Association of Snoring with Prediabetes and Type 2 Diabetes Mellitus: The Cardiovascular and Metabolic Diseases Etiology Research Center Cohort
Article information

Abstract
Background
Evidence suggests that habitual snoring is an independent risk factor for poor glycemic health. We examined the associations between snoring with prediabetes and diabetes in Korean population.
Methods
Self-reported snoring characteristics were collected from 3,948 middle-aged adults without prior cardiovascular diseases. Multivariable linear regression assessed the association of snoring intensity, frequency, disruptiveness, and disrupted breathing with fasting glucose and glycosylated hemoglobin (HbA1c) level. Then, multinomial regression evaluated how increasing snoring symptoms are associated with the risk for prediabetes and diabetes, adjusting for socioeconomic and behavioral risk factors of diabetes, obesity, hypertension, and other sleep variables.
Results
Higher snoring intensity and frequency were positively associated with fasting glucose and HbA1c levels. Participants presenting the most severe snoring were at 1.84 times higher risk (95% confidence interval [CI], 1.09 to 2.29) for prediabetes and 2.24 times higher risk (95% CI, 1.84 to 2.95) for diabetes, compared to non-snorers. Such graded association was also observed amongst the most frequent snorers with higher risk for prediabetes (odds ratio [OR], 1.78; 95% CI, 1.29 to 2.22) and diabetes (OR, 2.03; 95% CI, 1.45 to 2.85). Disruptive snoring (OR, 1.60; 95% CI, 1.12 to 2.28) and near-daily disruptive breathing (OR, 2.18; 95% CI, 1.02 to 4.19) were associated with higher odds for diabetes. Such findings remained robust after additional adjustment for sleep duration, excessive daytime sleepiness, unwakefulness, and sleep-deprived driving.
Conclusion
Snoring is associated with impaired glucose metabolism even in otherwise metabolically healthy adults. Habitual snorers may require lifestyle modifications and pharmacological treatment to improve glycemic profile.
INTRODUCTION
A growing body of epidemiological evidence suggests that habitual snoring is an important risk factor for the development and exacerbation of cardiovascular and metabolic complications, including type 2 diabetes mellitus [123]. Considering that snoring is the most common and salient symptom of obstructive sleep apnea (OSA) [4], it is consistently associated with both high prevalence and incidence of type 2 diabetes mellitus among otherwise healthy adults [5]. Poor glycemic control amongst snorers prevails, even after accounting for other sleep-related conditions, such as extreme sleep duration, excessive daytime sleepiness, and chronic fatigue [67891011].
Considering that good sleep quality is essential to maintain normal physiological function to regulate normal somatic, cognitive, and psychological processes, it is important to examine the extent which snoring is associated with glycemic maintenance. The recent Korean statistics showed that among adults 30 years or older, prevalence of prediabetes is 25.3% and 14.4% for type 2 diabetes mellitus; their pervasiveness escalated drastically with older age [12]. Considering that both prediabetes and diabetes populations are at increased risk for microvascular (chronic kidney disease, neuropathies, and retinopathy) and cardiovascular diseases (CVD) [13], early detection and management of glycemic disorder are crucial.
Whether various characteristics of snoring are associated with elevated risk of both prediabetes and type 2 diabetes mellitus is not well-established in the general population. Moreover, previous studies primarily utilized a single marker of sleep-disordered breathing rather than incorporating comprehensive aspects of sleep. Given the poor prognostics of uncontrolled glycemic state in regard to the CVD progression, investigating whether snoring can be indicative of adverse glycemic state may aid in identifying high-risk or already prevalent individuals for prediabetes and diabetes. In this context, the objective of this study is to examine the association of various characteristics of snoring with prediabetes and type 2 diabetes mellitus, independent of other sleep characteristics among community-dwelling Korean adults. We hypothesized that individuals presenting higher severity (louder sound and greater disruptiveness) and frequency of snoring will have positively graded risk for prediabetes and type 2 diabetes mellitus, compared to non-snoring participants.
METHODS
Study population
The Cardiovascular and Metabolic Diseases Etiology Research Center (CMERC) Study has been approved by the Institutional Review Boards of Severance Hospital, Yonsei University Health System, Seoul, Korea (4-2013-0661). Written informed consent has been obtained from all participants prior to the baseline survey. Participants were ensured that they can withdraw from the study at any time, regardless of its cause, without any repercussions.
The study participants consisted of healthy community-dwelling capital residents of Republic of Korea, between the age of 30 to 64 years, who were enrolled in the CMERC cohort. Briefly, the CMERC study aimed to identify novel risk factors and to investigate distribution and effects of known cardiac and metabolic diseases risk factors, ultimately to develop improved CVD prediction tools for the general Korean population [14]. Adhering to standardized protocols, trained researchers collected detailed information on socioeconomic status, health behaviors, disease history, nutrition, and psychosocial characteristics and performed blood and urine tests [14]. In the present study, among 4,060 participants who have undergone baseline examination at the CMERC center 1 between 2013 and 2018, participants either currently undergoing cancer treatment, diagnosed with heart failure or angina pectoris, or missing information on glycemic index were excluded, yielding 3,948 participants (1,800 male and 2,548 female) for the final analysis.
Assessment of exposure
A face-to-face interview obtained information on snoring and other sleep-related variables based on the Korean version of the Berlin Questionnaire [15]. Briefly, the Berlin Questionnaire is one of the most widely and readily used screening tools for OSA. In reference to polysomnography results, previous validation studies confirmed its sensitivity of 84.4% and specificity of 35.3% in both general population and sleep clinic patient-based studies [1617]. Another systematic review confirmed that among sleep clinic patients or self-reported habitual snorers, the Berlin Questionnaire showed substantial OSA predictability, with sensitivity and specificity as high as 81% and 80%, respectively [1819]. Considering that in-laboratory polysomnography, currently the gold standard tool for OSA diagnosis, is infeasible for large-scale epidemiologic studies, Berlin Questionnaire collects sleep behavior in cost- and time-efficient manner. In this study, participants were inquired whether they are a habitual snorer. If affirmative, they were subsequently asked to rate their snoring frequency: never or rare, seldom (1 to 2 time/month), sometimes (1 to 2 time/week), often (3 to 4 time/week), or frequent (almost every night). The following question on sleep-disordered breathing (“Has anyone noticed that you quit breathing during your sleep?”) was evaluated in the same manner. The respondents rated the intensity of their snoring: slightly louder than breathing, as loud as talking, louder than talking, or very loud (can be heard in adjacent rooms). Lastly, participants were inquired whether own snoring has bothered bed partners); the answer was dichotomized to either a “yes” or a “no.”
To simultaneously account for other various sleep-related factors, participants were additionally asked to report their weekday/workday sleep duration in exact hours and minutes, subsequently categorized into ≤5, 6, 7, 8, or ≥9 hours. Frequency of unwakefulness (fatigue after waking up), excessive daytime sleepiness (feeling tired or fatigued during day/active time), and history of sleep-deprived driving were also inquired.
Based on the responses to the aforementioned questions, we identified five sleep variables: snoring (frequency/intensity/disordered breathing/disruptiveness), sleep duration, unwakefulness, excessive daytime sleepiness, and sleep-deprived driving. Our primary analysis focused on various characteristics of snoring, accounting for other aforementioned sleep variables.
Assessment of glycemic profile
Participants underwent blood test after overnight fasting for a minimum of 8 hours. Fasting plasma glucose levels were assessed using colorimetry method (ADIVA1800 Auto Analyzer; Siemens medical Sol., Deerfield, IL, USA) and glycosylated hemoglobin (HbA1c) was analyzed using high-performance liquid chromatograph (Variant II Turbo Hemoglobin Testing System; Bio-Rad, Irvine, CA, USA).
Prediabetes was defined as a fasting glucose level between 100 mg/dL and 125 mg/dL or HbA1c level between 5.7% and 6.4%. Type 2 diabetes mellitus was defined as fasting glucose level ≥126 mg/dL, HbA1c ≥6.5%, a self-reported physician-diagnosis, or current use of oral glucose-lowering drugs or insulin injection. The CMERC study did not collect sufficient information (e.g., C-peptide levels) enough to identify every subtype previously diagnosed; however, the entailed information regarding history of autoimmune or other chronic diseases, thereby able enabled us to distinguish between type 2 diabetes mellitus and other types of diabetes, such as type 1 diabetes mellitus or maturity onset diabetes of the young.
Assessment of covariates
Demographics, health-related behaviors, and disease history were obtained via face-to-face interview. Household income was categorized into cohort-specific quartile. Longest held and current occupation were classified into white or blue collar or unemployed. Education level was categorized into four groups: elementary school or below, middle school, high school, or college/university. Physical activity was assessed by the Korean version of the International Physical Activity Questionnaire standard [20]. The total metabolic equivalent of task was then categorized into quartile. Alcohol consumption and cigarette smoking were divided into non-, previous-, and current drinker/smoker. Information on familial and personal morbidity history included the age at first diagnosis of common chronic diseases, such as hypertension, diabetes mellitus, and so on. Accordingly, participants presented prescription records entailing previous and current treatment status, including types of oral hypoglycemic medications or insulin injection.
Height was measured to the nearest 0.1 cm using stadiometers (DS-102; Jenix, Seoul, Korea), and weight was measured to the nearest 0.1 kg on a digital scale (DB-150; CAS, Seongnam, Korea). To minimize measurement variability, a zero-point adjustment was routinely conducted using a standard ruler (170 cm) and weights (20, 40, and 60 kg). Body mass index (BMI) was calculated as a ratio of weight in kilograms to height in squared meters. We defined obesity as BMI ≥25 kg/m2 based on the Asia-Pacific classification from the World Health Organization guideline [21]. Blood pressure (BP) was consecutively measured using both single- and double-arm automated oscillometric device (HEM-7080 and HEM-9000 AI; Omron Health, Matsusaka, Japan) at a single sitting; the mean of second and third measurements was adopted for analysis. Hypertension was defined as systolic BP ≥140 mm Hg, diastolic BP ≥90 mm Hg, self-reported physician-diagnosis, or current use of antihypertensive medication.
Statistical analysis
We compared anthropometric, socioeconomic, lifestyle, and morbidity characteristics of the participants across healthy glycemic (“normal”), prediabetes, and type 2 diabetes mellitus groups using one-way analysis of variance. Next, we employed multivariable linear regression model to assess the association between individual dimension of snoring and fasting glucose level and HbA1c concentration, separately. Then, to examine whether snoring and its subcomponents are associated with increased risk of prediabetes and type 2 diabetes mellitus, we employed multivariable multinomial logistic regression to compare associations among normal, prediabetes, and type 2 diabetes mellitus groups. All results are presented in odds ratio (OR) and 95% confidence interval (95% CI).
We selected potential confounders based on a review of the literature and logical assessment of potential causal relationships accounting for biological plausibility. In the first model, we adjusted for age and sex. In the second model, we additionally adjusted for BMI, hypertension prevalence, and socioeconomic status, including education level, household income, and longest held occupation. In the third model, we additionally adjusted for well-known cardiovascular and metabolic behavioral risk factors, including current smoking and drinking status and physical activity. To account for residual confounding even after adjusting for BMI and hypertension prevalence, subgroup analyses were done by further stratifying by obesity and hypertension status. To further explore whether the effect of snoring was independent of other sleep conditions, we simultaneously adjusted for all sleep-related variables, including sleep duration, unwakefulness, excessive daytime sleepiness, and sleep-deprived driving.
Hosmer-Lemeshow goodness of fit for logistic regression ensured appropriateness of the model. All statistical tests were two-sided, and the statistical significance was set at a P value <0.05. All analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA).
RESULTS
Among 3,893 participants, 1,224 (31.4%) participants had prediabetes and 355 participants (9.1%) had type 2 diabetes mellitus. Table 1 compares the general characteristics of the study population across normoglycemic, prediabetes, and type 2 diabetes mellitus groups. Compared to normoglycemia group, prediabetes and type 2 diabetes mellitus groups were older and higher proportion of male sex, current smoker, obesity, and hypertension. Furthermore, there were significant differences in education level, household income, and drinking history among the three groups. Participants with type 2 diabetes mellitus had the highest proportion of habitual snorer (76.5%), followed by prediabetes group (73.2%) and lastly, the normal group (59.9%).

General characteristics of the study population (n=3,948)
Table 2 presents age- and sex-adjusted mean comparison of fasting glucose and HbA1c levels by level of each snoring characteristics. Compared to their non-snoring counterpart, participants who habitually snore had higher fasting glucose (92.5 mg/dL vs. 88.2 mg/dL) and HbA1c (5.7% vs. 5.6%) levels. Both indices were incrementally higher with increasing snoring intensity, frequency, disruptiveness, and disrupted breathing.

The mean level of fasting glucose and HbA1c by characteristics of snoring (n=3,948)
Table 3 illustrates results from the multivariable linear regression of individual snoring characteristics with fasting glucose and HbA1c level. For each sleep variable dimension, the estimates are obtained in reference to the lowest categorical level; for instance, the analyses on snoring frequency are in reference to the “never or rare” category. In prediabetes group, higher snoring intensity (β=1.20 mg/dL, P=0.001), frequency (β=0.99 mg/dL, P=0.008), and bothersome snoring (β=0.96 mg/dL, P=0.007) were positively associated with fasting glucose level. Similar direction and magnitude of association were observed in type 2 diabetes mellitus group. Likewise, regardless of glycemic status, higher intensity, frequency, and disruption were also positively associated with HbA1c levels. Such trend remained robust after stratification by sex (Supplementary Table 1).
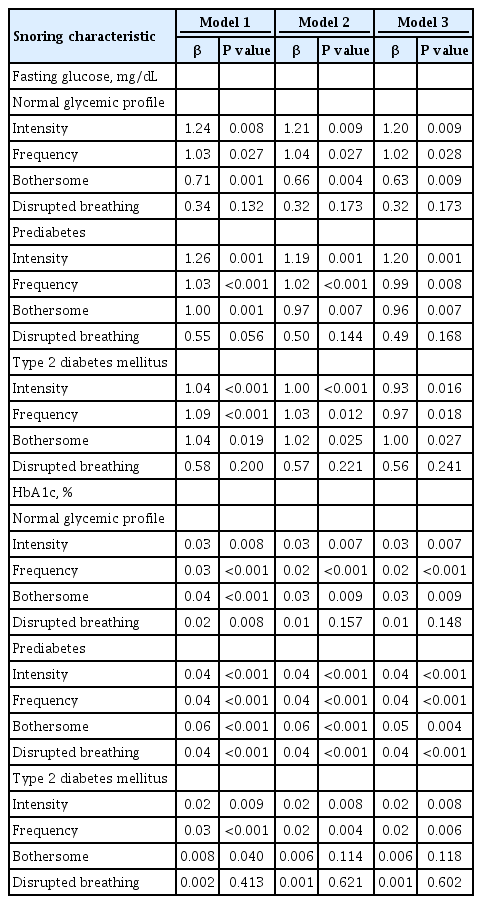
Association of individual characteristics of snoring with fasting glucose and HbA1c (n=3,948)
Table 4 presents results from the multinomial logistic model comparing the risk for prediabetes and type 2 diabetes mellitus across categories of each snoring dimension. All risk levels are in reference to non-snorers with normal glycemic profile. After adjusting for age, sex, and known risk factors of type 2 diabetes mellitus, participants with the most severe snoring were at 1.81 times higher risk (95% CI, 1.07 to 2.33) for prediabetes and 1.84 times higher risk (95% CI, 1.14 to 2.95) for type 2 diabetes mellitus. Such graded association was also noted across more frequent snoring among participants with prediabetes (OR, 1.79; 95% CI, 1.33 to 2.24) and type 2 diabetes mellitus (OR, 2.05; 95% CI, 1.48 to 2.83). Disruptive snoring was associated with 1.59 times higher risk for type 2 diabetes mellitus (95% CI, 1.10 to 2.25) only. Likewise, positively graded association with more frequent disrupted breathing was observed only for type 2 diabetes mellitus; those reporting near-daily disrupted breathing had 2.2 times higher odds for type 2 diabetes mellitus (95% CI, 1.06 to 4.30), compared to those with complacent breathing. As a supplementary analysis, we examined the association of each sleep variable with prediabetes and type 2 diabetes mellitus (Supplementary Table 2). To integrate comprehensive aspects of sleep, we additionally adjusted for these variables when assessing the odds for prediabetes and type 2 diabetes mellitus (Table 4). Additional adjustments did not reverse the direction nor noticeably diminish the strength of association.
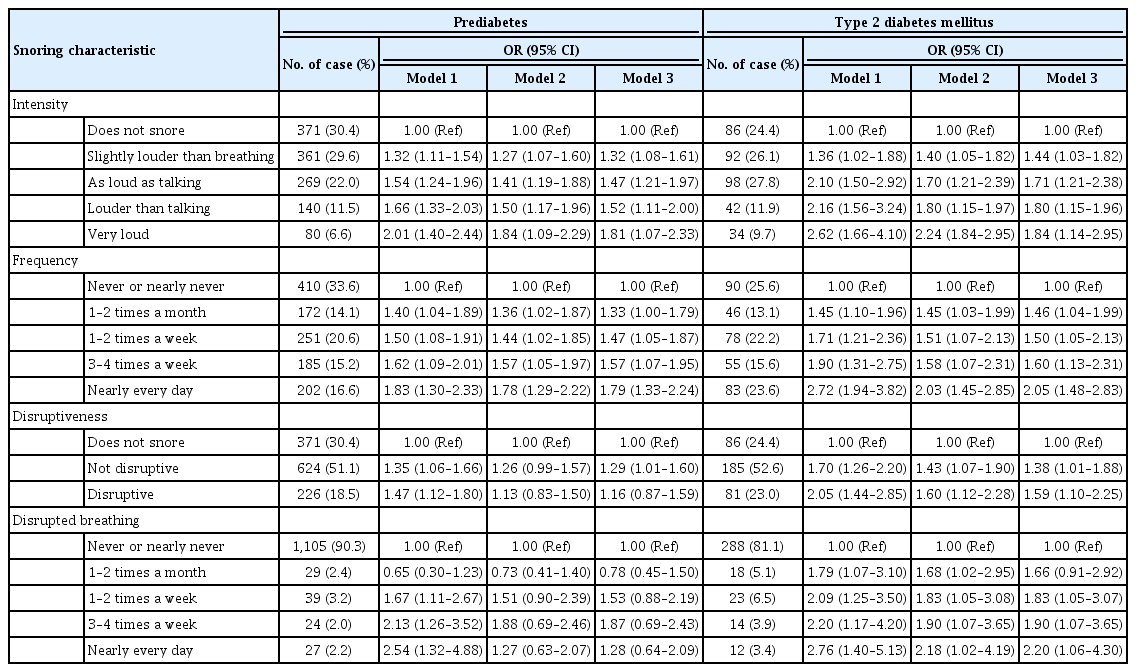
Association of individual characteristics of snoring with prediabetes and type 2 diabetes mellitus (n=3,948)
In the first subgroup analysis stratified by obesity status, the association between snoring intensity and frequency with type 2 diabetes mellitus remained significant in participants with BMI less than 25 kg/m2 (Supplementary Table 3). Non-obese participants reporting the highest intensity snoring had 1.54 times higher odds (95% CI, 0.97 to 2.66) for prediabetes and 1.83 times higher odds (95% CI, 1.24 to 2.43) for type 2 diabetes mellitus, compared to normal weight, non-snorers. Moreover, regardless of obesity status, participants reporting higher frequency snoring were at incrementally higher risk for both prediabetes and type 2 diabetes mellitus. The second subgroup analysis stratified participants by hypertension prevalence (Supplementary Table 4). Similarly, participants without hypertension were at higher risk for prediabetes and type 2 diabetes mellitus across more intense and frequent categories of snoring, but the experience of bothersome snoring nor disrupted breathing did not yield any significant results.
DISCUSSION
In this community-dwelling cohort of middle-aged Korean adults, snoring frequency and intensity were significantly associated with higher odds for both prediabetes and type 2 diabetes mellitus, independent of socioeconomic, behavioral, and other sleep-related factors. Furthermore, snoring also showed continuous association with elevated glycemic biomarkers in among persons with type 2 diabetes mellitus. Therefore, in a primary prevention setting, persons experiencing habitual snoring or OSA may be at high-risk for current or future type 2 diabetes mellitus, and timely screening for diabetes may be advisable in these individuals. Conversely, in patients already with type 2 diabetes mellitus, habitual snorers may be potential targets for lifestyle modifications or more aggressive clinical interventions to improve sleep quality and to optimize glycemic control.
Our findings on the association between snoring and type 2 diabetes mellitus are consistent with previous studies. Among large Chinese community studies, both occasional and habitual snoring were significantly associated 1.4 times higher risk for impaired fasting glucose and 1.1 times higher risk for impaired glucose tolerance, even after adjusting for diabetes- and sleep-related covariates [13]. The Cardiovascular Health Study also demonstrated that diverse symptoms of OSA, including daytime sleepiness and disruptive snoring, were associated with elevated fasting glucose level and lower insulin sensitivity [22]. In the Nurses' Health Study, the multivariable-adjusted hazard ratio of developing type 2 diabetes mellitus was 1.41 (95% CI, 1.22 to 1.63) for self-reported occasional snorers and 2.03 (95% CI, 1.71 to 2.40) for habitual snorers [523]. In a Korean study, compared to non-snorers, habitual snorers showed analogous baseline fasting glucose and insulin levels, but later underwent more drastic increase over 1- and 2-hour oral glucose tolerance test [24]. In another community-dwelling Korean population, the homeostatic model assessment-insulin resistance showed dose-response relationship across higher frequency snoring gradient in female [25].
However, our study extends the previous findings in two important ways. Firstly, it examined multiple characteristics of snoring, rather than simply assessing its absence or presence. Secondly, it examined both stages of diabetes (prediabetes and type 2 diabetes mellitus), simultaneously adjusting for surrogate markers for sleep fragmentation, obstruction, recurrent arousals, etc.
The observed association between snoring and type 2 diabetes mellitus is biologically plausible. Snoring is a form of abnormal breathing during sleep that inhibits good quality sleep via oxygen desaturation and upper airway obstruction [11]. This, resultant intermittent hypoxia leads to insulin resistance and disrupts glucose metabolism via several pathways. First, increased sleep fragmentation and frequent arousals trigger pro-inflammatory cascade by elevating interleukin-6, C-reactive protein, and fibrinogen levels and lowering albumin levels, thereby systematically damaging glucose stability and beta-cell function [26]. Another proposed mechanism is that snoring activates sympathetic nervous system, resulting in catecholamine elevation and hypothalamic-pituitary-adrenal axis activation. This conjointment of elevated cortisol, formation of reactive oxygen species, and increased oxidative stress alter sleep, thereby glucose metabolism [27282930]. Lastly, snoring may be manifestation of behavioral risk factors of type 2 diabetes mellitus, such as lack of physical activity. Physical inactivity is known to reciprocate circulating leptin and ghrelin levels that are responsible for increased appetite, thereby encourage higher caloric intake [31]. Excessive energy consumption coupled with reduced physical activity can disrupt food intake pattern and energy expenditure, accelerating obesity development and glycemic deterioration [31].
Despite numerous proposed mechanisms, other studies have shown divergent findings on the association between snoring and prevalence or manifestation of type 2 diabetes mellitus. Several studies demonstrated that daytime sleepiness [1932] or short sleep duration [3334] was rather associated with altered glucose metabolism, poor glycemic control, and insulin resistance. Perhaps, regardless of sleep phenotype, considering the high prevalence of snoring in the elderly population, OSA symptoms may be benign part of the typical aging process without reflecting a specific glycemic or metabolic pathology. In endocrinological context, sex-specific steroid hormones and dimorphism may support female-specific associations reported in previous research [3536]. Varied data collection tools and variable treatment also contribute to discrepancies in effect size. Foremost, the presence of obesity and hypertension yield synergistic effect on diabetes. The amalgamation of adiposity and sleep breathing disturbances embodies high-risk for type 2 diabetes mellitus and CVD [37]. Therefore, considering the high likelihood that adjustments may still leave residual confounding, we performed subgroup analyses, in which we confirmed that the association persisted even in non-obese and normotensive groups.
Strengths of the present study include meticulous breakdown of snoring and comparison of associations between its individual dimension with prediabetes and type 2 diabetes mellitus risk. Moreover, the infrastructure of this large, general population cohort study adeptly served in ascertaining both the exposure and outcome variables in standardized manners. Finally, the nature of healthy community-based cohort allows to generalize our findings in detecting high-risk group for prediabetes/type 2 diabetes mellitus in ubiquitous clinic settings.
Several limitations merit consideration when interpreting our findings. Due to the cross-sectional study design, we were unable to infer specific directionality of the association between snoring and type 2 diabetes mellitus. Assessment of snoring and other sleep variables might have resulted in non-differential misclassification bias, due to differing recall capability and awareness of own sleep habits by the presence of bed partners. While subjective, use of sleep questionnaires still have fair clinical applicability for its low cost and time efficiency. Moreover, previous studies have reported that self-reported snoring correlates well with objective measures, especially among frequent snorers [38]. Availability of diverse sleep collection methodology warrants further studies, in which self-reported sleep measures be replaced with wearable actigraphy or selectively recruit high-risk individuals to undergo polysomnography to confirm reliability of sleep questionnaires. Furthermore, prior studies have shown that individuals who are unmarried or without bed partners tend to underreport their snoring [39]. Restricting the participants to those with bed partners may increase the accuracy of sleep measurements.
In summary, increasing snoring frequency and intensity were independently associated with risk of both prediabetes and type 2 diabetes mellitus in middle-aged adults. The associations persisted after adjustment for and stratification by obesity, hypertension, and other sleep variables. Snoring may impair glucose metabolism even in otherwise metabolically health adults; in the light of these findings, screening for type 2 diabetes mellitus may be warranted in asymptomatic individuals with habitual snoring. Furthermore, snoring may be a risk factor for poor glycemic control in diabetes, thereby warrants close and periodic surveillance and potential lifestyle and pharmacological interventions.
ACKNOWLEDGMENTS
This work was supported by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health and Welfare, Republic of Korea (grant no. HI13C0715). The authors appreciate all cohort members who participated voluntarily in the study. We are also grateful to members of the research staff for their passion.
We have uploaded data for each survey year to iCReaT, the clinical research information management system of the Korea National Institute of Health. We also keep biospecimens such as serum, plasma, buffy coat, and urine for future use, after obtaining individual consent for the retention period and scope of use. Biospecimens will be deposited at the Korea Biobank, managed by the Korea Centers for Disease Control and Prevention, after completion of the baseline assessment. Although cohort enrollment and baseline assessment are ongoing, this study is open to interested researchers. Researchers interested in collaborative study are invited to contact the CMERC principal investigator, Hyeon Chang Kim, at hckim@yuhs.ac.
Notes
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTIONS
Conception or design: S.M.J.C., J.S.S., H.C.K.
Acquisition, analysis, or interpretation of data: S.M.J.C., H.L., H.C.K.
Drafting the work or revising: S.M.J.C., H.L., H.C.K.
Final approval of the manuscript: S.M.J.C., H.L., J.S.S., H.C.K.
References
SUPPLEMENTARY MATERIALS
Supplementary Table 1
Association of individual characteristics of snoring with fasting glucose and HbA1c by sex (n=3,948)
Supplementary Table 2
Association of sleep variables with prediabetes and type 2 diabetes mellitus among total participants (n=3,948)
Supplementary Table 3
Association of individual characteristics of snoring with prediabetes and type 2 diabetes mellitus by obesity (n=3,948)
Supplementary Table 4
Association of individual characteristics of snoring with prediabetes and type 2 diabetes mellitus by hypertension prevalence (n=3,948)