinal variables and T2DM risk is shown in Table 3 and Fig. 1. In the total population (485 case-control pairs), the biomarker score was positively associated with T2DM risk in a dose-dependent manner (P trend <0.001). Compared to those in the lowest quartile of the score, the OR was 12.0 (95% CI, 5.43 to 26.6; P trend <0.001) for those in the highest quartile. In addition, among 246 cases with baseline HbA1c <6.5% or 129 cases with HbA1c <6.0% and their respective matched controls, the strong positive association between the biomarker score and T2DM risk remained largely unchanged, and the OR comparing the highest versus lowest quartile of the biomarker score for T2DM risk was 8.62 (95% CI, 3.32 to 22.4; P trend <0.001) and 10.1 (95% CI, 2.47 to 41.4; P trend <0.001), respectively. Furthermore, in the stratified analysis, although the association was slightly stronger among participants with older age (≥60 years), higher BMI (≥23 kg/m2), more physical activity (≥0.5 hr/wk) and non-fasted samples compared to their respective counterparts, no significant interaction has been observed (Supplementary Table 2). In addition, the 10-fold cross validation test has suggested similar model fit from 10 attempts, and the root mean squared error ranged from 0.63 to 0.72.

Odds ratios (95% confidence intervals) of type 2 diabetes mellitus associated with quartile levels of the ordinal biomarker scorea
The predictive performance of the biomarker score is presented in Table 4. The AUC of the base model comprising age, smoking status, BMI and history of hypertension was 0.70 (95% CI, 0.66 to 0.73). When adding the composite biomarker score to the base model, the AUC was improved to 0.76 (95% CI, 0.73 to 0.79; P<0.001). In addition, when the base model was further included random glucose and insulin levels, adding the biomarker score increased AUC from 0.81 (95% CI, 0.78 to 0.83) to 0.83 (95% CI, 0.81 to 0.86; P=0.002). When substituting the random glucose levels and HbA1c in the base model, adding the biomarker score still yield a small yet statistically significant increment in AUC from 0.85 (95% CI, 0.83 to 0.88) to 0.86 (95% CI, 0.84 to 0.89; P=0.032). Moreover, when restricting to cases with baseline HbA1c <6.0% or <6.5% and their controls, significant improvements in AUCs were also observed. Furthermore, NRIs were all positive values, thus suggested that adding the biomarker score significantly improved the prediction of T2DM risk (all P<0.001).

Summary statistics to assess the biomarker score in predicting type 2 diabetes mellitus, the Singapore Chinese Health Study
To further stratify the NRI analyses by T2DM status, adding the biomarker score on top of base model 3 correctly assigned 32.0% of T2DM cases to a higher predicted T2DM risk and 15.5% of controls to a lower predicted T2DM risk in the total population (Supplementary Table 3). In the subgroup of cases with HbA1c <6.5% and matched controls, the biomarker score correctly re-assigned 31.7% cases and 14.6% controls. Moreover, in cases with HbA1c <6.0% and their matched controls, the biomarker score correctly reassigned 24.0% cases to higher T2DM risk and 8.6% controls to lower T2DM risk (Supplementary Table 3).
Since TG-to-HDL ratio and ALT are routine clinical tests, we also compared the performance the biomarker score with TG-to-HDL ratio and ALT alone. Adding to the base model comprising age, smoking status, BMI and history of hypertension, the biomarker score had stronger association than TG-to-HDL ratio and ALT alone (OR comparing the highest vs. lowest quartile: 13.3 [95% CI, 6.79 to 26.0] vs. 8.03 [95% CI, 4.45 to 14.5]), better discrimination (AUC, 0.76 [95% CI, 0.73 to 0.79] vs. 0.75 [95% CI, 0.72 to 0.78]), better model fit (AIC, 468 vs. 489), and additionally reclassified 12.4% participants to the correct T2DM risk category (Supplementary Table 4).
In the sensitivity analysis, we further created a biomarker score using each biomarker as a continuous variable, and calculated the corresponding β coefficient associated with per log increment of each biomarker (Supplementary Table 5). The continuous biomarker score ranged from −1.3 to 5.8 with a median value of 2.5, and the median of the score was 3.0 (IQR, 2.1 to 3.9) among cases and 1.8 (IQR, 0.6 to 2.9) in controls (P<0.001; data not shown). In terms of association, the continuous biomarker score has shown similar strength of association with T2DM risk compared to the ordinal score, and the OR comparing the extreme quartile of the score was 14.2 (95% CI, 6.03 to 33.3) in the total population (Supplementary Table 6). Regarding prediction, the continuous biomarker score had the same performance compared to the ordinal score: adding the continuous biomarker score to the base Model 1, 2, and 3 increased AUCs from 0.70 (95% CI, 0.66 to 0.73) to 0.76 (95% CI, 0.73 to 0.79), 0.81 (95% CI, 0.78 to 0.83) to 0.83 (95% CI, 0.81 to 0.86), and 0.85 (95% CI, 0.83 to 0.88) to 0.86 (95% CI, 0.84 to 0.89), respectively (all P<0.05) (Supplementary Table 7). In addition, the abovementioned association and prediction of the continuous score were essentially the same among cases with baseline HbA1c <6.0% or <6.5% and their matched controls.
DISCUSSION
In this middle-aged and older Chinese adults living in Singapore, we found that a weighted biomarker score, comprising TG-to-HDL ratio, ALT, ferritin, and adiponectin, was strongly associated with T2DM risk. The participants in the highest versus lowest quartile had an approximately 12-fold increased risk of T2DM. In addition, the biomarker score significantly improved the T2DM prediction, and it correctly reassigned 32.0% cases to higher T2DM risk and 15.5% controls to lower T2DM risk. Collectively, our results suggested that joint analysis of multiple biomarkers may be a useful tool to predict T2DM risk.
A few studies that have examined the predictive utility of multiple biomarkers for T2DM prediction have also included biomarkers that were common to the current study [1126272829303132]. A cross-sectional study in a Chinese population showed that a weighted biomarker score that included adiponectin, ferritin and two other inflammatory biomarkers (plasminogen activator inhibitor-1 and interleukin 6) substantially improved discrimination (AUC, NRI, and IDI) of T2DM risk [32]. Similarly, studies conducted across Western countries such as Denmark [11], Germany [2627], Switzerland [28], France [29], Finland [30], and United States [31] have also shown that adding adiponectin and/or ferritin along with other biomarkers have improved T2DM prediction on top of lifestyle characteristics, glucose and/or insulin parameters. Of note, the results from a prospective German cohort had an overlap of four biomarkers (TG, HDL-C, ALT, and adiponectin) with the current study, and the study showed that these biomarkers along with GGT and hs-CRP significantly improved T2DM on top of fasting glucose and HbA1c [26]. In addition, other risk scores developed in Asian populations (China [4344] and Korea [4546]) that mainly comprised of clinical information and lifestyle factors also included biomarkers such as lipids [43444546] or liver enzyme [46] that were similar to the current study.
The significant association between each biomarker included in the score (TG-to-HDL ratio, adiponectin, ferritin, and ALT) were consistent with findings across populations [172122232425]. Experimental studies have provided the biological plausibility for the underlying mechanisms of these biomarkers in the pathogenesis of T2DM. High TG or low HDL, resulting in a high TG-to-HDL ratio as a marker for dyslipidemia, may increase T2DM risk through lipotoxicity, inflammation, and endoplasmic reticulum stress [14]. Adiponectin, a well-known adipokine, has been shown to improve insulin sensitivity and glucose metabolism [47]. Ferritin, a widely-used marker for body iron, has been linked to T2DM risk through insulin resistance and β-cell function impairment [16]. ALT, the most specific marker for liver injury and a surrogate marker for nonalcoholic fatty liver disease [48], has been shown to impact T2DM risk by increasing hepatic insulin resistance, inflammation and dysregulation of lipid and glucose metabolism [49].
Although the clinical usefulness of the biomarker score has been shown in the current study, whether the biomarker score is also cost-effectiveness is unclear yet. Among the four biomarkers, TG-to-HDL ratio and ALT are routinely tested in the clinical setting, while measurements for adiponectin and ferritin are less common and could be expensive. Though evidence is scarce regarding the cost-effectiveness of utilization of adiponectin and ferritin in clinical settings, a study in the United States has shown that a biomarker score (PreDx Diabetes Risk Score) comprised of adiponectin, ferritin, and five other biomarkers (glucose, insulin, HbA1c, C-reactive protein, and interleukin 2 receptor-α) was more cost-effective than using the impaired fasting glucose alone over a 10-year period [50]. However, since no other study has examined this issue, future studies are warranted to evaluate the cost-effectiveness of the biomarker score developed in the current study.
To our best knowledge, this is the first prospective study in a Chinese population to evaluate the value of a weighted biomarker score for T2DM prediction. In addition, we comprehensively used AUC, NRI, and IDI to evaluate the predictive performance of the biomarker score. However, several limitations merit consideration. First of all, biomarkers were measured in one-time collection of blood samples from the participants and we could not study subsequent changes in these biomarkers. Furthermore, residual confounding may exist since body weight and height, and history of hypertension were self-reported. In addition, information on family history of T2DM and waist circumference was not collected; therefore, we could not apply the basic prediction model that were used in other studies which comprised of these variables [2830].
In conclusion, we have shown the utility of a composite score of four biomarkers as a predictor of T2DM in a Chinese population, and our finding suggest that this score is a promising marker as a screening tool to identify at-risk individuals for targeted diet and lifestyle intervention. Future studies are warranted to further validate these findings in other populations to determine cut-off values for more precise risk prediction of T2DM and to investigate the upstream factors that influence the levels of the biomarkers, as well as to evaluate the cost-effectiveness of the biomarker score in the local setting and other Asian countries.
ACKNOWLEDGMENTS
This work was supported by the National Medical Research Council, Singapore (NMRC/CIRG/1354/2013) and National Institutes of Health, USA (RO1 CA144034 and UM1 CA182876). Woon-Puay Koh is supported by the National Medical Research Council, Singapore (NMRC/CSA/0055/2013). An Pan is supported by the National Key Research and Development Program of China (2017YFC0907504).
We thank Siew-Hong Low of the National University of Singapore for supervising the fieldwork of the Singapore Chinese Health Study, and Renwei Wang for the maintenance of the cohort study database. We also thank the founding principal investigator of the Singapore Chinese Health Study, Mimi C. Yu as well as all the cohort participants.
Notes
CONFLICTS OF INTEREST: No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTIONS:
Conception or design: W.P.K., X.S., A.P.
Acquisition, analysis, or interpretation of data: Y.W., W.P.K., X.S., J.M.Y., A.P.
Drafting the work or revising: Y.W., W.P.K., X.S., J.M.Y., A.P.
Final approval of the manuscript: Y.W., W.P.K., X.S., J.M.Y., A.P
References
SUPPLEMENTARY MATERIALS
Supplementary materials related to this article can be found online at https://doi.org/10.4093/dmj.2019.0020.
Supplementary Table 1
Distribution of the biomarker score and included biomarkers according to the quartiles of the biomarker score
Supplementary Table 2
Odds ratios (95% confidence intervals) of type 2 diabetes mellitus by stratified analysis
Supplementary Table 3
Reclassification of diabetes cases and controls with no categories based on their ordinal biomarker scorea
Supplementary Table 4
Summary statistics to assess the biomarker score versus TG-to-HDL ratio and ALT in predicting type 2 diabetes mellitus, the Singapore Chinese Health Study
Supplementary Table 5
Associations between per log increment of all the biomarkers and risk of type 2 diabetes mellitusa
Supplementary Table 6
Odds ratios (95% confidence intervals) of type 2 diabetes mellitus associated with quartile levels of the continuous biomarker scorea
Supplementary Table 7
Summary statistics to assess the continuous biomarker score in predicting type 2 diabetes mellitus, the Singapore Chinese Health Study
Supplementary Fig. 1
Flowchart of the Singapore Chinese Health Study. HbA1c, glycosylated hemoglobin.