Diabetes Fact Sheets in Korea, 2018: An Appraisal of Current Status
Article information

Abstract
Background
The objective of this study was to investigate the prevalence, management, and comorbidities of diabetes among Korean adults aged 30 years and older.
Methods
This study used 2013 to 2016 data from the Korea National Health and Nutrition Examination Survey, a nationally-representative survey of the Korean population. Diabetes was defined as fasting glucose ≥126 mg/dL, current use of antidiabetic medication, a previous history of diabetes, or glycosylated hemoglobin (HbA1c) ≥6.5%.
Results
In 2016, 14.4% (approximately 5.02 million) of Korean adults had diabetes. The prevalence of impaired fasting glucose was 25.3% (8.71 million). From 2013 to 2016, the awareness, control, and treatment rates for diabetes were 62.6%, 56.7%, and 25.1%, respectively. People with diabetes had the following comorbidities: obesity (50.4%), abdominal obesity (47.8%), hypertension (55.3%), and hypercholesterolemia (34.9%). The 25.1%, 68.4%, and 44.2% of people with diabetes achieved HbA1c <6.5%, blood pressure <140/85 mm Hg, and low density lipoprotein cholesterol <100 mg/dL. Only 8.4% of people with diabetes had good control of all three targets.
Conclusion
This study confirms that diabetes is as an important public health problem. Efforts should be made to increase awareness, detection, and comprehensive management of diabetes to reduce diabetes-related morbidity and mortality.
INTRODUCTION
Economic and social developments have affected lifestyles and diet habits, resulting in increases in non-communicable diseases, such as obesity, dyslipidemia, hypertension, and diabetes. Diabetes is associated with a high risk of vascular disease. Cardiovascular disease is a primary cause of death among people with type 2 diabetes [12]. In Korea, four million adults aged 30 years or older have diabetes. The prevalence of diabetes has been estimated to be 12.4% in Korea in 2011 [34]. In 2016, diabetes was the sixth leading cause of death and the most common cause of renal replacement therapy in Korea [5]. The increase in diabetes has, consequently, resulted in an increase in diabetes-related morbidity, thus becoming a socioeconomic burden. Therefore, recognizing problems in reaching glycemic target goals and seeking solutions are important to decrease the comorbidities and mortality of diabetes. Since 2012, The Korean Diabetes Association (KDA) has published Diabetes Fact Sheets based on the Korea National Health and Nutrition Examination Survey (KNHANES), a nationwide survey conducted by the Korean Centers for Disease Control and Prevention to promote the understanding of chronic diseases, provide comprehensive and systematic prevention and management at the national level, and improve public awareness of diabetes and its risk factors. More active, comprehensive management of diabetic patients is a very important health issue. The objective of this study was to investigate the prevalence, management, and comorbidities of diabetes among Korean adults aged 30 years and older by analyzing nationally-representative KNHANES data.
METHODS
Study population
This study analyzed KNHANES data from 2013 to 2016, a nationally representative, cross-sectional survey designed to evaluate the health and nutritional status of the Korean population. KNHANES consists of three surveys: a health interview survey, a health examination survey, and a nutrition survey. The health interview included prior history of diabetes diagnosis, hypertension, hypercholesterolemia, and medication for those conditions. Informed consent was obtained during the KNHANES process. The estimated percentages and the total number of people over the age of 30 with diabetes and prediabetes were determined by reflecting the 2016 demographic structure. We constructed two datasets from KNHANES as follows: (1) KNHANES 2016 and (2) KNHANES 2013 to 2016 (merged 4 years of data). Data form KNHANES 2016 were used to calculate the prevalence of diabetes and impaired fasting glucose (IFG). And, data for KNHANES 2013 to 2016 (4 years of data) were used to identify current status of managing diabetes and comorbidities in diabetes. The study protocol conformed to the ethical guidelines of the World Medical Association Declaration of Helsinki and was approved by the Institutional Review Board of Soonchunhyang University Bucheon Hospital (IRB No 2018-11-018).
Biochemical measurements
After an overnight fast, fasting plasma glucose (FPG), total cholesterol (TC), high density lipoprotein cholesterol (HDL-C), triglyceride (TG) level, serum creatinine level, and urinary concentration of creatinine were measured using a Hitachi Automatic Analyzer 7600 (Hitachi, Tokyo, Japan). Low density lipoprotein cholesterol (LDL-C) was measured by direct assay for persons with TG >200 mg/dL (Hitachi Automatic Analyzer 7600). Thus, we used either directly measured or calculated LDL-C according to the Friedewald formula: LDL-C=TC–HDL-C–(TG/5) [6]. Glycosylated hemoglobin (HbA1c) levels were measured using high-performance liquid chromatography (HLC-723G7; Tosoh, Tokyo, Japan). Urinary albumin levels in random urine samples were measured using a Hitachi Automatic Analyzer 7600.
Definitions of diabetes and its related comorbidities
The diagnosis of diabetes was based on FPG ≥126 mg/dL, current use of antidiabetic medication(s), a previous history of diabetes, or HbA1c ≥6.5%. IFG was defined by FPG in the range of 100 to 125 mg/dL among those without diabetes as described above [7]. Glycemic control rate in diabetes was defined as rate of people of HbA1c <6.5% among people with diabetes (%). Obesity was defined as a body mass index (BMI; weight in kilograms divided by the square of height in meters) ≥25.0 kg/m2 in accordance with the Asia-Pacific criteria of the World Health Organization guidelines [8]. Abdominal obesity was defined as waist circumference ≥90 cm in men and ≥85 cm in women. Hypertension was defined ad systolic blood pressure ≥140 mm Hg or diastolic blood pressure ≥90 mm Hg and/or current use of antihypertensive medications. Control of hypertension was defined as systolic and diastolic blood pressure <140/85 mm Hg according to the KDA Treatment Guideline for Diabetes 2015 (English version is available at www.diabetes.or.kr) [9]. Hypercholesterolemia was defined as TC ≥240 mg/dL or current use of lipid-lowering medication(s), and control of hypercholesterolemia was defined as LDL-C <100 mg/dL [910]. Awareness rate was defined as rate of people diagnosed with diabetes by a doctor among people with diabetes (%). Treatment rate was defined as rate of people treated with oral hypoglycemic agents, or insulin therapy among people with diabetes (%). Definition of health behaviors are as follows: current smoking: smoked at least five packs of cigarettes (100 cigarettes) during lifetime; high-risk drinking: more than seven glasses in men or five glasses in women on the same occasion on each of two or more a week; regular walking exercise: 5 days or more per week and for 30 minutes or more per activity.
Statistical analysis
Descriptive statistics were used to evaluate the patient data. Statistical analyses were performed using SAS statistical software version 9.3 (SAS Institute Inc., Cary, NC, USA) to reflect the complex sampling design and sampling weights of KNHANES and to provide nationally representative prevalence estimates using a complex sampling design.
RESULTS
Prevalence of diabetes and IFG
Among adults aged 30 years or more in 2016, the prevalence of diabetes was 14.4%, representing approximately 5.02 million. There were differences in diabetes prevalence by sex, age group, and household income. The prevalence of diabetes among women in 2016 was 13.0%, which was lower than that in men (15.8%). The prevalence increased with age in both sexes. Specifically, the prevalence exceeded 10% for men in the 40 to 49 age group and for women in the 50 to 59 age group. In addition, the prevalence of diabetes among adults 65 years or older was 29.8%. By household income quartile, the prevalence in the lowest household income quartile was 14.7%, while that in the highest household income quartile was 10.8% (Fig. 1). The prevalence of IFG among adults 30 years or older in 2016 was 25.3%. The number of people with IFG was estimated to be 8.71 million in 2016. The IFG prevalence peaked in the of 50- to 59-year-old age group in men and in the 60- to 69-year-old age group in women (Fig. 1).
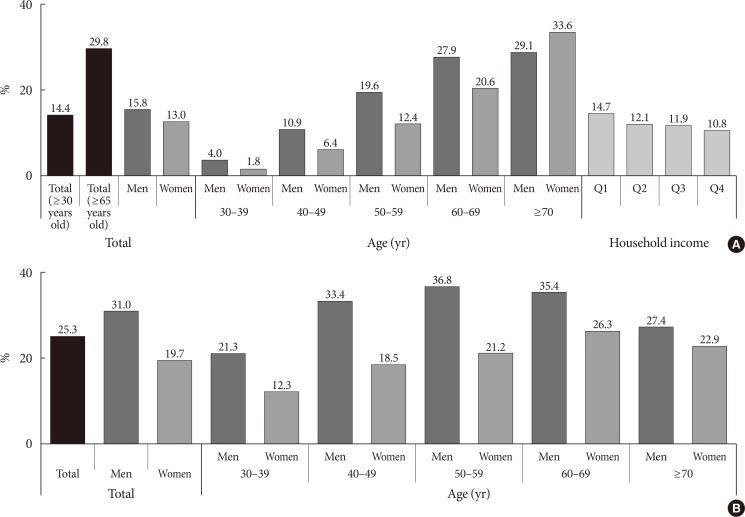
Estimated prevalence of adults (≥30 years old) with (A) diabetes and (B) impaired fasting glucose (household income: from the lowest to the highest quintiles [Q]).
Current status of managing diabetes
In 2013 to 2016, among people with diabetes, 62.6% were aware of their condition and 56.7% were using glucose-lowering drugs (oral hypoglycemic agent, 51.5%; insulin therapy, 5.2%). However, 43.1% were not receiving any treatment (glucose-lowering drugs and/or lifestyle modification). Among people who were previously diagnosed with diabetes, 9.2% were not receiving any treatment for their disease. However, most of them were being treated with oral hypoglycemic agents (82.3%) and 8.3% of them were receiving insulin therapy (Fig. 2). Glycemic control rate among people with diabetes was 25.1% for HbA1c <6.5% and 52.6% for HbA1c <7.0%. However, 20.9% of people with diabetes had worse glycemic control (HbA1c ≥8.0%) (Fig. 3).
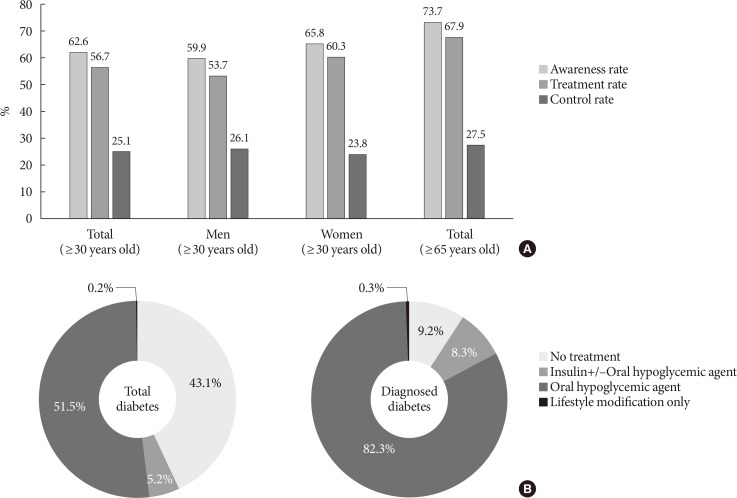
Management of (A) diabetes and (B) type of treatment (awareness rate: rate of people diagnosed with diabetes by a doctor among people with diabetes [%]; treatment rate: rate of people treated with oral hypoglycemic agents, and/or insulin therapy among people with diabetes [%]; control rate: rate of people of glycosylated hemoglobin <6.5% among people with diabetes).
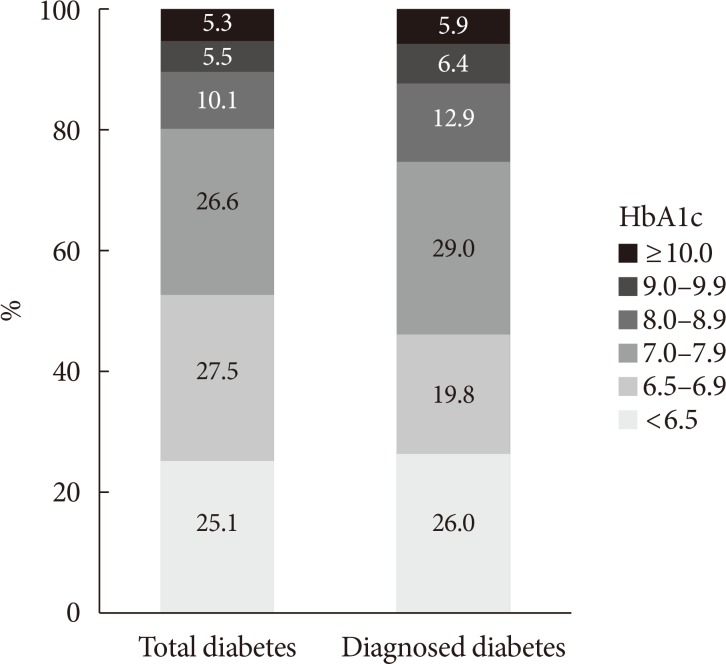
Glycemic control rate in diabetes. HbA1c, glycosylated hemoglobin.
Comorbidities in diabetes
In 2013 to 2016, the prevalence of obesity (BMI ≥25.0 kg/m2) in people with diabetes was 50.4%. When obesity was categorized as class I to III, obesity class I (BMI 25.0 to 29.9 kg/m2) accounted for 40.2% of the diabetes cases and obesity class II (BMI 30.0 to 34.9 kg/m2) accounted for 8.4%, while obesity class III (BMI ≥35.0 kg/m2) only accounted for 1.8%. Abdominal obesity, based on waist circumference (men ≥90 cm, women ≥85 cm), accounted for 47.8% of the people with diabetes. The prevalence of abdominal obesity was higher in women than in men (men 44.2%, women 52.1%). In diabetes, the prevalence of hypertension was 55.3% and that of hypercholesterolemia was 34.9% (Fig. 4).
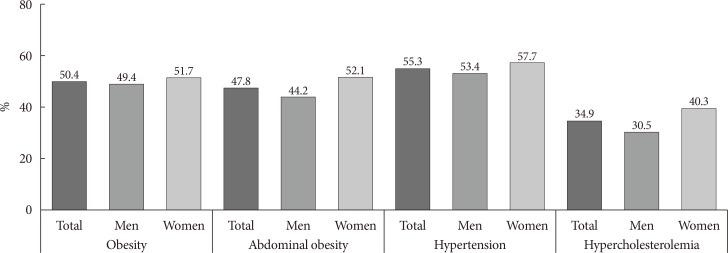
Estimated prevalence of comorbidities in diabetes (obesity: body mass index [kg/m2] ≥25.0; abdominal obesity: men ≥90 cm, women ≥85 cm; hypertension: systolic blood pressure ≥140 mm Hg or diastolic blood pressure ≥90 mm Hg and/or antihypertensive medications; hypercholesterolemia: total cholesterol ≥240 mg/dL and/or lipid-lowering medications).
According to the 2015 KDA treatment guideline, 25.1% of people with diabetes achieved HbA1c <6.5%, 68.4% achieved blood pressure <140/85 mm Hg, and 44.2% achieved LDL-C <100 mg/dL. Only 8.4% of people with diabetes had good control of all three targets. In addition, more men than women were current smokers (men 39.6%, women 5.3%) or high-risk drinkers (men 24.3%, women 3.1%). Only 36.0% of those with diabetes were walking 30 minutes regularly (Fig. 5).
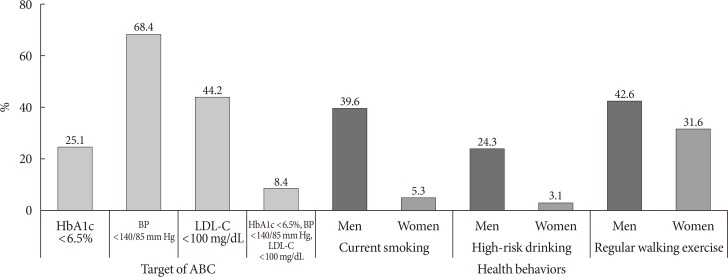
Control rate of comorbidities and estimated proportion for health behaviors in diabetes (current smoking: smoked at least five packs of cigarettes [100 cigarettes] during lifetime; high-risk drinking: more than seven glasses in men or five glasses in women on the same occasion on each of 2 or more a week; regular walking exercise: 5 days or more per week and for 30 minutes or more per activity). HbA1c, glycosylated hemoglobin; BP, blood pressure; LDL-C, low density lipoprotein cholesterol; ABC, glycosylated hemoglobin, blood pressure, and low density lipoprotein cholesterol.
DISCUSSION
In a representative sample of Korean adults in 2016, the prevalence of diabetes among adults aged 30 years or more was 14.4% and the estimated number of people with diabetes was 5.02 million. Excluding HbA1c from the definition of diabetes, the prevalence decreased to 13.0%. In addition, the prevalence of IFG was 25.3%.
In Korea, the prevalence of diabetes has mainly increased due to population aging [11]. This study also showed that the prevalence of diabetes increased with age in both sexes. Specifically, the prevalence of diabetes among adults 65 years or older was 29.8%, which was more than twice the prevalence of diabetes among adults aged 30 years or more. Diabetes in the elderly is accompanied by functional disability, several comorbidities, and premature mortality [12]. Thus, the management of diabetes is necessary, especially considering the prevalence and comorbidities in the elderly.
This study showed that the lower the income level, the higher the prevalence of diabetes. Previous studies have shown that people with low socioeconomic status (SES) were more likely to develop type 2 diabetes with worse glycemic control that can lead to more diabetic complications [1314]. According to the Korean National Diabetes Program (KNDP) cohort study, men with low SES had worse glycemic control and higher risk for retinopathy [15]. In addition, in Korea, low-income people with diabetes had lower medication adherence and lower levels of utilization of fundus examinations and HbA1c tests than high-income people with diabetes [16].
Improved awareness of diabetes through early detection should be prioritized in diabetes management. However, from 2013 to 2016, the diabetes awareness rate was only 62.6%, which was lower than that (68.0%) in 2005 [17]. The reason for the decrease in awareness was that the number of undiagnosed diabetes cases increased when HbA1c was included in the diagnosis of diabetes from 2013 to 2016. In addition, 43.1% did not take treatment with glucose-lowering drugs or modify their lifestyle. Although the rate of worse glycemic control (HbA1c ≥8.0%) fell steadily from 33.6% in 2005 to 20.9% in 2013 to 2016 [18], good control (HbA1c <6.5%) was only achieved in 25.1% of the patients.
In addition, more than half the people with diabetes had comorbidities. According to the KNHANES 2011 study, the prevalence of dyslipidemia, hypertension, and obesity was 79.6%, 54.6%, and 44.4%, respectively, among adults with diabetes [19]. In 2013 to 2016, the prevalence of hypertension and obesity among people with diabetes was higher, while the prevalence of dyslipidemia was lower compared to the data in 2011. However, in 2011, the definition of dyslipidemia included hypercholesterolemia, hypertriglyceridemia, hyper-LDL-cholesterolemia, or hypo-HDL-cholesterolemia. Thus, we could not exactly compare the differences in prevalence.
Tight glycemic control and treatment of additional cardiovascular risk factors can decrease diabetic complications [202122]. Thus, the management of diabetes through achievement of the ABC clinical targets (A, HbA1c; B, blood pressure; and C, LDL-C) is important. However, only 8.4% of subjects achieved all three ABC targets. Also, 24.1% were current smokers, 14.7% were high-risk drinkers, and only 36.4% were walking 30 minutes regularly. Compared to a previous study, the proportion of current smokers among people with diabetes has decreased and that of people who participate in regular walking exercise activities has significantly increased. However, the proportion of high-risk drinkers among people with diabetes has slightly increased. The incidence of type 2 diabetes is closely related to diet and lifestyle [2324]. Several studies have shown that alcohol consumption can increase the risk of diabetes, even in the case of moderate consumption [2526], while another study reported that moderate alcohol consumption decreased the risk of type 2 diabetes [27]. Although there is still controversy about the effect of moderate alcohol consumption, heavy alcohol drinking is known to potentiate the development of diabetes through pancreatic β-cell dysfunction [2829]. In addition, the prevalence of alcohol dependence and alcohol abuse is much higher in Korea compared to other countries [30]. Thus, it is necessary to inform people with diabetes about the danger of alcohol consumption and the importance of decreasing alcohol intake.
In conclusion, increasing awareness and strengthening the management of people with diabetes can have a positive impact on the prevention of diabetes-related complications. However, the prevalence of diabetes is constantly increasing, while the awareness and control rates are still low in Korea. Thus, we need to construct a systemic approach to supporting diabetic patients, ranging from early detection to target-driven management.
ACKNOWLEDGMENTS
This study was supported by The Korean Diabetes Association.
Notes
CONFLICTS OF INTEREST: No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTIONS:
Conception or design: J.C.W., D.J.K., K.S.P.
Acquisition, analysis, or interpretation of data: B.Y.K., J.C.W., J.H.L., H.S.K., J.H.P., D.J.K.
Drafting the work or revising: B.Y.K., K.H.H., K.C.W., D.J.K.
Final approval of the manuscript: K.C.W., D.J.K., K.S.P.