The Correlations between Extremity Circumferences with Total and Regional Amounts of Skeletal Muscle and Muscle Strength in Obese Women with Type 2 Diabetes
Article information
Abstract
Background
Insulin resistance is related to central obesity and the amount of skeletal muscle. A simple and practical anthropometric marker for muscle mass is not known, although waist circumference (WC) is used as an indicator of abdominal obesity. The aims of this study were to investigate whether arm (AC) and thigh circumferences (TC) can be used as an indicator of muscle mass and if they are related to muscle strength.
Methods
A total of 110 obese (body mass index [BMI]≥25 kg/m2) women with type 2 diabetes were enrolled, and WC, AC, and TC were measured. Abdominal visceral fat (AVF), subcutaneous fat (ASF), and total fat (ATF) were assessed by computed tomography, regional muscle (MM), and fat mass by dual-energy X-ray absorptiometry, muscle strength by one repetition maximum (1RM) of both extremities (chest and leg press) and insulin resistance by KITT.
Results
The mean age was 56.2±7.3 years, duration of diabetes was 4.2±4.4 years, and BMI was 27.2±2.8 kg/m2. WC was correlated with ATF, AVF, and ASF (r=0.728, P<0.001; r=0.515, P<0.001; r=0.608, P<0.001, respectively). Arm MM was correlated with AC (r=0.500, P<0.001), and leg MM with TC (r=0.291, P=0.002). Upper 1RM was related to AC/WC ratio (r=0.359, P<0.001), and lower 1RM was to TC/WC ratio (r=0.286, P=0.003). Insulin resistance had significant relations with AVF, WC, and total MM (r=-0.262, P=0.008; r=-0.217, P=0.029; r=0.160, P=0.031, respectively).
Conclusion
The muscle mass was related to extremity circumferences, and muscle strength was to extremity/waist circumference ratio in obese women with type 2 diabetes.
INTRODUCTION
The increase in abdominal fat, especially in visceral portion, causes hypertension, hyperlipidemia, type 2 diabetes, and metabolic syndrome. Compared to Western populations, the level of obesity in Asians is not as high. Reportedly, as the percentage of visceral fat increases, the prevalence of diabetes and metabolic syndrome increases [1]. Waist circumference is correlated with the amount of abdominal fat and thus has been accepted as an indicator of metabolic syndrome and for assessing abdominal obesity [2]. The increase in muscle mass improves insulin sensitivity and helps control blood glucose in type 2 diabetes patients [3]. Dunstan et al. [4] reported that insulin sensitivity improves as muscle mass increases. However, muscle mass decreases with age, with seniors over 65 years of age experiencing an approximately 25% muscle loss, and seniors over 80 years of age experiencing an approximately 50% muscle loss [5]. To improve stamina, the American Diabetes Association recommends aerobic exercise to improve muscle strength at 75% to 85% maximum intensity with 8 to 10 exercises per day and 3 sets of resistance exercises 3 times per week [6]. Since skeletal muscle is considered the major organ responsible for glucose uptake under insulin-stimulated conditions, measuring muscle mass and muscle strength in type 2 diabetic patients is necessary.
Muscle mass can be measured accurately using dual-energy X-ray absorptiometry (DXA), and muscle strength can be measured accurately using a one repetition maximum (1RM). Generally, when muscular strength is measured, the bench press or chest press is used for the upper body, in which the main functioning muscles are the biceps and the triceps. Maximum lower muscle strength is generally measured using a leg press and squats, in which the main functioning muscles are the quadriceps, hamstrings, and glutei. The measurement of muscle mass is complicated, and care must be given to joint and muscle strain when measuring maximum muscle strength in patients with low muscular strength, and patients who cannot be measured require simple indicators. Additionally, Cha et al. [7] performed a study targeting middle-aged women based on the correlation between the visceral fat/skeletal muscle ratio and insulin resistance because changes in the fat/muscle mass ratio and its correlation with insulin resistance are high. However, simple indicators for estimating amount of skeletal muscle are yet to be suggested.
Thus, in the present study, the relationships between limb circumferences and regional muscle amounts in obese female type 2 diabetes patients were investigated, as were the correlations between maximum muscular strength with arm/waist circumference ratio and thigh/waist ratio (fat/muscle mass ratio).
METHODS
Study target
The participants of the present study included patients between the ages of 40 to 60 years who visited the Eulji Hospital Diabetes Center between September 2008 and August 2009, who were diagnosed with diabetes based on the criteria set by the World Health Organization (WHO), and who were not receiving insulin treatment. Among the patients, type 1 diabetes patients, patients with genetic disease, patients with chronic complications of diabetes, congestive heart failure, uncontrolled arrhythmia, severe valvular heart disease, unmanageable hypertension, neuropathy, retinopathy, and patients who were unable to perform strenuous exercise due to severe health conditions were excluded from the present study. In addition, patients with a body mass index (BMI) greater than 25 kg/m2 who were classified as being obese and patients with HbA1c level less than 9% (n=110) were included in the present study.
Measurement methods
Physical measurements and biochemical tests
The height, weight, waist circumference, upper arm and thigh circumferences of the study participants were measured. Height and weight were measured with patients wearing a thin robe, and BMI was calculated by dividing mass (kg) by height squared (m2). Waist circumference was measured when patients exhaled and relaxed using a tape measure on the thinnest portion between the bottom rib and the iliac crest. Arm circumference was measured between the acromion and the elbow using a tape measure when patients were standing with their arms comfortably spread, and thigh circumference was measured immediately below the line of the thickest area of the buttocks when the legs were spread 10 cm apart in the standing position, and the average of each thigh was recorded [8]. Blood pressure was measured using a mercury sphygmomanometer (Yamasu, Tokyo, Japan) after the patients were seated for 10 minutes.
For biochemical tests, venous blood was drawn after more than 10 hours of fasting, and samples were centrifuged at 3,000 rpm for 15 minutes. Serum was separated, and samples were frozen at -70℃ and stored for further analysis. The glucose oxidation method was used to measure fasting blood glucose, and HbA1c was measured using high-performance liquid chromatography (HPLC). Fasting blood glucose, cholesterol, triglycerides, high density lipoprotein cholesterol (HDL-C) and low density lipoprotein cholesterol (LDL-C) were analyzed using an automatic biochemical analyzer that utilizes enzymatic reactions (Hitachi 7170; Hitachi, Tokyo, Japan). Fasting insulin concentrations were analyzed using electrical luminescence immunoassays Inmylife 2000 (Siemens, Mountain View, CA, USA).
Insulin resistance was measured using KITT [9], after fasting for a minimum of 10 hours prior to visiting the hospital, and a 20 G catheter was inserted into the patients' antecubital vein on one side of the body and was used to collect blood samples. On the opposite side, a 20 G catheter was inserted into a forearm vein, and after insulin shots were administered and the examination was finished, intravenous glucose was used. In a stable condition, 0.1 U of previously-diluted insulin (Humulin R; Eli Lilly, Indianapolis, IN, USA) was calculated per kg of body weight and injected into a forearm vein. On the opposite side, blood was sampled from the antecubital vein, at 0, 3, 6, 9, 12, and 15 minutes. For the prevention of hypoglycemia, after 15 minutes of blood sampling, 100 mL of 20% glucose was administered intravenously, blood samples were immediately centrifuged and glucose concentrations were measured. The glucose concentrations measured over time during the assessment of insulin resistance were entered into a computer program. Each value was converted into a natural log, and the slope of the regression line was calculated using the values collected between 3 and 15 minutes. Subsequently, the point at which baseline blood glucose decreased by half (half life [t1/2]) was obtained, and the insulin resistance blood glucose reduction rate indicator (rate constant for plasma glucose disappearance, KITT) was calculated using the following formula:
KITT=0.693/t1/2×100 (%/min)
Maximum strength (1RM)
In order to measure maximum strength, a chest press was used for the upper body, which measured the muscle strength of the deltoids, triceps, and pectoral muscle groups. A leg press was used for the lower body and measured the muscle strength of the gluteal, hamstring and quadriceps muscle groups (Keiser, Fresno, CA, USA). First, in order to measure maximum strength, 50% of the expected maximum weight was lifted 8 to 10 times for a light warm-up (1/2 of upper body weight and 1/2 of lower body weight). Afterward, patients performed gentle stretches for 3 minutes and rested for 1 minute. Participants performed one set of approximately 75% of the maximum weight that was expected to be lifted 3 to 5 times. After 1 minute, patients attempted to lift an additional 1.25 to 4.5 kg to reach their maximum strength capacity. This was performed until patients were unable to lift anymore, and the final weight lifted was recorded as the maximum strength. The maximum was typically determined within 3 to 5 attempts [10]. Grip strength was also examined (Hand grip, T.K.K.540; DAKEI, Tokyo, Japan).
DXA
Total body fat and muscle mass were measured using DXA (GE LUNAR, Madison, WI, USA). The body weights of patients were measured while wearing light clothing, and head to toe scans were performed when patients were lying down in a comfortable state on the examination bed. The examination took approximately 10 to 20 minutes. Body composition including body fat and muscle mass was measured separately for arm, leg, trunk, and total. Whole-body somatic volume was calculated using the enCORE program (version 11.x; GE LUNAR).
Computed tomography (CT)
CT of the abdominal region was used to measure total fat, visceral fat, and subcutaneous fat. The CT (Hispeed NX/I; GE, Milwaukee, WI, USA) method utilized was based on the method by Smith et al. [11], which was uniformly performed starting from the 4th to the 5th lumbar vertebra and extending to the naval area. The CT scan was performed in a 10 mm range, and the reorganized fat density results ranged between -190 to -30 Hounsfield units (HU). Using CT, cross-sectional abdominal fat volume was calculated. The distributions of the abdomen and the peritoneum were measured inside of the boundary area to determine visceral fat volume. Subcutaneous fat was calculated by subtracting the visceral fat volume from the total abdominal fat volume.
Statistical analysis
The statistical method for calculating the mean and standard deviation of the scores collected was performed using SPSS for Windows version 15.0 (SPSS Inc., Chicago, IL, USA). In addition, variables outside of the normal distribution were noted as median and interquartile range and were analyzed after log transformation. The Pearson's correlation analysis was performed on the relationships between circumferences and maximum strengths of the upper arms and thighs. The correlation coefficient 'r,' was used to determine degrees of correlation, and statistical significance was described as P values of less than 0.05.
RESULTS
Clinical characteristics of participants
A total of 110 female type 2 diabetes patients were enrolled in the present study. The average age was 56.2±7.3 years, and the average diabetes duration was 4.2±4.4 years. Average height, body weight, BMI, and waist circumference were 156.9±4.4 cm, 67.0±6.9 kg, 27.2±2.7 kg/m2, and 89.4±6.7 cm, respectively. Average glycated hemoglobin, HDL-C, and LDL-C were 7.1%±0.9%, 44.5±12.7 mg/dL, and 99.9±32.3 mg/dL, respectively (Table 1).
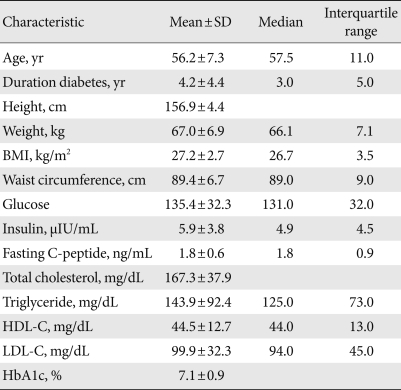
The clinical characteristics of the subject (n=110)
Correlations among abdominal fat mass, waist circumference, and insulin resistance
The average total abdominal fat was 393.8±87.1 cm2, and visceral fat and subcutaneous fat were 157.8±44.4 cm2 and 234.9±66.7 cm2, respectively.
The abdominal total fat mass measured using CT had a strong positive correlation with waist circumference (r=0.728, P<0.001), and visceral fat and subcutaneous fat had statistically significant positive correlations with waist circumference (visceral fat, r=0.515, P<0.001; subcutaneous fat, r=0.608, P<0.001). Additionally, visceral fat and waist circumference both showed a negative correlation with insulin resistance evaluated by KITT (visceral fat, r=-0.262, P=0.008; waist circumference, r=-0.217, P=0.029). Neither abdominal total fat mass nor subcutaneous fat had a linear correlation with KITT result (abdominal total fat mass, r=-0.151, P=0.130; subcutaneous fat, r=-0.032, P=0.753) (Table 2).

Correlations between abdominal fat, waist circumference and insulin resistance
The relationships of insulin resistance with muscle mass, extremity circumference and their ratios to waist circumference
The total average muscle mass was 40,031.3±3,794.1 g, and the upper and lower body muscle masses were 4,054.0±536.9 g, and 12,158.8±1,438.8 g, respectively. Additionally, the average upper arm and thigh circumferences were 32.5±2.5 cm, and 53.7±3.9 cm, respectively.
Insulin resistance expressed as KITT had a weak correlation with total muscle mass (r=0.160, P=0.031), but not with upper or lower extremity muscle mass (arm, r=0.067, P=0.501; leg, r=0.073, P=0.464). The upper arm and thigh circumference had no linear relationship with upper and lower extremity muscle mass (upper arm, r=0.096, P=0.348; thigh, r=0.053, P=0.605, respectively). The thigh/waist circumference ratio showed a slight correlation with KITT value (r=0.227, P=0.025), but the upper arm/waist circumference ratio did not (r=0.127, P=0.212) (Table 3).
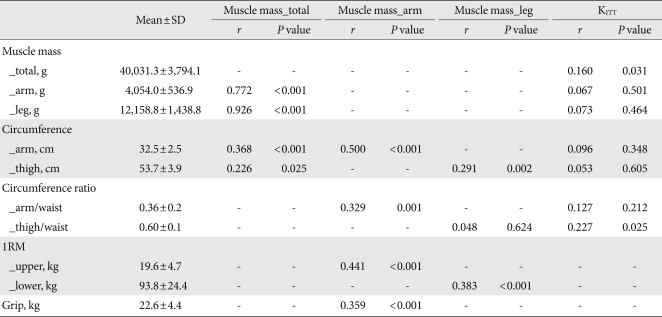
Correlations between muscle mass, circumference, muscle strength and insulin resistance
The relationships of insulin resistance with muscle mass with 1RM and extremity circumferences
Arm muscles accounted for 10.1% of total muscle mass and had a strong positive correlation with total muscle mass (r=0.772, P<0.001). Leg muscles accounted for 30.4% of total muscle mass, which had a statistically strong positive correlation with total muscle mass (r=0.926, P<0.001). The muscle to fat ratio in upper extremity was 1.7±0.4, that in the lower extremity was 2.1±0.8, and that in total body was 1.7±0.4.
Total muscle mass had a significant positive correlation with upper arm circumferences and weakly with thigh circumferences (r=0.368, P<0.001; r=0.226, P=0.037, respectively). The muscle mass in upper extremity showed a significant positively correlated with upper arm circumference, and the upper arm/waist circumference ratio (r=0.500, P<0.001; r=0.329, P=0.001, respectively). Additionally, there was a statistically significant positive correlation between 1RM of upper extremity and hand grip power (r=0.441, P<0.001; r=0.359, P<0.001). The muscle mass in lower extremity showed a significant positive correlation with thigh circumference and 1RM of lower extremity (r=0.291, P=0.002; r=0.383, P<0.001, respectively), but not with thigh/waist circumference ratio (r=0.048, P=0.624) (Table 3).
The ratios of muscle mass of upper and lower extremity to BMI in the present study were 45.5% and 63.6% of those in previous studies, respectively. When the total muscle mass and upper arm circumference reference values were investigated, the average muscle mass/BMI ratio in the previous study corresponding to the upper arm circumference in the present study was 32.4 cm, the corresponding upper arm/waist circumference ratio were 0.36, and arm muscle mass was 3,992.1 g (Fig. 1).

Correlations between muscle mass, circumference and arm/waist circumference ratio.
Extremity circumferences and muscle strength
The upper arm circumference and upper arm/waist circumference ratio were significantly positive correlations with 1RM of upper extremity (r=0.255, P=0.009; r=0.359, P<0.001, respectively). However, they did not have a linear correlation with the upper arm muscle mass/fat mass ratio (r=0.008, P=0.937).
The thigh circumference and thigh/waist circumference ratio was slightly positively correlated with lower body muscle mass (r=0.276, P=0.005; r=0.286, P=0.003, respectively). However, they did not have a linear correlation with the lower body muscle mass/fat mass ratio (r=0.037, P=0.702).
Grip power had no linear correlation with any measurements including upper arm circumference, upper arm/waist circumference ratio or upper body muscle mass/fat mass ratio (r=0.138, P=0.170; r=0.156, P=0.122; r=0.123, P=0.213, respectively) (Table 4).
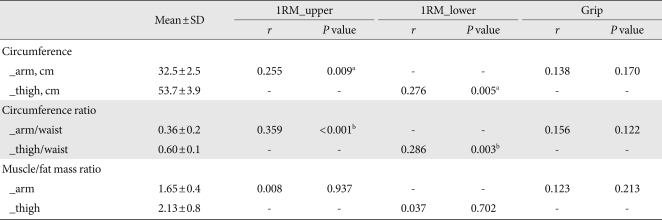
Correlations between muscle strength, circumference and muscle mass
The 1RM of upper and lower extremity to body weight ratio from previous studies was 0.27. When compared with the results from the present study (1.40), 1RM of upper extremity had a 44.0% correspondence, and 1RM of lower extremity had a 50% correspondence. When the determined reference values of maximum strength and upper arm circumference were investigated, the average upper arm circumference to maximum upper body strength correlation was 32.3 cm, and the corresponding upper body/waist circumference ratio was 0.36, and the upper body maximum strength was 19.0 kg (Fig. 2).
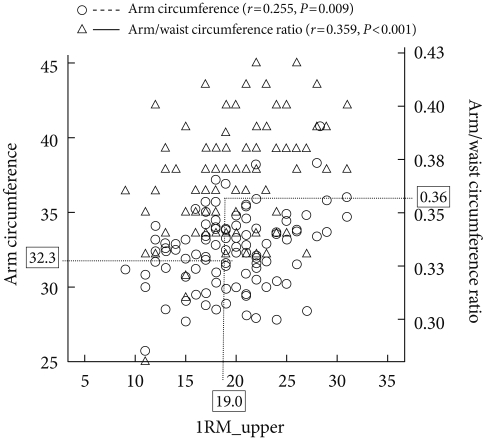
Correlations between muscle strength, circumference and arm/waist circumference ratio. 1RM, one repetition maximum.
DISCUSSION
The anthropometric measurement for abdominal obesity was the waist circumference to define metabolic syndrome [12]. The waist circumference cutoff by the Korean Society for the Study of Obesity [13] was 85 cm, and 74.5% of the participants (82 patients) in the present study had abdominal obesity. In a study by Jung et al. [14] performed on a total of 84 female type 2 diabetes patients with an average age of 63 years, the average BMI was 25.0 kg/m2, and average visceral fat and subcutaneous fat levels were 136 cm2 and 176 cm2, respectively. The average visceral fat and subcutaneous fat levels in the present study were 157.8 cm2 and 234.9 cm2, respectively. Visceral fat levels were similar between the studies, while the subcutaneous fat level in the present study was higher. Additionally, in a previous study performed by Kwon et al. [15] on corresponding females in their 50s, the average 1RM of the upper and lower extremity were 17.8 kg and 89.8 kg, respectively, and their ratios to the body weight were 0.29 and 1.40, respectively. The average upper body and lower body maximum strengths from the present study were 19.6 kg and 93.8 kg, respectively, and the strength to weight ratios were 0.29 and 1.40, respectively. Similar lower body results were observed in other previous studies, and grip strength in the present study was 22.6 kg, comparable to that in a study performed by An et al. [16] on female type 2 diabetes patients in their 50s who had an average hand grip strength of 23.1 kg.
Even when BMI is normal, if the waist circumference is high, patients are at a high risk for diabetes or cardiovascular disease [17]. Kim et al. [18] performed a study on 2,033 type 2 diabetic patients, in which an average age was 58.7 years. The average BMI was 25.4 kg/m2, and waist circumference was 88.2 cm. The present study was performed on obese patients with a higher BMI and waist circumference. The abdominal visceral adiposity has been reported to cause stronger insulin resistance than does subcutaneous fat [19,20]. Miyazaki et al. [21] reported a correlation between an increase in visceral fat and insulin resistance in a study performed on 62 type 2 diabetes patients between 30 and 70 years of age with a high BMI of at least 37 kg/m2. In the present study, the correlation between visceral fat and insulin resistance was higher, and waist circumference was shown to have a strong association with abdominal fat. In addition, waist circumference might be considered to be an indicator of insulin resistance.
The skeletal muscles are also the tissues that related with insulin resistance in type 2 diabetes patients and the accumulation site of metabolites from fatty acids. Muscle mass accounts for 35% to 40% of total body weight, and that is primary site for oxidation of glucose and fatty acids [22]. In a study performed by Dunstan et al. [4] on type 2 diabetes patients, the authors reported that as muscle mass increases, insulin resistance improves. In the present study, the insulin resistance expressed as KITT, and total muscle mass had a significant correlation and these findings are consistent with the results from previous studies. There was no correlation reported between extremity circumferences and extremity muscle mass, which was consistent with the knowledge that insulin resistance cannot be predicted with body circumference. However, there were significant correlations between change in fat mass/muscle mass ratio, upper arm/waist ratio and thigh/waist ratio with insulin resistance and between thigh/waist circumference ratio and improvements in insulin resistance.
Kim et al. [23] reported a significant correlation between the low density muscle mass of the femoral quadriceps muscle and insulin resistance in obese subjects, which was consistent with reports from a similar study. The authors of the present study recommend additional research on insulin resistance and femoral quadriceps muscle increase in Korean diabetes patients.
Changes in muscle mass and size are generally evaluated using BMI and body circumference measurements [24]. In a previous study, Kwon et al. [25] reported that, as the BMIs in the male and female participants increased, the muscle mass also increased, but also reported that muscle mass did not increase in female diabetes patients with a BMI greater than 25 kg/m2. In a study on muscle mass analysis by Kim [26] on healthy 20 to 73-year-old subjects (total 212 participants), female participants between 40 and 59 years of age with a mean BMI of 24.4 kg/m2 had an average upper arm muscle mass of 3,689.2 g and an average lower extremity muscle mass of 12,055.6 g. In a study performed by Chung et al. [27] on premenopausal and menopausal women (394 participants), the mean age of menopausal women was 56.9 years, the mean BMI was 23.0 kg/m2, and the upper arm and lower body muscle masses were 3,800.0 g and 11,600.0 g, respectively. In the present study, diabetic, menopausal female patients between 40 and 60 years of age with a BMI of 27.2 kg/m2 represented 81.9% of the total participants. The mean upper arm and lower body muscle masses were 4,054.0 g and 12,158.8 g, respectively. When the muscle mass/BMI ratio was examined, the upper body muscle mass was 2.9% to 9.7% lower than those in normal and menopausal women in the same age group, and the lower body muscle mass was 5.6% to 11.3% lower. Compared to the muscle mass/BMI ratio of the upper body and lower body results from previous studies, 45.5% (50 participants) of the upper body results from the present study and 63.6% (70 participants) of the lower body results did not meet the standards. When the mass of the upper arm muscle has high correlation with upper arm circumference, the corresponding standard upper arm circumference result from previous studies was 32.4 cm, and the upper arm/waist circumference ratio was 0.36. Therefore, the upper arm circumference in obese type 2 diabetic female patients was evaluated, and measurements less than 32.4 cm were assumed to be due to a lack of muscle mass. Such patients should receive education regarding combined strength exercises.
When resistance exercises are performed, the exercise intensity is based on the 1RM [28]. The current upper arm strength measurement is often measured according to strength [29-31]. However, among the numerous strength tests, Mathiowetz et al. [32] measured grip strength to represent hand strength and reported the test was necessary to assess the patient's ability to work. In the present study, a correlation between grip and upper arm strength was observed, but there was no correlation between grip and upper arm circumference. Thus, the authors of the present study believe there are limits to accurately measuring overall muscle strength of the upper arm through grip. Kim et al. [33] performed a study in which the maximum strength of male students in their 20s who had no prior strength exercise experience was estimated through upper arm and thigh circumferences. The bench press, which utilizes the pectoral and the triceps agonist muscle groups, has significant correlations with upper arm and forearm circumferences, and squat repetitions have been reported to be correlated with hip circumference. The measured chest press and leg press from the present study utilize the same agonist muscles involved in the bench press and squats. A correlation between upper arm circumference and thigh circumference was observed, and the results from the present study are consistent with existing studies. In addition, there was a correlation between maximum upper body strength and upper arm/waist circumference ratio and between maximum lower body strength and thigh/waist circumference ratio. Individuals with similar waist circumferences and larger upper arm and thigh circumferences tend to have higher maximum strengths. In the study by Kwon et al. [15] on female type 2 diabetes patients in their 50s, the mean maximum upper and lower body strengths were 17.8 kg and 89.8 kg, respectively, and the strength to weight ratios were 0.27 and 1.40, respectively. Using other studies as a standard for 1RM in upper and lower extremity, when compared with the present study, 44.0% (49 patients) and 50% (55 patients), respectively did not meet the criteria from previous studies. Assumed that the upper arm/waist circumference ratio related to 1RM of upper extremity was examined, the standard corresponding upper arm circumference from previous studies was 32.3 cm, and the upper arm/waist circumference ratio was 0.36. In other words, an upper arm circumference of 32.3 cm and an upper arm/waist circumference ratio less than 0.36 in female type 2 diabetes patients might be cutoff value of a lack in skeletal muscle mass, although 110 participants was not sufficient to determine it.
The primary goal of the present study was to determine and compare the relationship between muscle strength and muscle mass. For person with decreased maximum muscle strength, resistance exercise would be combined with aerobic exercise in order to increase muscle mass and muscle strength.
Therefore, in order to understand the anthropometric parameter, comparison of additional anthropometric measurements and prediction of muscle and adiposity on diabetes patients are required. Further research for resistance exercise methods in patients with lower extremity circumferences will be needed to increase muscle mass and strength.
Notes
No potential conflict of interest relevant to this article was reported.