- Current
- Browse
- Collections
-
For contributors
- For Authors
- Instructions to authors
- Article processing charge
- e-submission
- For Reviewers
- Instructions for reviewers
- How to become a reviewer
- Best reviewers
- For Readers
- Readership
- Subscription
- Permission guidelines
- About
- Editorial policy
Articles
- Page Path
- HOME > Diabetes Metab J > Volume 34(2); 2010 > Article
-
Original ArticleSmall Rice Bowl-Based Meal Plan versus Food Exchange-Based Meal Plan for Weight, Glucose and Lipid Control in Obese Type 2 Diabetic Patients
- Hee-Jung Ahn1, Kyung-Ah Han2, Hwi-Ryun Kwon1, Bo-Kyung Koo3, Hyun-Jin Kim2, Kang-Seo Park2, Kyung-Wan Min3
-
Korean Diabetes Journal 2010;34(2):86-94.
DOI: https://doi.org/10.4093/kdj.2010.34.2.86
Published online: April 30, 2010
- 3,205 Views
- 28 Download
- 10 Crossref
1Diabetes Center, Eulji Hospital, Seoul, Korea.
2Department of Internal Medicine, Eulji University School of Medicine, Daejeon, Korea.
3Department of Internal Medicine, Seoul National University School of Medicine, Seoul, Korea.
- Corresponding author: Kyung-Wan Min. Diabetes Center, Eulji Hospital, 280-1 Hagye 1-dong Nowon-gu, Seoul 139-872, Korea. minyungwa@yahoo.co.kr
- *Hee-Jung Ahn and Kyung-Ah Han jointly contribute to this paper as first authors.
Copyright © 2010 Korean Diabetes Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Background
- The Korean National Health and Nutrition Examination Surveys reported 65% of daily energy intake (EI) as carbohydrate (CHO) in the Korean population and main source of CHO was cooked rice. We used a standardized-small sized rice bowl for diet education and investigated its effectiveness on body weight, glucose and lipid, compared to the conventional food exchange system in type 2 diabetes obese women.
-
Methods
- Type 2 diabetic women with body mass index ≥ 23 kg/m2 were randomly assigned to small rice bowl-based meal plan (BM) and food exchange-based meal plan (ExM) group. Both groups were asked to reduce their EI by 500 kcal/day for 12 weeks. The macronutrient composition was instructed: 55 to 60% of EI as CHO, 15 to 20% as protein, and 20 to 25% as fat. BM group received only a simple instruction for application of the rice bowl. Nutrient intake was estimated with the 3-day dietary records.
-
Results
- Finally, 44 subjects finished the study. The percent reduction of body weight was significant both BM group (-5.1 ± 2.6%) and ExM group (-4.8 ± 2.8%) after 12 weeks (P < 0.001) but there was no difference between the groups. There was no difference in the proportional change of CHO, protein and fat in EI between the groups. Additionally, the change of HbA1c and low density lipoprotein-cholesterol were not significantly different between the two groups.
-
Conclusion
- The BM group was as effective as ExM for body weight and glucose control in type 2 diabetes obese women.
- In obese type2 diabetes, meal education plan is important for reduction of their body weight (BW) [1], but which meal plan is effective in decreasing weight is not well-known. For weight control, low-fat diet has been traditionally recommended [2]. However, Nordmann et al. [3] reported that in meta-analysis low-carbohydrate (CHO) diet declined BW more than low-fat diet in six months and low-CHO diet was helpful in reducing serum triglyceride and in increasing high density lipoprotein cholesterol (HDL-C) but could increase low density lipoprotein cholesterol (LDL-C) level. For these reasons American Diabetes Association (ADA) recommends both of low-fat diet and low-CHO diet as effective meal plans to reduce BW for a short period [4].
- According to Korean Health and Nutrition Examination Survey conducted in 2005, the rates of CHO, protein and fat to total energy intake (EI) of Koreans were 64.5%, 15.6%, and 20.5%, respectively, and National Health and Nutrition Examination Survey (NHANES) performed in the U.S. said that those to EI of Americans were 51.7%, 14.8%, and 32.9%, respectively. Therefore, Koreans were observed to take more CHO and less fat compared to Americans [5,6]. In addition, when the obese group and the normal group were divided by body mass index (BMI) of 25 kg/m2 the obese women had significantly more CHO than those with normal BMI [7]. That was similar with the result of Park et al. [8] saying that obese women with type 2 diabetes took significantly more CHO than others with the disease.
- Food exchange system has been widely used to decrease dietary EI and to control macronutrient composition for weight reduction in obese patients with type 2 diabetes. However, the survey on recognition on food exchange system performed with dietitians in Seoul and Gyeongin area revealed that 39% said that food exchange system was hard to be utilized and 49% did that it was complex and confusing [9]. With this background, simple education methods are needed and in foreign countries a simplified meal education such as "plate method." "Plate method" means that 1/3 to 1/4 of the total dish area is served with protein including meat, fish, egg, and cheese and the other area is done with starch, grain, bread, and vegetables to decline the intake of protein and fat relatively [10,11]. But, studies on simple methods to decrease CHO actively for Koreans with type 2 diabetes taking high-CHO diet with different dietary patterns compared to foreigners, are insufficient.
- Ahn et al. [12,13] reported that among type 2 diabetes patients the size of rice bowl was related with rice intake and obese patients with type 2 diabetes who used smaller rice bowl than what they ordinarily used showed an effective decrease in EI and CHO intake. However, any clinical usefulness of meal plan of supplying a smaller rice bowl than a bowl commonly used has not been reported.
- Therefore, this study investigated clinically the difference in effect on BW, glucose and lipid control between meal plans using food exchange system and reducing rice intake with small rice bowl with obese Koreans with type 2 diabetes.
INTRODUCTION
- Subjects
- This study recruited women with type 2 diabetes visiting Diabetes Center of Eulji Hospital as outpatients from June 2008 to November 2008, hearing the purpose and the methods of this study and agreeing with them. The data of totally 44 patients followed up for all of 12-week study period were finally analyzed. Type 2 diabetes was diagnosed by following diagnosis criteria invented by ADA in 1997. The subjects of this study were 20 to 70 years old when they participated in this study and their BMI and glycosylated hemoglobin (HbA1c) were 23 kg/m2 or higher and 6.5 to 10%, respectively. They had taken orally a hypoglycemic agent of over 1,000 mg metformin for at least 12 weeks without insulin therapy before the beginning of this study. The patients taking insulin or thiazolidinedion, drinking one or more cups of alcohol every day, having any special dietary habit (e.g., vegetarian), not being able to take exercise and having gestational diabetes, malignant tumor, cardiovascular disease or diabetic nephrosis, taking drugs to reduce BW within the last three months, not being followed up and refusing the participation in this study were excluded. After four-week differentiation, they continued to take 1,000 mg metformin or sulfonylurea for 12 weeks and maintained their blood pressure agents or anti-lipid agents during the study period. This clinical study was approved by Institutional Review Board of Eulji Hospital (Approval no.: EMCIRB 08-28).
- Methods
- After the subjects enrolled, they were divided into small rice bowl-based meal plan (BM) group and food exchange-based meal plan (ExM) group, with the random number table.
- To examine dietary EI and nutrient intake, both of the two groups were asked to write three-day diet record sheet (two days for weekdays and a day for weekend) every two weeks. Ordinary total energy expenditure and physical activity for activities were monitored at each visit by using a multi-record accelerometer (Lifecorder®; Suzuken Co., Nagoya, Japan) for all day except sleeping time.
- The subjects were educated on the diet record method simply before writing the record sheet actually and they were asked to write amounts and kinds of all foods taken for a meal, nutrition supplementary foods and snacks for a day on the dietary record sheet by themselves. To increase accuracy of the record, a registered dietitian (RD) reviewed contents of the sheets by using real-sized food models, measuring cups, measuring spoons and the book called "data on eye measurement of foods" (The Korean Dietetic Association, 1999) when the sheets were returned. The data from the sheet were analyzed with CAN-Pro (Computer-Aided Nutritional Analysis Program, version 2.0; Korean Nutrition Society, Seoul, Korea) and were converted into nutrient intake.
- The subjects maintained ordinary food intake and exercise before 4 weeks from the beginning of this study and both of the two groups reduced their food intake by 500 kcal/day from their ordinary intake with a goal of decreasing BW by 0.45 kg per week during the study period. The proportions of CHO, protein and fat to the total EI were recommended to be 55 to 60%, 15 to 20%, and 20 to 25%, respectively [14].
- The subjects of the BM group were supplied with 200 cc rice bowls containing around 200 kcal rice and diet leaflet corresponding to described energy and were educated on tips for putting rice into the bowl and taking side dishes, within 10 minutes by person to person. They were asked to use the bowl for every meal and CHO sources such as bread, rice cake, potato, sweet potato, and jeon were limited through the leaflet. Noodle could substitute for rice but any specific amount for that was not suggested. Fruit intake was shown as the amount per day through the leaflet. For fish, meat and vegetables, the subjects were educated with pictures of diet fitting each food exchange unit and were asked to practice it but that was not emphasized intensively at each visit. The pictures of diet of fish, meat and vegetables were included in the leaflet by focusing on foods frequently found in the preliminary survey.
- For the ExM group, food exchange system (Korean Diabetes Association [KDA], the Korean Nutrition Society, The Korean Dietetic Association, 1995) for meal plan and the data of food exchange stickers (KDA) were utilized. The subjects of the group were educated about grouping of foods into list and serving size and rice was asked to be measured according to the serving size with a scale. Cereals, fish & meat, milk and fruit were recommended to be taken by following serving size proportional to each EI and nutrient composition. The subjects were educated about food exchange system for around 40 minutes and were asked to participate in buffet education for diabetes patients (practice using food exchange system) one time.
- Compliance of EI of the two groups was calculated as a percent by comparing their actual intake with the targeted intake (reduction of 500 kcal/day from the ordinary level).
- As exercise, walking, which had been conducted before the education, was maintained to be 4 to 6 levels (3.6 to 5.2 MET) with a multi-record accelerometer (Lifecorder®) for 30 to 60 minutes per day, five or more times per week for 12 weeks.
- Height, BW, and waist circumference were measured at the beginning of this study and at each visit made every two weeks. Height and BW were gauged in thin clothes by taking off outer clothes and BMI was calculated by dividing the BW (kg) with the square of the height (m2). The narrowest line between the lower rib and iliac crest was measured as waist circumference with a tapeline when a subject breathed out easily, and blood pressure was gauged in a sitting posture with a hemomanometer (Yamasu Co., Saitama, Japan) after resting for 10 minutes.
- Biochemical tests were performed for the both of the two groups at the beginning of the study and in 12 weeks. For blood test, venous blood was collected after over 10-hour fasting and was centrifuged at 3,000 rpm for 15 minutes to isolate serum. The serum was stored at -70℃ in a refrigerator and was used for analysis. Fasting blood glucose and HbA1c were measured with glucose oxidase method and HPLC utilizing cation exchange resin, respectively. Cholesterol, triglyceride, HDL-C, and LDL-C were examined with kits using enzymatic response and an automatic chemistry analyzer (Hitachi 7170; Hitachi, Tokyo, Japan).
- The lengths of abdominal subcutaneous and visceral fat were measured with 3.5 MHz probe of high-resolution B-mode scanner (HDI 5000; ATL-Phillips, Bothell, WA, USA) at the point separating by 1 cm above the bellybutton at the end of expiration when a subject lied down. The lengths of abdominal subcutaneous and visceral fat were determined with the length from the skin surface to the upper side of abdominal muscle and with the length from the inner side of abdominal muscle to the anterior wall of the aorta at the same point, respectively.
- To evaluate compliance of use of bowl or scale, all subjects of the two group were asked to write whether they used the bowl or the scale for each meal and the record sheets were returned at each visit made every two weeks. Compliance of use was calculated as a percent of frequency of using the bowl or the scale out of the total meals every two weeks and the average of compliance was done every two weeks to assess the compliance.
- Compliance of use of bowl (%) = Frequency of using bowl / Number of total meals × 100
- Compliance of use of scale (%) = Frequency of using scale / Number of total meals × 100
- Data analysis and statistical analysis
- For data analysis, means and standard deviation were calculated with SPSS statistics program version 15.0 (SPSS Inc., Chicago, IL, USA). Paired sample t test, independent sample t test and crosstabs analysis were used for comparison of physical characteristics, results of biochemical tests and averages of nutrient intake before and after the education, for comparison between the two groups and for categorical variables, respectively. Correlation among intake of CHO, protein and fat was examined with Pearson's correlation coefficient. A P value of less than 0.05 was considered to be statistically significant.
METHODS
Dietary EI and total energy expenditure
Diet and exercise education
Physical measurement and biochemical tests
Abdominal ultrasound
Compliance of use of bowl and scale
- General characteristics of subjects
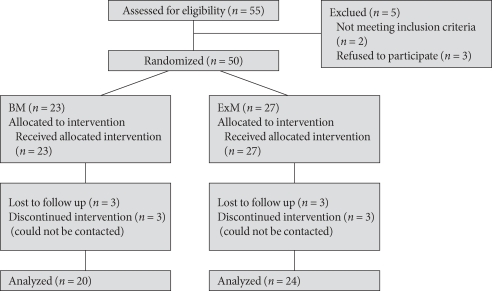
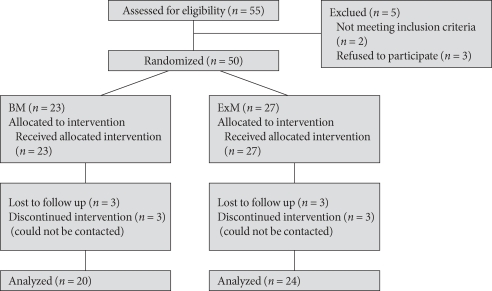
- Out of 55 subjects registered in this study, fifty subjects except those not meeting registration criteria (n = 2) and those refusing the participation (n = 3) were divided into the BM and the ExM groups. As three in each group dropped out of this study (move or not contacted), finally 44 subjects participated in this study. The drop-out rates of the two groups were not different (Fig. 1). Age, prevalence period, BMI, fasting blood glucose level and HbA1c of the totally 44 subjects were 55.2 ± 7.6 years, 6.6 ± 4.6 years, 28.0 ± 3.6 kg/m2, 142 ± 35 mg/dL, and 7.9 ± 0.8%, respectively. As therapy for diabetes only metformin and combination of metformin and sulfonylurea were used for 40.9% and 59.1% of the patients, respectively. In two weeks after the beginning of this study, 46.2% of the subjects treated with combination of metformin and sulfonylurea reduced the dose of sulfonylurea to prevent hypoglycemia, and it was decreased to 50% of its initial level when this study was ended. There was no difference in the reduced amount of the dose between the two groups. The two groups also did not show any significant difference in age, prevalence period of diabetes, BMI, fasting blood glucose, dietary energy intake, total energy expenditure and treatment methods. As the average dietary energy intake was 1,931 ± 227 kcal/day and total energy expenditure and physical activities recorded 1,928 ± 165 kcal/day, respectively, any significant difference between the two groups was not found (Table 1). The proportions of CHO, protein and fat to the total EI were 63.1 ± 7.8%, 16.0 ± 2.4% and 21.1 ± 5.4%, respectively. The rate of CHO was higher than the rate recommended by KDA or 55 to 60% and it was not different between the two groups [14] (Table 2). The frequencies of using the bowl or the scale for 12 weeks were 70 ± 28%, 47 ± 24%, and 59 ± 24% for breakfast, lunch and dinner, respectively and there was no significant difference between the two groups.
- Changes of BW and abdominal visceral fat
- Both of the BM and the ExM groups showed significantly reduced BW by 3.7 ± 2.3 kg (5.1 ± 2.6%) and 3.3 ± 2.0 kg (4.8 ± 2.8%) in 12 weeks (P < 0.001) but their reduced BW between the group was not significantly different. Waist circumference also decreased significantly by -4.9 ± 3.7 cm (-5.1 ± 3.8%) and -4.5 ± 3.1 cm (-4.8 ± 3.3%) in the BM and the ExM groups, respectively (P < 0.001) but there was no significant difference in the reduced waist circumference of the two groups.
- Abdominal visceral fat measured with ultrasound was declined significantly by -1.1 ± 0.7 cm (-1.7 ± 1.1%) only in the BM group (P < 0.01) but the reduced amount of the two groups were not significantly different. Abdominal subcutaneous fat of both of the two groups were significantly reduced (P < 0.01) and the difference in the reduced fat between the two groups was not significant (Table 3).
- Changes of blood glucose and lipids
- HbA1c was decreased significantly by -0.5 ± 0.9 and -0.9 ± 0.7% in the BM and the ExM groups, respectively (P < 0.05) and their difference in the reduced HbA1c was not significant. Although in 12 weeks the BM group recorded significantly higher HDL-C (P < 0.05) and the ExM group did significantly lower LDL-C (P < 0.05) compared to their initial levels the changes of total cholesterol, triglyceride, HDL-C and LDL-C were not significant different between the two groups. Systolic blood pressure was declined significantly in both of the two groups (P < 0.05) but there was no significant difference in the reduced level between the two groups (Table 3).
- Changes of dietary energy intake and CHO intake
- As changes of dietary energy intake and total energy expenditure during 12 weeks were not consistent, their averages for the 12 weeks were used. Dietary energy intake and nutrient intake were assessed with 3-day dietary record. Dietary energy intake was significantly reduced by -439 ± 202 kcal/day and -369 ± 164 kcal/day in the BM and the ExM groups, respectively in 12 weeks (P < 0.05) and the difference between the two groups was not significant. Compliance of EI was decreased from 136 ± 5% to 107 ± 13% in the 12 weeks and the level was similar with the described energy level in both of the two groups (P < 0.001). There was no significant difference in the average of total energy expenditure for 12 weeks before and after the education and any difference in the increased amount between the two groups were also not observed.
- In 12 weeks both of the two groups showed significantly less CHO, protein and fat intake (P < 0.05) and the reduced amount of CHO, protein and fat was not significantly different between the two groups. Although the proportions of CHO, protein and fat to total EI initially recorded 63.1:16.0:21.1%, they changed into 60.8:17.1:22.4% in 12 weeks which were more similar with the proportions recommended by KDA. There was no significant difference between the two groups. Fiber, cholesterol and sodium intake were also not different in 12 weeks compared to their initial levels and the changes of the two groups were also not significantly different (Table 2).
- In the BM group the CHO intake for 12 weeks was correlated with the protein intake (r = 0.582, P = 0.006) and the fat intake (r = 0.581, P = 0.007) for the same period.
RESULTS
- Although small rice bowl-based meal plan did not provide sufficient information on tips to choose various foods and portion size of foods, the reduced CHO intake by using the small rice bowl led to no significant difference in the proportions of CHO, protein and fat to total EI compared with the ExM group. In addition, the cholesterol and the sodium intake were not different before and after the 12-week education and according to education methods. This result was considered to be because the subjects in the two groups chose similar foods so that they did not show difference in intake of each nutrient.
- In particular, the CHO intake of the BM group for 12 weeks showed correlation with its protein intake (r = 0.582, P = 0.006) and its fat intake (r = 0.581, P = 0.007). It suggested that for Koreans having meals mainly with rice when snack with CHO sources were limited and the amount of rice for a meal was changed with a rice bowl the EI of the provided rice could affect the EI of side dishes because they took meals with a standard of the amount of rice [15]. For this reason, Koreans with type 2 diabetes could reduce their nutrient intake only with small rice bowls as much as food exchange-based meal plan.
- The obese patients with type 2 diabetes decreased dietary energy intake by 439 ± 202 kcal/day and finally reduced their BW by -3.7 ± 2.3 kg (-5.1 ± 2.6%) through small rice bowl-based meal plan in 12 weeks and the reduced amounts were not different from those of the ExM group. The reduced levels of both of the two groups were found to be higher than the level or 1.4 kg (2.0%) in a study of Woo et al. [16] performed with type 2 diabetes patients who had meals following diet guidelines recommended by KDA by using food exchange system for 12 weeks. Abdominal visceral and subcutaneous fat were measured with ultrasound showing a correlation with computed tomography, and the reduced amounts of the abdominal visceral and subcutaneous fat were also not significantly different between the two groups [17]. This finding that the decreased amounts of BW and abdominal fat were similar despite different education methods between the two groups seemed to be caused by no difference in reduction of dietary energy intake and of macronutrient composition.
- According to a previous clinical research on medical nutrition therapy for diabetes conducted with type 2 diabetes patients, HbA1c was reduced by 0.25 to 2.9% for 3 to 6 months [4]. Wilson et al. [18] revealed that among diabetes patients with 8% of an average HbA1c the education on diet performed by a RD decreased the level by 0.26 to 0.32% and a study of UK Prospective Diabetes Study (UKPDS) [19] found that among newly diagnosed type 2 diabetes patients the education on BW reduction and low-fat diet reduced the HbA1c level by 1.9% (from 8.9% to 7%). A study of Kim et al. [20] conducted with Koreans with diabetes reported that combination of meals following guidelines recommended by KDA and using food exchange system and exercise for 12 weeks decreased HbA1c by 0.7% (from 8.9% to 8.2%) and a research of Woo et al. [16] found that meals following guidelines recommended by KDA and using food exchange system for 20 weeks reduced HbA1c by 0.1%. Because the decrease of HbA1c is influenced by types of diabetes, prevalence period, initial HbA1c level and education methods, their decreased levels are hard to be compared directly [21]. However, the decreased amount of HbA1c observed in this study was similar with that of a study of Wilson et al. [18] performed with diabetes patients with similar initial levels compared to those of the subjects of this study. Moreover, the two groups of this study educated with different methods also did not show any significant difference in the decreased amount. The HbA1c was declined to 7% or a level recommended by KDA in both of them. Considering that sulfonylurea was reduced by 50% to prevent hypoglycemia in the combination group of metformin and sulfonylurea, both of the two groups were found to be effective in controlling blood glucose. The reason why the decrease amount of HbA1c was not different between the two group was considered to be no difference in drug therapy, the decreased amount of dietary energy and macronutrient composition.
- Improvement of dyslipidemia of type 2 diabetes patients can decrease the risk of cardiovascular diseases, and ADA's first goal for management of dyslipidemia was to reduce LDL-C [4]. Yu-Poth et al. [22] reported that in meta-analysis meals following The National Cholesterol Education Program (NCEP) step I and step II declined LDL-C by 15 to 25 mg/dL in patients without diabetes and Barnard et al. [23] revealed that meals following recommendations of ADA decreased LDL-C by 3.4 mg/dL in type 2 diabetes patients. Although LDL-C of only the ExM groups was reduced by 10.6 mg/dL, the difference between the two groups was not significant. When Koreans with type 2 diabetes patients had meals following guidelines recommended by KDA, the decreased amount of LDL-C was found to be similar with that shown in a study of Barnad et al. and both of the two groups recorded less than 100 mg/dL or a level recommended by ADA [4,23]. The reason why the level was not significantly decreased in 12 weeks was thought to be because initial LDL-C was not high enough to produce additional decrease, and the reason why the levels of the two groups were not different was considered to be because the rates of patients taking lipid-lowering agent were not different between the two groups and their fat intake and total cholesterol intake were not largely different between them using different education methods.
- This study was a random designation study comparing effects of small rice ball-based rice intake control on BW, blood glucose and lipid with those of traditional ExM with obese Koreans with type 2 diabetes taking high-CHO diet, and it was meaningful to investigate self-management meal plan which could replace food exchange based meal plan. Nevertheless, future studies are needed to compare effects of education with obese patients with different knowledge levels, gender and age and using different therapies. In particular, this study had limitations that it examined only women who took relatively more CHO and followed further management relatively well, that many of the subjects took metformin because they were limited to be obese patients and that it did not show clinical outcomes of various groups by limiting to a group using only metformin and a group using combination of metformin and sulfonylurea to evaluate the effect on BW and blood glucose.
- Moreover, a low frequency of using the bowl recording 57.4 ± 21.7% was another limitation of this study. However, according to a study of Ahn et al. [24] analyzing compliance of use of a bowl and factors hindering it, 11.1% of the subjects said that they did not use it because they learned the concept of the amount of foods fully through their experience of using it. Although this study did not examine specific reasons of the low frequency, the same reason was said. In addition, the study period of this study included summer vacation period when persons ate out usually so that the frequency could be observed to be low. The finding of this study that the effects of small rice bowl-based meal plan showed similar effects on EI, nutrient intake, BW, blood glucose and lipid control compared to those of food exchange-based meal plan despite the low frequency, suggested its possibility as one of clinically useful meal plans.
DISCUSSION
- 1. Ziemer DC, Berkowitz KJ, Panayioto RM, El-Kebbi IM, Musey VC, Anderson LA, Wanko NS, Fowke ML, Brazier CW, Dunbar VG, Slocum W, Bacha GM, Gallina DL, Cook CB, Phillips LS. A simple meal plan emphasizing healthy food choices is as effective as an exchange-based meal plan for urban African Americans with type 2 diabetes. Diabetes Care 2003;26:1719-1724. ArticlePubMedPDF
- 2. Bantle JP, Wylie-Rosett J, Albright AL, Apovian CM, Clark NG, Franz MJ, Hoogwerf BJ, Lichtenstein AH, Mayer-Davis E, Mooradian AD, Wheeler ML. Nutrition recommendations and interventions for diabetes: a position statement of the American Diabetes Association. Diabetes Care 2008;31(Suppl 1):S61-S78. PubMed
- 3. Nordmann AJ, Nordmann A, Briel M, Keller U, Yancy WS Jr, Brehm BJ, Bucher HC. Effects of low-carbohydrate vs low-fat diets on weight loss and cardiovascular risk factors: a meta-analysis of randomized controlled trials. Arch Intern Med 2006;166:285-293. ArticlePubMed
- 4. American Diabetes Association. Standards of medical care in diabetes: 2009. Diabetes Care 2009;32(Suppl 1):S13-S61. ArticlePubMedPMCPDF
- 5. Yang EJ, Kerver JM, Park YK, Kayitsinga J, Allison DB, Song WO. Carbohydrate intake and biomarkers of glycemic control among US adults: the third National Health and Nutrition Examination Survey (NHANES III). Am J Clin Nutr 2003;77:1426-1433. ArticlePubMed
- 6. Korea Centers for Disease Control and Prevention. The Third National Nutrition Examination Survey (KNHANES III), 2005. 2007. Seoul: Korea Centers for Disease Control and Prevention.
- 7. Korea Centers for Disease Control and Prevention. The Fourth National Nutrition Examination Survey (KNHANES IV-1), 2007. 2008. Seoul: Korea Centers for Disease Control and Prevention.
- 8. Park YM, Sohn CM, Jang HC. Correlation of carbohydrate intake with obesity in type 2 diabetes mellitus patients. J Korean Diet Assoc 2006;12:254-263.
- 9. Lee YN, Roh SY. The study of awareness and practice of Korean dietitians in food exchange lists, serving size and dietary guidelines. J Korean Diet Assoc 2001;7:9-18.
- 10. Pedersen SD, Kang J, Kline GA. Portion control plate for weight loss in obese patients with type 2 diabetes mellitus: a controlled clinical trial. Arch Intern Med 2007;167:1277-1283. ArticlePubMed
- 11. Raidl M, Spain K, Lanting R, Lockard M, Johnson S, Spencer M, Sant L, Welch J, Liddil A, Hartman-Cunningham M. The healthy diabetes plate. Prev Chronic Dis 2007;4:A12PubMed
- 12. Ahn HJ, Koo BK, Jung JY, Kwon HR, Chung MY, Ku YH, Kim JT, Han KA, Min KW. Association between volume of bowls and the dietary intakes in subjects with type 2 diabetes. Korean Diabetes J 2009;33:335-343.Article
- 13. Ahn HJ, Ku YH, Eon YK, Seok HG, Kwon HR, Kim JT, Kim HJ, Park KS, Han KW, Min KW. Reduced rice bowl-based meal plan for carbohydrate intake and dietary pattern in type 2 diabetic patients. Korean Diabetes J 2009;33(suppl 8):206.
- 14. Korean Diabetes Association. A guideline for diabetes education. 2006. 2nd ed. Seoul: Gold Agency; p. 167.
- 15. Son SM. Rice based meal for prevention of obesity and chronic disease. Korean J Community Nutrition 2001;6:862-867.
- 16. Woo YJ, Lee HS, Kim WY. Individual diabetes nutrition education can help management for type II diabetes. Korean J Nutr 2006;39:641-648.
- 17. Jung ED, Chung DS, Lee JY. The correlation between visceral ount by computed tomography in type 2 diabetes. Korean Diabetes J 2008;32:418-427.Article
- 18. Wilson C, Brown T, Acton K, Gilliland S. Effects of clinical nutrition education and educator discipline on glycemic control outcomes in the Indian health service. Diabetes Care 2003;26:2500-2504. ArticlePubMedPDF
- 19. UKPDS Group. UK Prospective Diabetes Study 7: response of fasting plasma glucose to diet therapy in newly presenting type II diabetic patients, UKPDS Group. Metabolism 1990;39:905-912. ArticlePubMed
- 20. Kim SH, Kang ES, Park SY, Lee SJ, Kim MJ, Yoo JS, Ahn CW, Cha BS, Lim SK, Lee HC. The effects of lifestyle modification on the metabolic parameters of type 2 diabetes. J Korean Diabetes Assoc 2004;28:441-451.
- 21. Khan MA, St Peter JV, Breen GA, Hartley GG, Vessey JT. Diabetes disease stage predicts weight loss outcomes with long-term appetite suppressants. Obes Res 2000;8:43-48. ArticlePubMed
- 22. Yu-Poth S, Zhao G, Etherton T, Naglak M, Jonnalagadda S, Kris-Etherton PM. Effects of the National Cholesterol Education Program's Step I and Step II dietary intervention programs on cardiovascular disease risk factors: a meta-analysis. Am J Clin Nutr 1999;69:632-646. ArticlePubMed
- 23. Barnard ND, Cohen J, Jenkins DJ, Turner-McGrievy G, Gloede L, Green A, Ferdowsian H. A low-fat vegan diet and a conventional diabetes diet in the treatment of type 2 diabetes: a randomized, controlled, 74-wk clinical trial. Am J Clin Nutr 2009;89:1588S-1596S. ArticlePubMedPMC
- 24. Ahn HJ, Koo BK, Jung JY, Kwon HR, Kim HJ, Park KS, Han KA, Min KW. Bowl-based meal plan versus food exchange-based meal plan for dietary intake control in Korean type 2 diabetic patients. Korean Diabetes J 2009;33:155-163.Article
REFERENCES
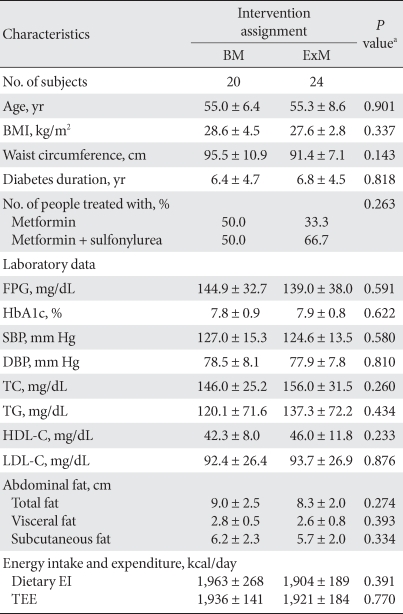
The values were presented as mean ± standard deviation.
BM, small rice bowl-based meal plan; ExM, food exchange-based meal plan; BMI, body mass index; FPG, fasting plasma glucose; HbA1c, glycosylated hemoglobin; SBP, systolic blood pressure; DBP, diastolic blood pressure; TC, total cholesterol; TG, triglycerides; HDL-C, high density lipoprotein cholesterol; LDL-C, low density lipoprotein cholesterol; EI, energy intake; TEE, total energy expenditure.
aThe P values are for comparison between BM and ExM by independent t-test.
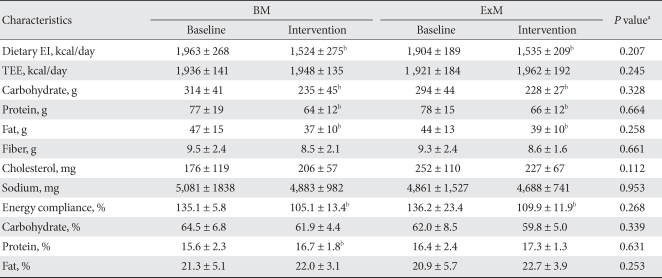
The values were presented as mean ± standard deviation.
BM, small rice bowl-based meal plan; ExM, food exchange-based meal plan; EI, energy intake; TEE, total energy expenditure.
aThe P values are for comparison for the change from baseline to intervention between BM and ExM by independent t-test, bThe P values < 0.05 are for comparison between baseline and intervention by paired t-test.

The values were presented as mean ± standard deviation.
BM, small rice bowl-based meal plan; ExM, food exchange-based meal plan; BW, body weight; BMI, body mass index, SBP, systolic blood pressure; DBP, diastolic blood pressure; FPG, fasting plasma glucose; HbA1c, glycosylated hemoglobin; TC, total cholesterol; TG, triglycerides; HDL-C, high density lipoprotein cholesterol; LDL-C, low density lipoprotein cholesterol.
aThe P-values are for comparison for the change from baseline to intervention between BM and ExM by independent t-test, bThe P values < 0.05 are for comparison between baseline and intervention by paired t-test.
Figure & Data
References
Citations
- Development of a Sport Food Exchange List for Dietetic Practice in Sport Nutrition
José Miguel Martínez-Sanz, Susana Menal-Puey, Isabel Sospedra, Giuseppe Russolillo, Aurora Norte, Iva Marques-Lopes
Nutrients.2020; 12(8): 2403. CrossRef - The Effect of Combined Therapy with Fenugreek and Nutrition Training Based on Iranian Traditional Medicine on FBS, HgA1c, BMI, and Waist Circumference in Type 2 Diabetic Patients: a Randomized Double Blinded Clinical Trial
Seyyedeh Seddigheh Hassani, Arezodar Fallahi, Seyyed Saeid Esmaeili, Mohammad Gholami Fesharaki
Journal of Advances in Medical and Biomedical Research.2019; 27(120): 37. CrossRef - Development of a Spanish Food Exchange List: Application of Statistical Criteria to a Rationale Procedure
Iva Marques-Lopes, Susana Menal-Puey, J. Alfredo Martínez, Giuseppe Russolillo
Journal of the Academy of Nutrition and Dietetics.2018; 118(7): 1161. CrossRef - A Practical Approach to the Management of Micronutrients and Other Nutrients of Concern in Food Exchange Lists for Meal Planning
Giuseppe Russolillo-Femenías, Susana Menal-Puey, J. Alfredo Martínez, Iva Marques-Lopes
Journal of the Academy of Nutrition and Dietetics.2018; 118(11): 2029. CrossRef - Anemia is inversely associated with serum C-peptide concentrations in individuals with type 2 diabetes
Jin Ook Chung, Seon-Young Park, Dong Hyeok Cho, Dong Jin Chung, Min Young Chung
Medicine.2018; 97(32): e11783. CrossRef - Relationship between serum C-peptide level and diabetic retinopathy according to estimated glomerular filtration rate in patients with type 2 diabetes
Jin Ook Chung, Dong Hyeok Cho, Dong Jin Chung, Min Young Chung
Journal of Diabetes and its Complications.2015; 29(3): 350. CrossRef - Serum bilirubin concentrations are positively associated with serum C‐peptide levels in patients with Type 2 diabetes
J. O. Chung, D. H. Cho, D. J. Chung, M. Y. Chung
Diabetic Medicine.2014; 31(11): 1316. CrossRef - Association between serum C-peptide levels and chronic microvascular complications in Korean type 2 diabetic patients
Bo-Yeon Kim, Chan-Hee Jung, Ji-Oh Mok, Sung-Koo Kang, Chul-Hee Kim
Acta Diabetologica.2012; 49(1): 9. CrossRef - Small Rice Bowl-Based Meal Plan for Energy and Marcronutrient Intake in Korean Men with Type 2 Diabetes: A Pilot Study
Hee Jung Ahn, Kyung Ah Han, Jin Young Jang, Jae Hyuk Lee, Kang Seo Park, Kyung Wan Min
Diabetes & Metabolism Journal.2011; 35(3): 273. CrossRef - The Small Rice Bowl-Based Meal Plan was Effective at Reducing Dietary Energy Intake, Body Weight, and Blood Glucose Levels in Korean Women with Type 2 Diabetes Mellitus
Hee Jung Ahn, Kyung Ah Han, Hwi Ryun Kwon, Kyung Wan Min
Korean Diabetes Journal.2010; 34(6): 340. CrossRef
 PubReader
PubReader Cite
Cite