The Role of Negative Affect in the Assessment of Quality of Life among Women with Type 1 Diabetes Mellitus
Article information

Abstract
Background
The purpose of this study is to determine the impact of negative affect (defined in terms of lack of optimism, depressogenic attributional style, and hopelessness depression) on the quality of life of women with type 1 diabetes mellitus.
Methods
Participants (n=177) completed either an online or paper questionnaire made available to members of Australian diabetes support groups. Measures of optimism, attributional style, hopelessness depression, disease-specific data, and diabetes-related quality of life were sought. Bivariate correlations informed the construction of a structural equation model.
Results
Participants were 36.3±11.3 years old, with a disease duration of 18.4±11.2 years. Age and recent glycosylated hemoglobin readings were significant contextual variables in the model. All bivariate associations involving the components of negative affect were as hypothesized. That is, poorer quality of life was associated with a greater depressogenic attributional style, higher hopelessness depression, and lower optimism. The structural equation model demonstrated significant direct effects of depressogenic attributional style and hopelessness depression on quality of life, while (lack of) optimism contributed to quality of life indirectly by way of these variables.
Conclusion
The recognition of negative affect presentations among patients, and an understanding of its relevance to diabetes-related quality of life, is a valuable tool for the practitioner.
INTRODUCTION
In the absence of a cure, the goals for those with type 1 diabetes mellitus (T1DM) are to successfully navigate the rigors of a self-management program, and to maintain blood glucose levels as near to normal as practicable through the use of injected insulin, while preserving quality of life [1]. The primary health practitioner is key to identifying and alleviating barriers to these goals. Yet given the constellation of potential comorbidities, which may be biological, psychological, or social [2], subtle presentations may go unheeded. Negative affect is one such psychological barrier. Encompassing subjective feelings of distress, it is a commonly used construct in behavioral medicine [34]. Negative affect may manifest in a number of forms, including all of behavioral (functional impairment), affective (rumination on current negative circumstances), and cognitive processes [5]. The latter is most common, and the current study highlights the interplay between three cognitions (lack of optimism, attributional style, and hopelessness depression), and their potential to negatively impact quality of life [6]. In the current study this inquiry is conducted using only a sample of women who, compared with men, find diabetes self-management particularly challenging. They have poorer metabolic control [7], twice as many depressive symptoms, an increased likelihood of major depression [89], and poorer quality of life [1011].
Optimism
Optimism reflects the dispositional tendency to believe that, on balance, more desirable than undesirable events will occur in the future [12]. Research has demonstrated that when individuals encounter challenging medical events, higher optimism is associated with resilience against stress [13], better quality of life [14], and fewer symptoms of depression [15]. While there is as yet little research concerning optimism in individuals with T1DM, there are nonetheless hints as to its relevance. In a study of multiple chronic illnesses, including T1DM, those who were more optimistic were more likely to perform proactive health-related behaviors [16]. Arguably, individuals with T1DM who are positive about their future may have better quality of life because they remain engaged with the goal of self-management, despite adversity.
Hopelessness depression
Hopelessness depression is described in terms of its emotional and motivational symptoms such as sad affect, lack of energy, apathy, psychomotor retardation, sleep disturbance, and, at times, lowered self-esteem and dependency [17]. It is argued that this emphasis on motivational deficits may be more relevant to understanding wellbeing among people with T1DM than depression per se. Further, hopelessness is a noted barrier to wellbeing for those with T1DM [18]. Hopelessness depression may be proposed to develop from the perception that efforts to effectively manage diabetes are useless, with the motivation to do so in turn depleted.
Attributional style
The final component of negative affect to be considered is attributional style. Specifically, a predisposition to view negative events as stable (likely to recur in similar situations), global (something affecting other aspects of their lives), and important has been termed a depressogenic attributional style [19]. This has been linked previously to poorer wellbeing in children with diabetes [20]. Of note is that depressogenic attributional style has a significant influence on hopelessness depression, but not other forms of depression [21]. Among individuals with diabetes, this may occur through the belief that appropriate self-care behaviors will not have the desired outcome.
Hypotheses and analytical strategy
With optimism reverse coded to reflect lack of optimism, all components of negative affect were hypothesized to share positive bivariate associations. It was further hypothesized that all would demonstrate negative bivariate associations with quality of life. Beyond these relationships, it was possible to propose a putative causal order among the negative affect variables which was tested using a path analysis model. Specifically, as optimism is considered a dispositional characteristic, it was assessed first in the causal chain. That is, it was proposed that participants with lower dispositional optimism would be at greater risk of expressing both a depressogenic attributional style and hopelessness depression. Further, the evidence reviewed above led to the proposition that a depressogenic attributional style would be a precursor to hopelessness depression. Together, these associations were predicted to manifest, by way of both direct and indirect paths, as lower quality of life.
METHODS
Participants and procedure
The study was approved by the authors' institutional research ethics committee. Women with T1DM (n=177) participated in this study. A convenience sample was recruited from online support groups and education seminars. Eligibility comprised a diagnosis of T1DM for at least 6 months, aged at least 18 years, with the ability to comprehend an English language questionnaire. Participation was sought in two ways. First, an online questionnaire link was made available to members of key Australian diabetes support groups (e.g., Diabetes Australia). Second, the lead author attended local diabetes education seminars. Brief details concerning the aims of the study were provided prior to consent and access to the questionnaire. All responses were provided anonymously, either online or in a reply-paid envelope.
Measures
Age, duration of disease, and participants' most recent glycosylated hemoglobin (A1C) reading were recorded as contextual variables.
Optimism
The revised Life Orientation Test is a reliable and valid 6-item measure of dispositional optimism [22]. Respondents indicate their agreement with items (e.g., ‘I rarely count on good things happening to me’) using a 5-point scale (‘strongly disagree’ to ‘strongly agree’). Optimism is treated as a single dimension with scores coded such that higher values indicate a greater lack of optimism (range, 6 to 30).
Hopelessness depression
Eight items from the Beck Depression Inventory [23], previously nominated as indicative of hopelessness depression, were used [21]. Symptoms surveyed were sadness, hopelessness, suicidality, indecisiveness, work difficulty, sleep disturbance, tiredness and lack of energy. Responses scored from 0 to 3 (summated range, 0 to 24) allowed participants to indicate the degree to which each symptom described the way they had felt over the past 6 months. Higher scores represent more severe hopelessness depression.
Attributional style
Depressogenic attributional style was evaluated using the Balanced Attributional Style Questionnaire [24]. Respondents provide a cause for each of eight scenarios with a negative outcome (e.g., ‘You have been looking for a job unsuccessfully for some time’) and rate that cause on 7-point scales for stability (1, will never again be present; 7, will always be present), globality (1, influences just this particular situation; 7, influences all situations in my life), and importance (1, not at all important; 7, extremely important). All ratings are then combined, with possible scores ranging from 24 to 168 and higher scores indicating greater depressogenic style.
Quality of life
The 15-item Diabetes Quality of Life scale assesses impact on day-to-day functioning [25]. Participants use 5-point scales to record either their satisfaction (‘very dissatisfied’ to ‘very satisfied’; e.g., ‘How satisfied are you with your current treatment?’), or how often they feel or act a certain way (‘all the time’ to ‘never’; e.g., ‘How often do you find that you eat something you shouldn't rather than tell someone that you have diabetes?’). Items are summed (range, 15 to 75), with higher scores indicating a better quality of life.
Statistical analyses
Data were analysed using SPSS version 22 (IBM Co., Armonk, NY, USA). Bivariate hypothesis tests comprised Pearson correlation coefficients, while multivariate analyses were conducted within a Structural Equation Modelling framework using Analysis of a Moment Structures (AMOS) algorithms [26]. The goal was to iteratively test the proposed model until the properties of theoretical sense, reasonable parsimony, and an acceptably close correspondence to the data, were achieved [27]. A range of goodness-of-fit indices are reported as is the usual recommendation. However, thresholds for acceptable model-fit associated with these indices should be considered ‘rules of thumb’ at best [28]. Path coefficients are standardized. Non-significant paths that did not contribute to an improvement in overall model fit have been removed to improve interpretation. Similarly, error terms for endogenous variables are not shown.
RESULTS
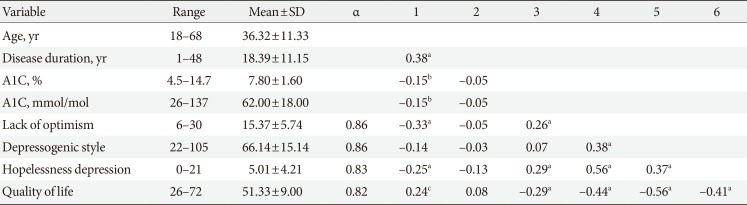
Table 1 provides descriptive data, including internal reliability (α) where applicable. Also shown are the bivariate associations among these variables. Age, disease duration, and most recent A1C level are included as potential contextual (endogenous) variables. Unsurprisingly, disease duration was longer for older participants while being unrelated to other study measures. It was therefore omitted from further analyses. However, increasing age was also associated with modestly lower A1C and hopelessness depression, better quality of life, and higher optimism. A1C was also higher among those who reported lower optimism, higher hopelessness depression, and lower quality of life. As predicted, all indicators of negative affect shared positive relationships. Also as predicted, all elements of negative affect were significantly related to quality of life, with higher negative affect associated with lower quality of life.

Summary statistics and intercorrelations for key study variables
With respect to the structural equation model (Fig. 1), final fit indices suggested satisfactory model fit. The model chi-square was non-significant (χ2(1)=1.53, P=0.217), and both the normed fit index and comparative fit index were excellent (0.99). The Tucker-Lewis index was good (0.94). The root-mean-square error of approximation (RMSEA) was also good at 0.055, although the upper limit of the 90% confidence interval (CI, 0.000 to 0.217) was higher than desirable. The obtained path coefficients largely mirrored the bivariate results described above, albeit at more modest levels due to multicollinearity. However, a modest number of previously-significant bivariate associations were no longer evident, yet still contributed to improved model fit. These are clearly noted in Fig. 1. Importantly, the direct relationship between lack of optimism and quality of life was channeled totally through depressogenic style and hopelessness depression.
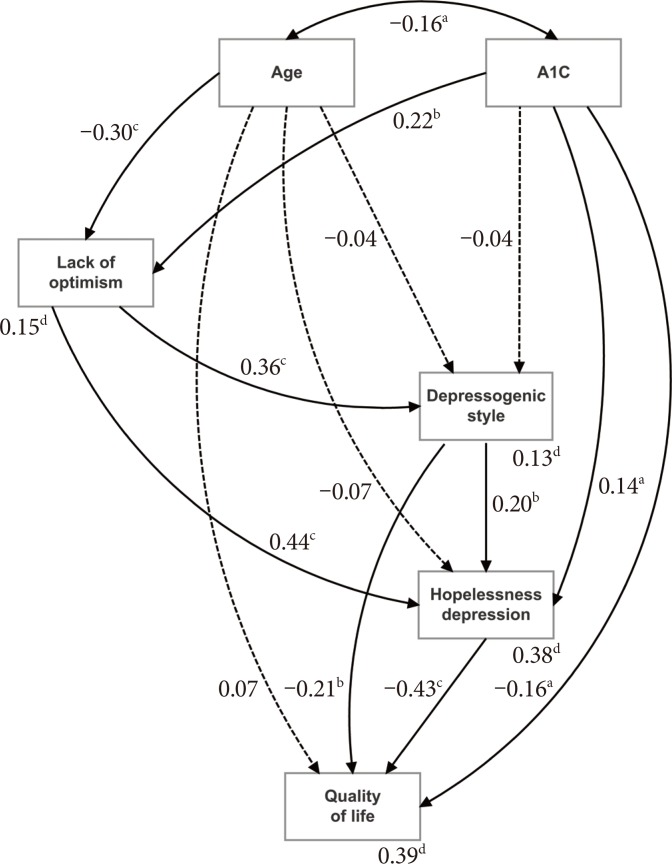
Structural equation model demonstrating the hypothesized paths linking hopelessness depression, depressogenic attributional style and lack of optimism, respectively, with quality of life: significant paths (←), non-significant paths (-->), covariances (↔). A1C, glycosylated hemoglobin. aP<0.05, bP<0.01, cP<0.001, dCoefficients are squared multiple correlations (R2).
The percentage of variance of each outcome variable accounted for by all predictors (squared multiple correlations, R2) is also shown in Fig. 1 (footnote ‘d’). The key outcome (quality of life) had 39% of its variance accounted for. Further, with indirect effects taken into account, the total effect of depressogenic attributional style on quality of life increased from −0.21 (the magnitude of the direct path) to −0.30 (P<0.001; the sum of the direct path and the indirect path through hopelessness depression to quality of life). Similarly, the total effect of A1C increased from −0.16 (the magnitude of the direct path) to −0.27 (P<0.001; the sum of the direct path and the indirect path through hopelessness depression to quality of life). Finally, the total effect of age increased from 0.07 (the magnitude of the direct path) to 0.20 (P<0.01; the sum of the direct path and all indirect paths from age to quality of life). Lack of optimism only impacted on quality of life by way of indirect effects through depressogenic style and hopelessness depression but was nevertheless important (−0.29, P<0.001).
DISCUSSION
The variables considered in the current study, characterized as negative affect, illustrate the multiple paths by which distress may impact on quality of life for those coping with a chronic illness. The unique and joint effects of a lack of optimism, depressogenic attributional style and hopelessness depression, were assessed among a sample of women with T1DM. The hypothesized relationships involving all variables were noteworthy. In general, higher levels of negative affect were associated with poorer quality of life. The findings add to a growing body of literature in two ways. First, the evaluation of the broader construct of negative affect, rather than elements of depression per se [29], and second its specific application to the diabetes context.
The univariate results were in accord with prediction. That is, negative affect was significantly associated with poorer quality of life. Those concerning hopelessness depression were novel, although the general role of hopelessness as a barrier to adjustment to diabetes among those with T1DM has been previously briefly acknowledged [18]. Of greater importance, however, were the multivariate results that allowed the examination of the joint effects of study variables on diabetes-related quality of life. This model allowed both direct and indirect (mediation-based) effects of the three indicators of negative affect to be evaluated. Key to the model were the hypothesized roles of lack of optimism, and depressogenic style, with hopelessness depression nominated as the primary ‘driver’ of quality of life. On balance, the hypothesized relationships were supported, although depressogenic attributional style was noted to have a significant direct effect on quality of life as well as a mediated effect through hopelessness depression. Further, with total effects of −0.29 (lack of optimism), −0.30 (depressogenic attributional style), and −0.43 (hopelessness depression), the model suggested that all three indicators were salient.
Interpretation of these results leads to the consideration that perhaps those with T1DM with higher negative affect become less attentive towards the management of their disease which, through experiencing the physical symptoms of fluctuating blood glucose levels, could impact on quality of life. Such poor attention to management may be due to a lack of motivation, a perception that their diabetes management is challenging or burdensome (a result previously noted among young people with diabetes) [30], and/or negative expectancies about the outcome of management efforts [31]. While this is a plausible explanation, such a causal assertion has not strictly been tested in the current study, with the hypothesis that challenges to management precede increases in negative affect also being credible.
The current results may also contribute to an understanding of existing conflicting evidence of the nature and role of depression in T1DM [32]. As previously noted, terms such as ‘depression,’ ‘depressive symptoms,’ and ‘clinical depression’ appear to be used somewhat interchangeably in the literature. However, it is unlikely in the majority of cases that people with T1DM will present with, or develop, diagnosable clinical depression. Rather, they may present with a range of symptoms that illustrate their position on a mood state continuum that we have argued includes negative affect.
Limitations and recommendations
The current results should not be considered without due acknowledgement of some important caveats. First, the sample recruited was of modest size and it is self-evident that future investigations would benefit from an examination of the impact of a larger sample on multivariate models such as those presented. Second, the current study was concerned only with female participants, and so the generalizability of the findings to men remains of interest. Third, although the negative affect indicators were demonstrated to influence quality of life, this process has the potential to be bidirectional. A longitudinal research design would allow a deeper analysis of the relationships among such indicators while taking into account the evolution of the illness over time. Fourth, it has to be considered that people of different ages face challenges of T1DM in different ways, such as in relation to available resources and the specific developmental tasks required across the life span [33], suggesting that further research is warranted in order to appreciate the relevance of age differences to the associations under investigation. Fifth, there are other variables which may influence the associations described. These include socioeconomic and life-style related characteristics and psychiatric disorders. These were not collected in the current study, but are worthy of consideration in future investigations, and may further increase the validity of the current findings. Finally, it is important to also study the behavioral manifestation of negative affect on quality of life through the addition of self-management practices to the analyses. For example, it may be hypothesized that the association between negative affect and quality of life is mediated by self-management.
Implications
Diabetes has long been considered a disease in which psychosocial as well as health related issues are relevant. Quality of life was the focus of this study, and the clinical importance of the results are worthy of consideration; that is, in terms of strategies of management to effect an adequate response to treatment. It was expected that women with T1DM who experienced negative affect would have poorer disease-related quality of life. While this expectation was met in univariate analyses, multivariate models demonstrated the greater importance of hopelessness depression and a depressogenic attributional style, respectively.
Clinicians treating this group should routinely screen their patients for negative affect and associated behaviors that may impede adjustment, and work towards an appropriate response in order to promote optimal short- and long-term outcomes. The consequence of these findings includes, but is not limited to, psychological ill-health and diabetic complications. Although pharmacologic strategies have strong efficacy for treatment of depression there are a number of associated repercussions, or costs, with a corollary being a necessary heterogeneity in management regimens. Finally, a greater understanding of the cognitive mechanisms associated with diabetes and its management may serve to augment the emerging evidence of the effectiveness of psychoeducation as an intervention to improve outcomes for patients [34].
Notes
CONFLICTS OF INTEREST: No potential conflict of interest relevant to this article was reported.