Agreement between Framingham Risk Score and United Kingdom Prospective Diabetes Study Risk Engine in Identifying High Coronary Heart Disease Risk in North Indian Population
Article information
Abstract
Background
The aim of the study is to evaluate the concurrence between Framingham Risk score (FRS) and United Kingdom Prospective Diabetes Study (UKPDS) risk engine in identifying coronary heart disease (CHD) risk in newly detected diabetes mellitus patients and to explore the characteristics associated with the discrepancy between them.
Methods
A cross-sectional study involving 489 subjects newly diagnosed with type 2 diabetes mellitus was conducted. Agreement between FRS and UKPDS in classifying patients as high risk was calculated using kappa statistic. Subjects with discrepant scores between two algorithms were identified and associated variables were determined.
Results
The FRS identified 20.9% subjects (range, 17.5 to 24.7) as high-risk while UKPDS identified 21.75% (range, 18.3 to 25.5) as high-risk. Discrepancy was observed in 17.9% (range, 14.7 to 21.7) subjects. About 9.4% had high risk by UKPDS but not FRS, and 8.6% had high risk by FRS but not UKPDS. The best agreement was observed at high-risk threshold of 20% for both (κ=0.463). Analysis showed that subjects having high risk on FRS but not UKPDS were elderly females having raised systolic and diastolic blood pressure. Patients with high risk on UKPDS but not FRS were males and have high glycosylated hemoglobin.
Conclusion
The FRS and UKPDS (threshold 20%) identified different populations as being at high risk, though the agreement between them was fairly good. The concurrence of a number of factors (e.g., male sex, low high density lipoprotein cholesterol, and smoking) in both algorithms should be regarded as increasing the CHD risk. However, longitudinal follow-up is required to form firm conclusions.
INTRODUCTION
It is a well accepted fact that cardiovascular disease (CVD) risk factors such as smoking, dyslipidemia, and diabetes cluster together and interact multiplicatively to enhance vascular risk [12]. This understanding has led to the development of multivariable risk prediction models incorporating various risk factors and can be utilized by clinicians for assessing individual subject for the risk of developing CVD or specific components of CVD, i.e., coronary heart disease (CHD) [34], peripheral vascular disease [5], or stroke [6]. For example, the Framingham formulation [3] for predicting CHD was incorporated into the Third Report of the Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) [7]. The Framingham risk assessment tool has been validated in whites and blacks in the United States [8] and later modified so that they are valid to culturally diverse populations in Europe, the Mediterranean region [9] and Asia [10].
Type 2 diabetes mellitus (T2DM) is expanding in pandemic proportions worldwide and particularly in developing nations like India. Diabetes poses two to four times higher risk for developing CVD [11] as compared to general population. This perception headed to the development of diabetes specific multivariable risk prediction algorithms by different ethnic groups for efficient prevention and management [12]. The prognostic ability of these algorithms differs substantially among different populations [13]. For example, United Kingdom Prospective Diabetes Study (UKPDS) Risk Engine was developed based on large randomized controlled trial which showed that both in-tensive treatment of blood glucose and of blood pressure in diabetes can lower the risk of diabetes-related complications in individuals newly diagnosed with T2DM. This model also pro-vided the algorithm for CHD risk assessment specifically in subjects with T2DM [12].
Indians are considered ethnically to be a high-risk population both for T2DM and CVD [14]. However, no India specific predictive CVD risk score has been developed till date and we continue to use the risk models. In this context the present study is conducted to assess 10-year CHD risk in newly diagnosed T2DM patients using Framingham risk score (FRS) [3] which was developed in general population and UKPDS which is diabetes specific CVD risk engine [12].
METHODS
Study sample selection
Subjects for the present study are drawn out of the baseline cross-sectional data from an ongoing study that is aimed to assess the performance of FRS and UKPDS risk engine in a public tertiary care hospital in North India. The study proceeded following the approval from the Institute Ethics Committee (PGIMER, Chandigarh, India). Consecutive patients of either sex, aged 18 to 75 years visiting endocrinology outpatient clinic of the hospital and newly diagnosed with T2DM (≤6 months duration of diagnosis) were eligible for study enrolment. The patients were enrolled if they had necessary data in their medical files to calculate FRS and UKPDS and were also ready to be interviewed for additional parameters. All patients provided written informed consent before their recruitment in the study. Pregnant and lactating women and patients with prior CVD were excluded. The sociodemographic and clinical characteristics of patients were obtained from the medical records available with the subjects and behavioural factors by personal in-terviews.
Assessment of CHD risk using FRS and UKPDS risk engine
Ten-year CHD risk was calculated according to FRS and UKPDS risk engine. Baseline risk factors included in UKPDS risk engine includes age, sex, race, smoking status, glycosylated hemoglobin (HbA1c), systolic blood pressure (SBP), total cholesterol, and high density lipoprotein cholesterol (HDL-C). Baseline risk factors included in FRS includes age, sex, total cholesterol, HDL-C, SBP, diastolic blood pressure (DBP), smoking status and presence of diabetes. A risk score <10% is considered very low, 10% to 15% low, 15% to 20% moderate, and >20% reflects high 10-year risk of cardiovascular events [3]. To calculate coronary risk, the following variables were collected: age, sex, total cholesterol, HDL-C, SBP, DBP, and smoking history.
Blood pressure was measured using mercury sphygmomanometer as recommended in several guidelines. Blood tests were performed in venous blood, after at least 8 hours fasting, in reference laboratories in the hospital. Lipid profiles were evaluated in accordance with the recommendations of the Adult Treatment Panel III [7]. The proportion of high risk subjects on FRS with high risk cut off at 20% and the UKPDS risk engine at various cut-offs is calculated. The proportion of study subjects categorised into level of risk using both FRS chart and UKPDS risk engine were compared at 20% high risk cut-point and were analysed for the variables involved in discrepancy.
Statistical analysis
Data analysis was done by descriptive and analytic statistics using SPSS version 14.0 (SPSS Inc., Chicago, IL, USA). Agreement between the two charts was assessed using the κ statistic (κ<0.2, poor agreement; 0.21 to 0.40, fair agreement; 0.41 to 0.60, moderate agreement; 0.61 to 0.80, good agreement; and 0.81 to 1.0, very good agreement) [7]. Discrepancies between the two scales were analyzed using the Pearson chi-square test for categorical variables and the Student t-test for quantitative variables, based on estimates of normality and equality of variances.
A P value less than 0.05 was considered statistically significant and 95% confidence intervals calculated.
RESULTS
Patient characteristics
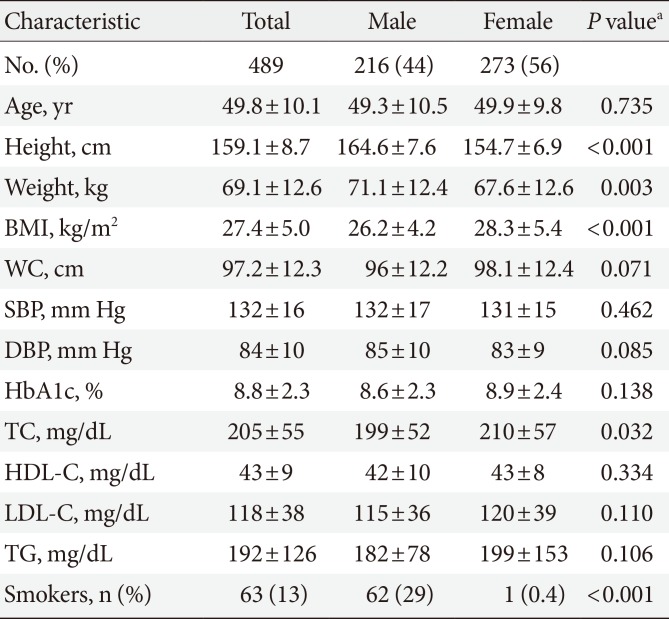
Of the 489 subjects included in the present study, the mean age±standard deviation was 49.8±10.1 years 56% were women and 13% were smokers, 14% had a history of hypertension. The mean SBP of the study cohort was 132±16 and diastolic 84±10 mm Hg. The mean FRS value was 15.1%, and the mean UKPDS risk engine score value was 13.4%. The baseline patient characteristics are shown in Table 1.

Sociodemographic and biochemical characteristics
Assessment of CHD risk status
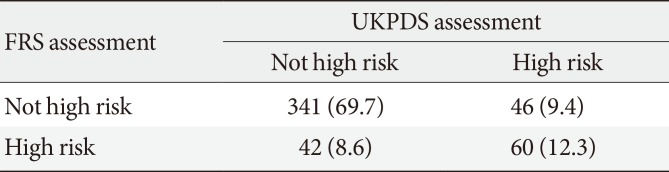
Using a threshold of 20%, 20.9% of the sample was classified as high risk using the FRS compared to 7.2% using UKPDS risk engine with cut-off at 30%. When a cut-point of 25% was used, the proportion of high risk subjects on the UKPDS risk engine increased to 12.7%. The proportion of high risk subjects on FRS with high risk cut off at 20% and the UKPDS risk engine at various cut-offs is shown in Fig. 1. The κ indices between the FRS and UKPDS risk engine are also shown. The κ index increased as the cut-point for high risk decreased on the UKPDS risk engine. The highest agreement was observed for a threshold of 20% of both the scores. At this cut-point, the number of high risk cases identified by the two scoring systems was found to be similar (P<0.001). Lowering the cut-point to 15% did not increase agreement between the two charts. Table 2 shows the distribution of the population into high risk and non-high risk groups using thresholds of 20% on both FRS and UKPDS risk engine. There was disagreement between the two scoring systems for 17.9% (14.7% to 21.7%) of cases (high risk on one scoring system but not on the other; κ=0.46 [0.36 to 0.56]). Of those, 9.4% were classified as high risk by UKPDS risk engine but not by FRS, and 8.6% were classified as high risk by FRS but not by UKPDS risk engine.
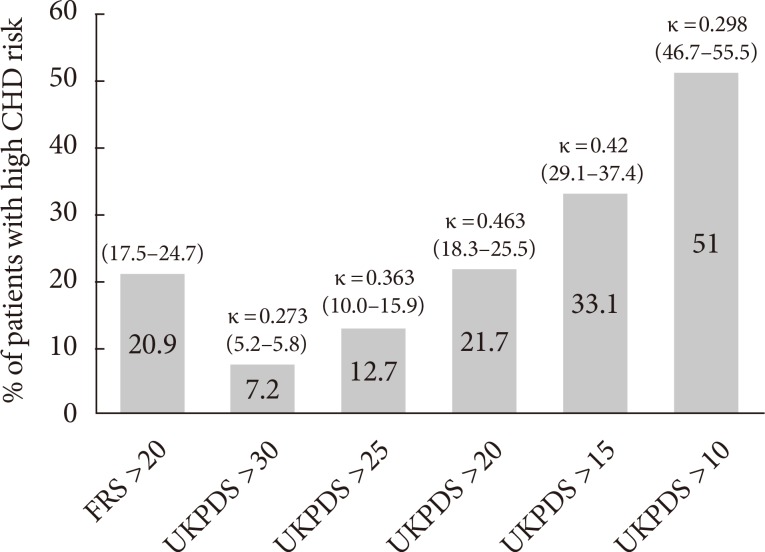
Percentage of patients classified as high risk by Framingham Risk score (FRS) and UKPDS, United Kingdom Prospective Diabetes Study (UKPDS) using different cut-points. CHD, coronary heart disease.

Distribution of subjects according to classification as high risk using FRS and UKPDS
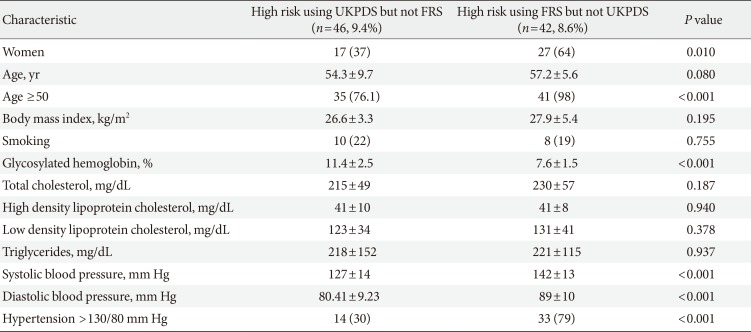
Table 3 shows the characteristics of the two groups in which there were discrepancies between the two instruments. Individuals classified as high risk on UKPDS risk engine but not on Framingham risk equation included a high percentage of males and cases with higher HbA1c levels than the group which classified as high risk with FRS but not on UKPDS risk engine. In the latter group, there were higher percentages of women and subjects with age ≥50 years. Also subjects had higher SBP and DBP values.

Characteristics of individuals with a discrepancy in coronary heart disease risk using FRS and UKPDS
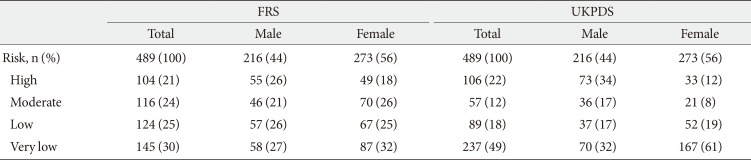
Table 4 shows the distribution of study subjects in various risk categories in detail from very low to high risk according to both the risk scoring systems. Using UKPDS more variation was observed in high risk category according to the gender, where 34% (n=73) are males and 12% (n=33) are females, while using FRS 26% (n=55) are males and 18% (n=49) are females. Though fair inter-rater agreement was observed between FRS and UKPDS scores (κ=0.27 [0.24 to 0.32]), large discrepancies are observed in very low, low, and moderate risk categories. While 49% of the study subjects are categorized as very low risk subjects according to UKPDS, only 30% subjects fell into very-low risk category according to FRS.

Comparison of estimated coronary heart disease risk scores according to FRS and UKPDS
DISCUSSION
In the present North Indian population study in individuals aged 18 to 75 years with no history of CVD and newly diagnosed with T2DM, the predicted results shows 21% and 22% of the study subjects having high risk of developing CHD in 10 years using FRS and UKPDS equations respectively. Only moderate agreement in identifying CHD risk was observed between FRS and UKPDS risk engine (using 20% cut-point).
We did not find significant difference in high risk category in FRS and UKPDS (21% [n=104] vs. 22% [n=106]). However, the actual patients identified by the two scoring systems are different. Although Table 4 suggests significant difference in 'very low risk group' of FRS and UKPDS; but it was definite only in women (32% vs. 61%), not in men (27% vs. 32%), it carries less importance since it's the high risk category that needs to be targeted and requires active intervention to prevent future mor-bidity and mortality.
Factors associated with individuals being classified as high risk using FRS but not UKPDS were low HbA1c, high blood pressure, particularly in elderly women; being classified as high risk by UKPDS but not by FRS was associated with being male and having a high HbA1c values or lower baseline SBP and DBP.
Compared to FRS, UKPDS may underestimate risk in patients with diabetes, low HbA1c, high blood pressure, particularly in elderly women. On the other hand, in comparison to UKPDS, FRS is likely to underestimate risk in young male patients with high HbA1c.
Agreement of the FRS and UKPDS risk engine
Using scoring algorithms to estimate CHD risk has its limitations. Comparative studies of the FRS and UKPDS have been done in various ethnic subgroups. In a cross-sectional study of 199 asymptomatic T2DM patients, Rakhit et al. [15] reported that area under the curves (AUCs) of the FRS and UKPDS risk engine were 0.61 and 0.56, respectively, with no significant difference between them. Guzder et al. [16] compared the pre-dictability of the FRS and UKPDS equations in 428 newly diagnosed T2DM patients in United Kingdom and reported that the AUCs of FRS and UKPDS were 0.657 and 0.670, respectively. In contrary to the above line of evidence, in a study by Simmons et al. [11] estimated 10-year CVD risk in the DM group as 37% and 33% using the FRS and UKPDS equations respectively.
In this study, we found that the estimated risk of developing CHD was more in males than in females which are similar to the findings of Hernaez et al. [17], where risk was higher in men. In general, males have a greater risk of CHD than females, but this observed gender difference gets diminished in T2DM patients [3181920].
A systematic review of 27 external validity studies found that the performance of the FRS differs significantly among different countries and ethnic groups. Predicted to observed ratios using FRS ranged from an under prediction of 0.43 in a high risk population, to over-prediction of 2.87 in low risk populations [21]. In our study UKPDS may have generated higher risk scores than FRS because it was developed for risk estimation in a population with diabetes, including important variables such as diabetes duration and HbA1c level, whereas the FRS was developed for general population.
Limitations
The main limitation of the study is its cross-sectional design meaning thereby the patients were not followed-up over time. Nevertheless, such a design is appropriate for assessing agreement between the scoring algorithms. Though the present study is being conducted using a rigorous methodology, the small sample size is yet another limitation.
Subjects in the study do not represent the national sample which is one of the limitations because in India there is no publically accessible database/registry. The present study is being conducted in largest tertiary care centre, i.e., PGIMER where patients from five different states covering entire Northern India visit the hospital. The present study is prospective study where each patient interfaced the researcher and was interviewed using structured questionnaire. Present manuscript is a part of larger project which aims at creating a new scoring system which will be useful for Indian patients.
Right now based on cross-sectional results we cannot comment on applicability of these algorithms in Indians, as Indians have been found to manifest CHD at lower body mass index [2223], waist circumference [2425], and total cholesterol levels relative to other ethnic groups [2627]. The results of this study with longitudinal follow-up may help in exploring these issues further to draw firm conclusions and recalibration of population-specific CVD risk prediction tools which will translate the findings into Indian context.
In conclusion, discrepancies in risk assessment and the identification of high risk individuals between the FRS and UKPDS risk engine (using a cut-point of 20%) have been observed. The two algorithms identify different populations as being at high risk. Defining the variables involved that resulted in discrepancies between the two algorithms can help in designing a new risk assessment tool which is valid for Indian population, which may help to improve the clinical assessment of CHD risk in patients with T2DM.
The importance of these findings and the impact of their application in clinical practice should be confirmed in future longitudinal studies.
ACKNOWLEDGMENTS
Authors are grateful to Ms. Harini Muthyala and Mr. Hari Prasad Esam for their assistance in data collection.
Notes
CONFLICTS OF INTEREST: No potential conflict of interest relevant to this article was reported.