Statin Discontinuation after Achieving a Target Low Density Lipoprotein Cholesterol Level in Type 2 Diabetic Patients without Cardiovascular Disease: A Randomized Controlled Study
Article information
Abstract
Background
This study investigated the rate of relapse of dyslipidemia and the factors which could predict relapse following a short-term statin discontinuation after achieving a target low density lipoprotein cholesterol (LDL-C) level in type 2 diabetic patients without cardiovascular disease (CVD).
Methods
Ninety-nine subjects on rosuvastatin treatment and whose LDL-C level was lower than 100 mg/dL were randomly assigned to discontinue or maintain statin treatment at a 2:1 ratio. The subjects were followed-up after 10 weeks. A relapse of dyslipidemia was defined as a reascent of LDL-C level to greater than 100 mg/dL.
Results
The statin discontinuation group had a significant rate of relapse compared to the maintenance group (79% vs. 3%, respectively). Pretreatment and baseline lipid levels, their ratios, and hemoglobin A1c level were significantly different between the relapse and nonrelapse groups. The pretreatment and baseline lipid profiles and their ratios were independently associated with relapse. The pretreatment LDL-C level was the most useful parameter for predicting a relapse, with a cutoff of 123 mg/dL. During the follow-up period, no CVD event was noted.
Conclusion
The relapse rate of dyslipidemia was high when statins were discontinued in type 2 diabetic patients without CVD. Statin discontinuation should be considered carefully based on the pretreatment lipid profiles of patients.
INTRODUCTION
The prevalence of dyslipidemia is increased in patients with type 2 diabetes, which contributes to their higher incidence of cardiovascular diseases (CVDs), resulting in higher morbidity and mortality than in nondiabetic subjects. The benefits of lipid-lowering therapy, mainly with statins (HMG CoA reductase inhibitors), in primary and secondary prevention have been well established by major trials [1-3]. Based on these evidences, recent guidelines now recommend stricter control of lipid levels. The American Diabetes Association recommends the use of statins by diabetic patients with overt CVD and by patients without CVD who are older than 40 years of age and have one or more CVD risk factors, regardless of baseline lipid level [4]. However, because there are no specific criteria for the discontinuation of statins, it is unclear whether statins should be administered throughout the patient's lifetime or if they can be withdrawn in some patients.
Several studies on subjects with acute coronary syndrome, ischemic stroke, or recipients of vascular surgery showed convincing evidence that statin discontinuation leads to adverse outcomes in these high-risk groups [5-9]. Furthermore, higher event rates and worse outcomes in subjects who discontinued statins compared with subjects without statin treatment [5-7] suggest the presence of a rebound phenomenon after statin withdrawal [10,11]. In contrast, the data from the Treating to New Target (TNT) study demonstrated that a 6-week discontinuation of statin therapy during a washout period in stable cardiac patients did not lead to an increased risk of acute coronary syndrome [12]. Therefore, whether the harmful effect of statin discontinuation extends to lower risk patients without CVD remains to be elucidated.
In this study, we investigated the rate of relapse following short-term statin discontinuation after achieving a target low density lipoprotein cholesterol (LDL-C) level in type 2 diabetic patients without a CVD history. We also determined the factors which could predict the relapse of dyslipidemia and the clinical outcome of statin discontinuation.
METHODS
Subjects and study design
After screening 110 patients, 99 patients with type 2 diabetes were enrolled in this randomized controlled study at a single center (Fig. 1). Subjects on 10 mg of rosuvastatin treatment whose LDL-C levels were between 100 and 160 mg/dL before the initiation of treatment (pretreatment) and who had achieved the ideal LDL-C level (lower than 100 mg/dL) at baseline were included. Subjects between 20 and 80 years of age with a hemoglobin A1c (HbA1c) lower than 10% were included. All of the subjects had normal hepatic, renal and thyroid functions, normal electrocardiographic findings, and no history of CVD, including coronary heart disease (CHD), stroke, or peripheral artery disease. The patients were regarded as having CHD if they had a history of angina pectoris or myocardial infarction or when significant stenosis (≥50%) in the coronary artery was observed by multidetector computed tomography or conventional angiography. Patients taking other classes of antihyperlipidemic agents, such as fenofibrate, ezetimibe, bile-acid binding resin or nicotinic acid, corticosteroids, or herbal medication were excluded. Eligible subjects were randomly assigned to either the statin discontinuation group or the maintenance group at a 2:1 ratio by permuted-block randomization using a computer-generated list of random numbers. After excluding five subjects due to consent withdrawal or lack of follow-up, 94 subjects (62 in the discontinuation group and 32 in the maintenance group) were included in the analysis. The subjects were followed up after 10±2 weeks for the clinical assessment and blood test. A reascent of LDL-C level to greater than 100 mg/dL was defined as a relapse of dyslipidemia. All of the subjects agreed to participate and provided oral and written consent. The Institutional Review Board of the Clinical Research Coordinating Center in St. Vincent's Hospital approved the study protocol (No. XC09OIMI0059V).
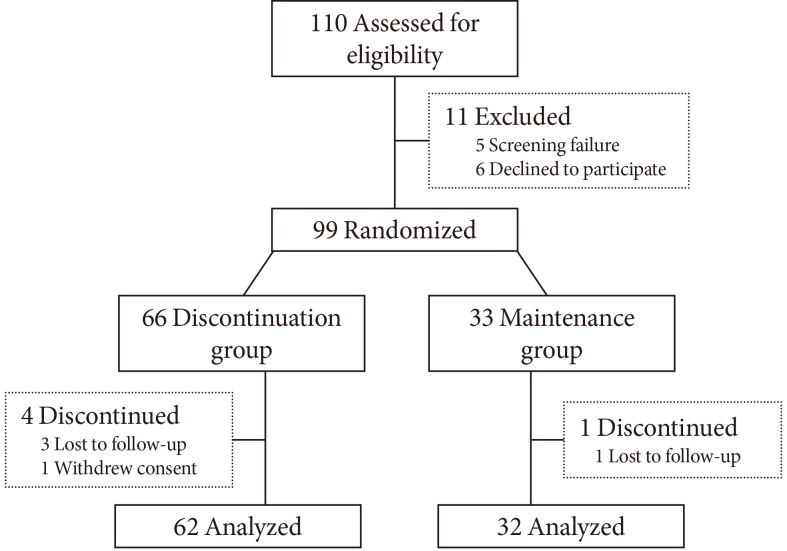
A flow diagram of the study.
Anthropometry and biochemical analysis
Body mass index (BMI) and waist-hip ratio (WHR) were calculated after anthropometric measurements. A whole body dual-energy X-ray absorptiometry (DEXA) scan was performed for a further analysis of body composition (Delphi-W; Hologic, Bedford, MA, USA). Blood samples were obtained on the days of randomization and follow-up, after the patients had fasted for at least 10 hours. Serum total cholesterol (TC) and triglyceride (TG) levels were measured using enzymatic colorimetric tests (Roche Diagnostics Corp., Indianapolis, IN, USA). High density lipoprotein cholesterol (HDL-C) levels were measured using a selective inhibition method (Daiichi, Tokyo, Japan), and LDL-C levels were measured using a direct enzymatic assay (Daiichi). Serum apolipoprotein B (ApoB) and apolipoprotein A1 (ApoA1) levels were measured by immunoturbidimetry (Daiichi). A clotting method with the Dade Thrombin reagent (Dade Behring Marburg GmbH, Marburg, Germany) was used for the measurement of fibrinogen. Serum insulin levels were measured using a chemiluminescent immunoassay kit (DPC, Los Angeles, CA, USA). Metabolic syndrome (MetS) was defined using the American Heart Association/National Heart, Lung, and Blood Institute criteria [13] with modifications in the waist circumference value (≥90 cm for men and ≥80 cm for women), according to the World Health Organization-Asian Pacific region criteria for abdominal obesity. The degree of insulin resistance was assessed by the homeostasis model assessment-insulin resistance [HOMA-IR=fasting insulin (µU/mL)×fasting plasma glucose (mg/dL)/405].
Statistical analysis
The sample size was calculated to provide a power of 80% and a level of significance of 5% to detect a relative risk for relapse of 3.0 in subjects with a baseline LDL-C level higher than 50 mg/dL. The relapse rate was assumed to be 80% in the discontinuation group, which was based on our previous observational data (unpublished).
The data are expressed as mean±standard deviation, as median (25th to 75th percentiles), or as proportion, except where noted. The odds ratio and 95% confidence interval were calculated when appropriate. The differences in the characteristics of the subgroups were compared using Student t-test or the chi-square test. For parameters showing nonnormal distributions (the duration of diabetes, duration of statin treatment, TG level, insulin level, and HOMA-IR), the Wilcoxon rank sum test was performed. Analysis of variance was used to compare lipid profiles among the subgroups. Pearson or Spearman correlation analysis was performed to examine the factors associated with ΔLDL-C after statin discontinuation. A multivariable logistic regression analysis was used to test for the factors that were independently associated with the relapse of dyslipidemia after statin discontinuation. Among various models tested, the most appropriate model was decided by analyzing model fit statistics. Receiver operating characteristics (ROC) analysis was applied to determine the optimal cutoff value for the parameters in order to detect the relapse of dyslipidemia after statin discontinuation. The values that resulted in a maximal Youden J-index (sensitivity+specificity-1) were defined as optimal. A P<0.05 was considered significant. Statistical analyses were performed using SAS version 9.01 (SAS Institute, Cary, NC, USA).
RESULTS
Baseline characteristics
The mean age and BMI of the participants were 55.3±8.0 years and 25.2±2.7 kg/m2, respectively. Of the subjects, 50% were men, and 76.6% had MetS. The mean HbA1c level was 7.4%±1.0%. The median (25th to 75th percentiles) duration of statin treatment was 12 months (range, 9 to 15 months). Table 1 shows the baseline characteristics of the patients and a comparison between the discontinuation group and the maintenance group. There were no significant differences in age, gender distribution, duration of diabetes, BMI, WHR, duration of statin treatment, or body composition between the groups. HbA1c levels were significantly higher in the maintenance group. Although the pretreatment TC and TG levels were significantly higher in the discontinuation group, there were no differences in the baseline lipid profiles between the groups.
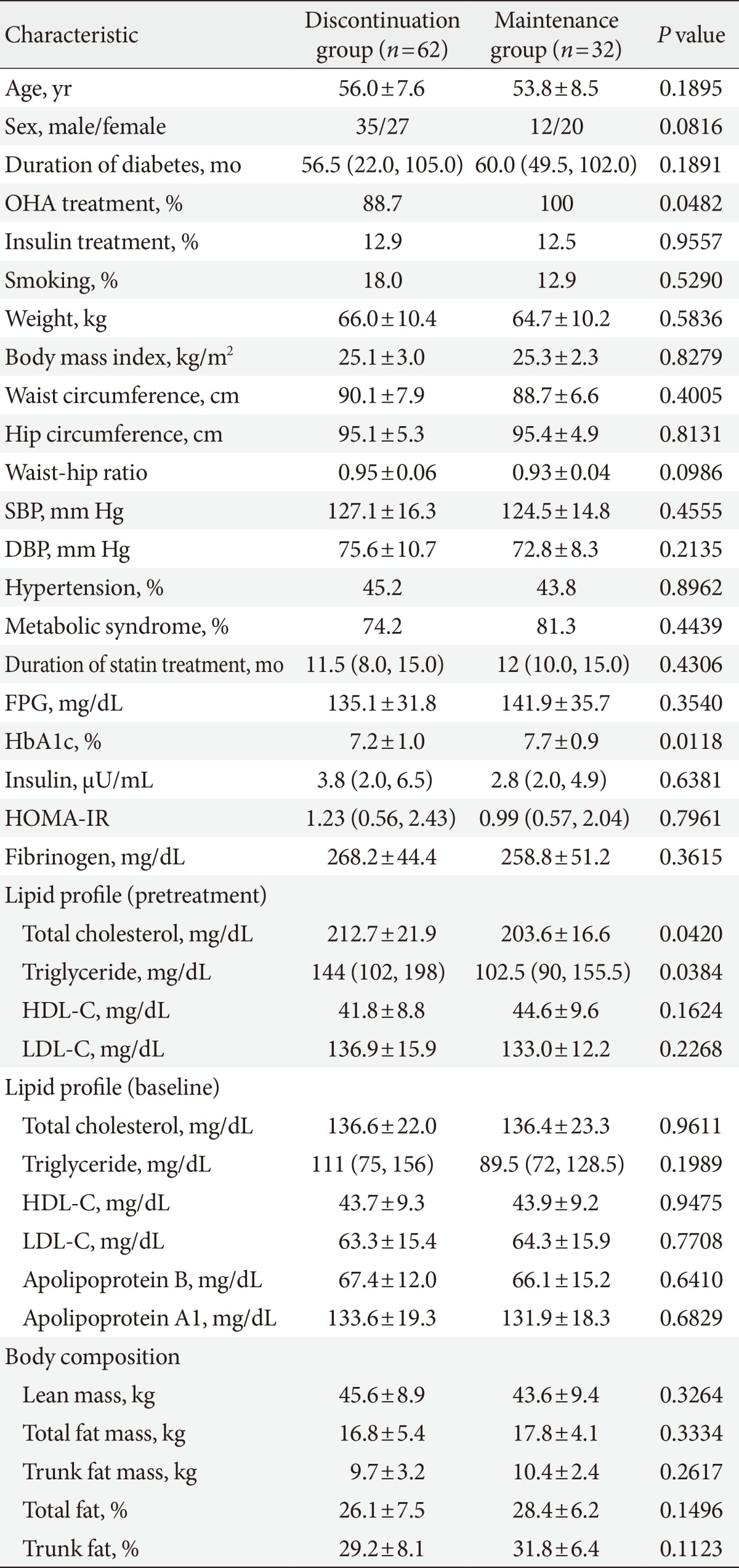
The baseline characteristics of the study subjects
The relapse rate of dyslipidemia and a comparison between the relapse and nonrelapse groups after statin discontinuation
Of the 62 subjects assigned to the discontinuation group, 49 subjects had an LDL-C level higher than 100 mg/dL at the follow-up examination, which indicated a 79% rate of relapse. In contrast, only one subject of 32 (3%) in the maintenance group had an elevated LDL-C level, which demonstrated a significant difference in the relapse rate between groups (P<0.0001). When the clinical characteristics of the relapse and nonrelapse groups were compared, the pretreatment LDL-C levels, baseline LDL-C levels, and baseline ApoB levels were significantly higher and the pretreatment HDL-C levels were significantly lower in the relapse group (Table 2, Fig. 2). As a result, the pretreatment LDL/HDL-C ratios (3.62±0.76 vs. 2.65±0.51; P<0.0001), baseline LDL/HDL-C ratios (1.63±0.42 vs. 1.04±0.29; P<0.0001), pretreatment TC/HDL-C ratios (5.48±1.06 vs. 4.51±0.80; P=0.0032), baseline TC/HDL-C ratios (3.31±0.62 vs. 2.86±0.65; P=0.0247), and baseline ApoB/ApoA1 ratios (0.54±0.10 vs. 0.41±0.07; P<0.0001) were also significantly higher in the relapse group than in the nonrelapse group, respectively (Fig. 3). HbA1c levels and fibrinogen levels were also significantly higher in the relapse group. However, there were no differences in the degree of insulin resistance as measured by fasting insulin level and HOMA-IR or in the proportion of MetS or adiposity as assessed by DEXA, which are the parameters closely related to dyslipidemia.
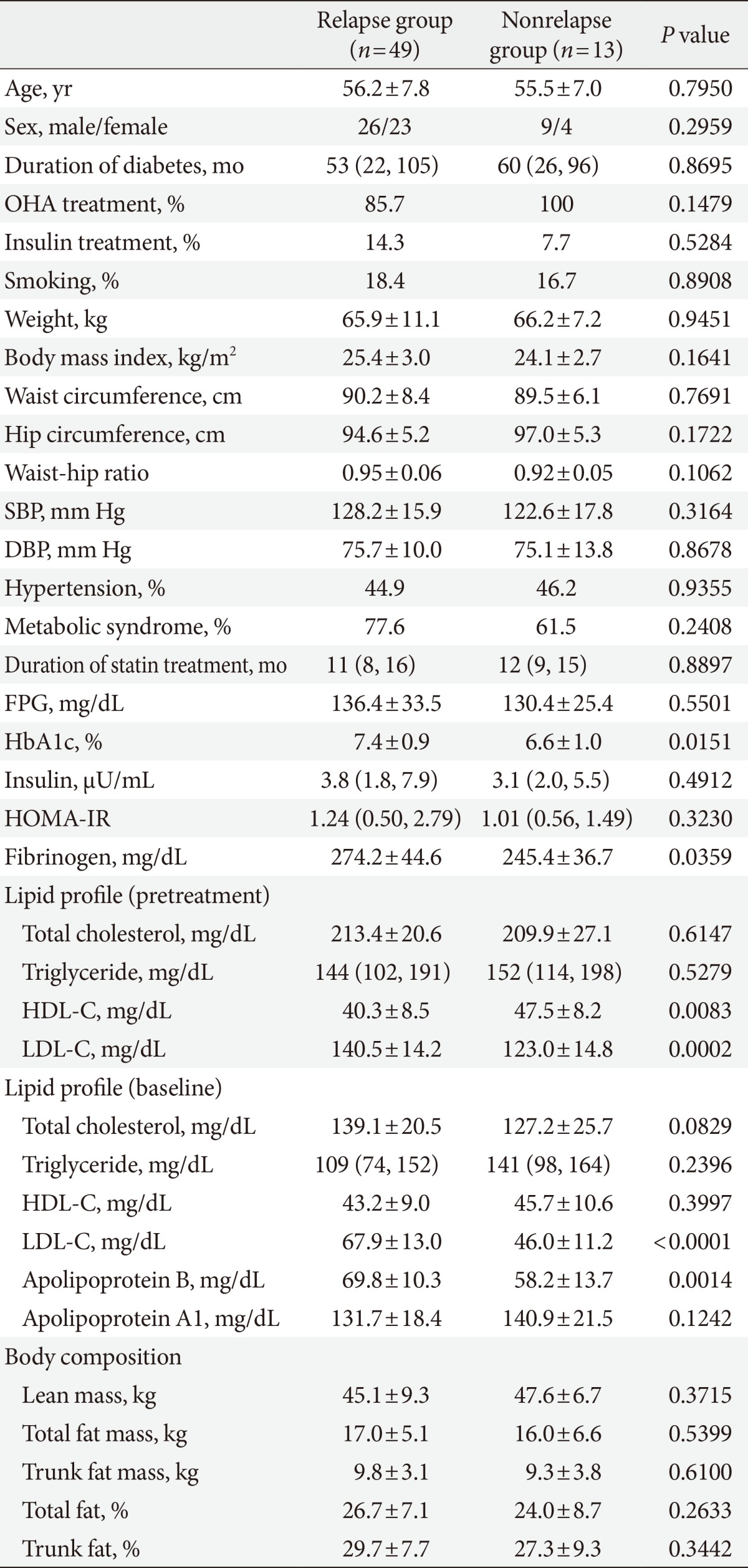
A comparison between the relapse versus nonrelapse groups after statin discontinuation
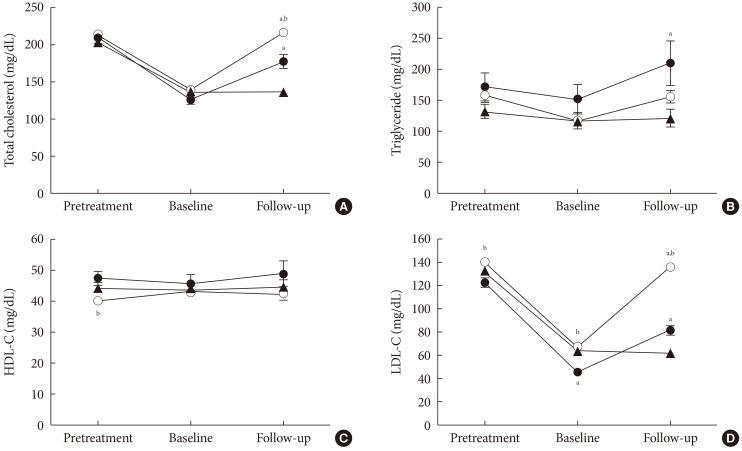
Changes in lipid profiles. (A) Total cholesterol, (B) triglycerides, (C) HDL-C, and (D) LDL-C. The maintenance group is represented by triangles; the discontinuation, nonrelapse group is represented by black circles; and the discontinuation, relapse group is represented by white circles. Values are presented as mean±standard error. HDL-C, high density lipoprotein cholesterol; LDL-C, low density lipoprotein cholesterol. aP<0.05 vs. the maintenance group, bP<0.05 vs. the discontinuation, nonrelapse group.
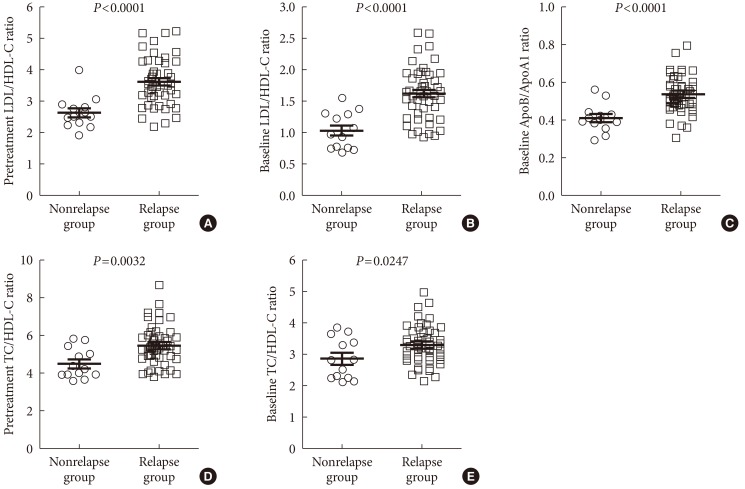
Comparison of lipid profiles between the relapse and the nonrelapse groups after statin discontinuation. (A) Pretreatment LDL/HDL-C ratio, (B) baseline LDL/HDL-C ratio, (C) baseline ApoB/ApoA1 ratio, (D) pretreatment TC/HDL-C ratio, and (E) baseline TC/HDL-C ratio. Values are presented as scatter dot plots and mean±standard error. LDL-C, low density lipoprotein cholesterol; HDL-C, high density lipoprotein cholesterol; ApoB, apolipoprotein B; ApoA1, apolipoprotein A1; TC, total cholesterol.
Next, the lipid profiles at the follow-up visit were compared. TC and LDL-C levels of the discontinuation, nonrelapse group had risen and were significantly higher than those of the maintenance group (TC, 177.7±9.1 mg/dL vs. 137.0±3.9 mg/dL; LDL-C, 81.9±4.1 mg/dL vs. 62.6±2.7 mg/dL, respectively) but were still significantly lower than those of the discontinuation, relapse group (TC, 216.7±4.2 mg/dL; LDL-C, 136.2±3.2 mg/dL). The ΔTC (77.5±3.5 mg/dL vs. 50.5±9.6 mg/dL; P=0.0018) and ΔLDL-C (68.3±2.7 mg/dL vs. 35.9±6.7 mg/dL; P<0.0001) after statin discontinuation were also significantly higher in the relapse group compared to the nonrelapse group, respectively. TG level was also increased in both the relapse and nonrelapse groups, but the difference was not significant (follow-up value, 156.3±10.4 mg/dL vs. 210.3±35.8 mg/dL; ΔTG, 38.7±8.2 mg/dL vs. 57.6±32.3 mg/dL, respectively). No significant differences were noted for the follow-up HDL-C levels among the groups (all are mean±standard error) (Fig. 2).
The factors associated with a relapse of dyslipidemia after statin discontinuation
The ΔLDL-C was significantly correlated with pretreatment LDL-C level (r=0.34, P=0.0065), pretreatment LDL/HDL-C ratio (r=0.27, P=0.0324), and baseline fibrinogen level (r=0.29, P=0.0207). Various models of multivariable logistic regression analysis showed that the pretreatment and baseline lipid levels and their ratios were independently associated with a relapse of dyslipidemia after adjustment for age, sex, BMI, oral hypoglycemic agent treatment, WHR, fibrinogen level, and HbA1c value (Table 3). Among the models tested, model 1 was considered to be the most appropriate with the lowest values of Akaike information criterion and Schwarz criterion by model fit statistics. Therefore, we concluded that higher pretreatment LDL-C and lower pretreatment HDL-C level are the most important factors associated with a relapse of dyslipidemia.
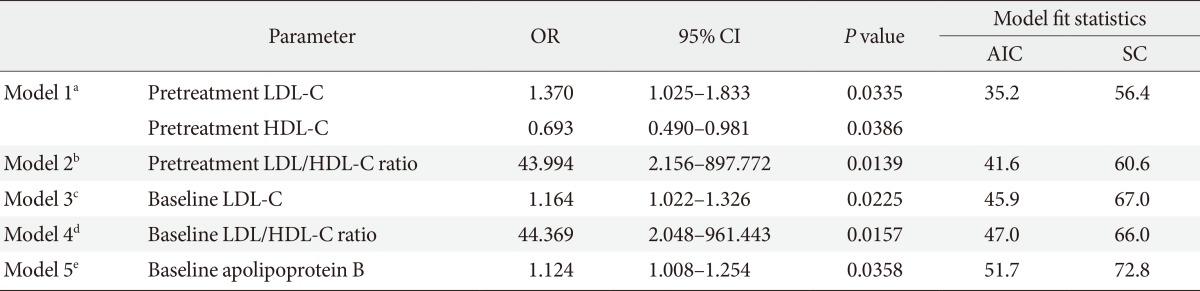
Multivariable logistic regression models used to assess the independent factors associated with relapse after statin discontinuation
The optimal cutoff values of parameters for detecting a relapse of dyslipidemia after statin discontinuation
The optimal cutoff values that produced the maximum sensitivity and specificity for detecting a relapse of dyslipidemia from the ROC analysis were 123 mg/dL for the pretreatment LDL-C level and 38 mg/dL for the pretreatment HDL-C level. The pretreatment LDL-C level was the most useful parameter with the highest area under the curve for the ROC and the J-index (Table 4).

The optimal cutoff values of variables to detect relapse of dyslipidemia after statin discontinuation
The clinical outcome of statin discontinuation
There were no symptomatic CVD events according to history in either the discontinuation group or the maintenance group after an approximate 10-week intervention.
DISCUSSION
In this study of type 2 diabetic patients without a CVD history, we show that statin discontinuation after achieving a target LDL-C level leads to a significant relapse rate of dyslipidemia. Pretreatment LDL and HDL-C levels were independently associated with relapse. Pretreatment LDL-C was the most useful parameter for predicting a relapse in these subjects. During the short follow-up period, no CVD events were noted.
There is compelling evidence that statin discontinuation after an acute vascular event has detrimental effects. A population-based cohort study involving survivors of an acute myocardial infarction demonstrated that the discontinuation of statin therapy was associated with significantly higher 1-year mortality [5]. Heeschen et al. [6] confirmed that statin discontinuation increased the risk of death and nonfatal myocardial infarction in patients with acute coronary syndrome during a 30-day follow-up period. Studies on the outcomes of ischemic stroke patients also showed harmful effects of statin discontinuation. A randomized controlled study of 89 patients with chronic statin treatment suggested that even a short-term withdrawal during an acute phase of the disease could result in a significant increase in morbidity and mortality. Statin discontinuation for the first 3 days after admission was associated with increased risk of death, dependency, early neurologic deterioration, and infarct volume [7]. Another study on stroke survivors found that statin discontinuation significantly increased and was an independent predictor of 1-year mortality [8]. Patients undergoing aortic or lower extremity vascular surgery also experienced a higher risk of perioperative cardiac events when statins were discontinued, which was mainly due to an inability to take oral medications [9]. These data emphasize the importance of maintaining statin therapy in patients with an acute CVD or CVD history. However, one study comparing the CVD event rate during a washout period and a subsequent open-label treatment period in the TNT study found no increase in acute coronary syndrome after statin discontinuation in stable cardiac patients [12]. Our study found that there were no discernible CVD events in patients with relatively well-controlled type 2 diabetes and with no CVD history during the ten weeks of statin discontinuation.
Because outcome studies on statin discontinuation in low-risk subjects are lacking, it is controversial whether statin treatment should be maintained throughout a patient's lifespan once a subject has been diagnosed with dyslipidemia. Some evidence supporting the continuous administration of statins is as follows. First, it is generally accepted that the lowest LDL-C level possible is better for patients with CVD [14-16], although it remains to be proven whether this notion is also relevant to subjects without CVD. Second, statin discontinuation may induce a rebound phenomenon [10,11] that abrogates beneficial pleiotropic effects, such as an improvement in endothelial dysfunction, increased bioavailability of nitric oxide, plaque stabilization, and anti-inflammatory and antioxidant effects [17]. Third, a recently published Finnish nested case-control study using a nationwide health database showed that adherence to statin treatment was associated with a reduced incidence of major coronary events irrespective of prior CHD in diabetic patients. However, the lack of data on glycemic control, aspirin use, and lifestyle factors and the method of assessing adherence by a dispensed prescription should be considered in the interpretation of this result [18]. Conversely, unfavorable aspects of an intensive statin treatment also need to be considered. In the TNT study, treatment with 80 mg of atorvastatin was associated with a persistent increase in aminotransferase level compared to treatment with 10 mg [14]. A dose-dependent effect on liver dysfunction was noted in another large population-based cohort study [19]. A meta-analysis of five statin trials showed that intensive-dose statin therapy was associated with an increased risk of new-onset diabetes compared with moderate-dose statin therapy [20]. The association between statin treatment and acute renal failure or myopathy is also a point of concern [19]. In addition, a significant association between the risk of cancer and an achievement of lower LDL-C level was observed in large randomized trials [21]. The different susceptibilities to CVD and the LDL-C levels that show a benefit of statin treatment in Asian populations also suggest the necessity of a differential approach between ethnicities [22].
The compliance to statin therapy is known to be low in clinical practice [23-26]. The discontinuation rate was shown to be high in the first year of treatment, and long-term adherence was poor, especially in subjects with fewer cardiovascular risk factors [26] and when used for primary prevention [25]. Based on the data mentioned above [5-9], the importance of maintaining this agent should be emphasized, especially in patients with a history of acute vascular events. For lower risk patients, it would be more effective if we could predict the possibility of a relapse of dyslipidemia after discontinuing statin use. Our data show that the pretreatment and baseline lipid profiles and their ratios were closely associated with a relapse of dyslipidemia in this study's population. Pretreatment LDL-C and HDL-C levels, baseline LDL-C level, baseline ApoB level, pretreatment LDL/HDL-C ratio, and baseline LDL/HDL-C ratio were independently associated with relapse, although this was dependent on the logistic regression model used. Among these various parameters, the most appropriate model indicated that pretreatment LDL and HDL-C levels were the most powerful predictors of relapse with cutoffs of 123 and 38 mg/dL, respectively. A study demonstrating that the benefits of intensive lipid-lowering therapy progressively decreased as the pretreatment LDL-C level declined supports the role of pretreatment lipid level in determining statin therapy [27]. Because the relapse rate was high in our subjects, we believe that the discontinuation of statins should be carefully determined based on lipid profile, lipid ratio, and whether patients have any side effects to statin treatment.
There are unresolved questions that need to be further elucidated. It is unknown whether the relapse rate after discontinuation is different among the various statins that have diverse potencies. It is also controversial whether the elevation of lipid level after statin discontinuation is an acute process that occurs within a few days [28-30]. Related to this, the biochemical and clinical outcomes of a long-term statin discontinuation remain undetermined.
Since substantial data indicate that dietary lipid intake influences serum levels of cholesterol and lipoproteins [31], the lack of information on the diets and exercise patterns of the subjects during the trial period is a limitation of this study. In addition, we cannot exclude the possibility of subtle preclinical changes after statin discontinuation because CVD events were evaluated symptomatically. In this context, there might be different CVD outcomes with long-term follow-up of participants after statin discontinuation.
In summary, the relapse rate of dyslipidemia was high when statins were discontinued after achieving a target LDL-C level in type 2 diabetic patients without CVD. To predict a relapse of dyslipidemia, pretreatment LDL and HDL-C levels might represent easy and useful parameters. However, the long-term clinical outcomes of statin discontinuation and the pros and cons of an intensive statin treatment in low-risk subjects need further investigation.
ACKNOWLEDGMENTS
The authors wish to thank Kyung-Mi Shin, RN and Mi-Jin Shim, RN for their excellent support in the study procedure.
Notes
No potential conflict of interest relevant to this article was reported.