
- Current
- Browse
- Collections
-
For contributors
- For Authors
- Instructions to authors
- Article processing charge
- e-submission
- For Reviewers
- Instructions for reviewers
- How to become a reviewer
- Best reviewers
- For Readers
- Readership
- Subscription
- Permission guidelines
- About
- Editorial policy
Articles
- Page Path
- HOME > Diabetes Metab J > Volume 34(5); 2010 > Article
-
Original ArticleENPP1 K121Q Genotype Not Associated with Coronary Artery Calcification in Korean Patients with Type 2 Diabetes Mellitus
- Dae Joon Jeong, Dong Gyu Lee, Hee-Jung Kim, Eun Hee Cho, Sang-Wook Kim
-
Korean Diabetes Journal 2010;34(5):320-326.
DOI: https://doi.org/10.4093/kdj.2010.34.5.320
Published online: October 31, 2010
- 3,527 Views
- 33 Download
- 4 Crossref
Department of Internal Medicine, Kangwon National University Hospital, Kangwon National University School of Medicine, Chuncheon, Korea.
- Corresponding author: Sang-Wook Kim. Department of Internal Medicine, Kangwon National University Hospital, Kangwon National University School of Medicine, 17-1 Hyoja 3-dong, Chuncheon 200-947, Korea. exoplanet@kangwon.ac.kr
Copyright © 2010 Korean Diabetes Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Background
- Ectonucleotide pyrophosphatase/phosphodiesterase-1 (ENPP1) generates inorganic pyrophosphate, a solute that serves as an essential physiological inhibitor of calcification. Inactivating mutations of ENPP1 are associated with generalized calcification in infancy and an increased risk of developing type 2 diabetes mellitus (T2DM). We hypothesized that the ENPP1 K121Q variant may be associated with increased coronary artery calcification in T2DM patients.
-
Methods
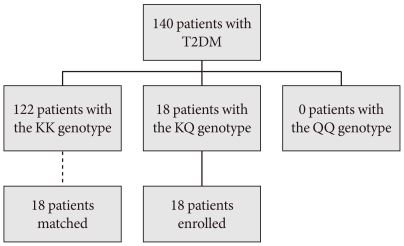
- The study subjects were aged 34 to 85 years and showed no evidence of clinical cardiovascular disease prior to recruitment. A total of 140 patients with T2DM were assessed for their coronary artery calcium (CAC) scores and ENPP1 K121Q polymorphisms were identified.
-
Results
- The prevalence of subjects carrying the KQ genotype was 12.9% (n = 18). There were no 121QQ homozygotes. Patients with the KQ genotype did not show a significantly higher CAC score (122 vs. 18; P = 0.858). We matched each patient with the KQ genotype to a respective control with the KK genotype by gender, age, and duration of diabetes. When compared to matched controls, we observed no significant difference in CAC score (P = 0.959).
-
Conclusions
- The ENPP1 K121Q polymorphism does not appear to be associated with coronary artery calcification in patients with T2DM.
- As in bone remodeling, vascular calcification is regulated by several physiological inhibitors, such as osteopontin, fetuin-A, and ectonucleotide pyrophosphatase/phosphodiesterase-1 (ENPP1) [1,2]. ENPP1 generates inorganic pyrophosphate (PPi), a solute that serves as an essential physiological inhibitor of calcification. Pyrophosphate levels, which are maintained by the activity of ENPP1, can be metabolized by alkaline phosphatase (ALP) into phosphate, a promoter of calcification. A balance between ectonucleotidase and ALP might be crucial in controlling the calcification process.
- Vascular calcification frequently develops in patients with diabetes mellitus resulting in an increased risk of cardiovascular events. The coronary artery calcium (CAC) scores measured by computed tomography is an excellent marker for the overall coronary atherosclerotic burden [3], and is an independent predictor even in asymptomatic diabetic patients [4]. Inactivating mutations of ENPP1 are associated with generalized calcification in infancy [5] and, interestingly, risk of developing type 2 diabetes mellitus (T2DM) [6-8]. These associations have been attributed to the direct interaction of ENPP1 with the α-subunit of insulin receptors [7]. A functional missense DNA polymorphism in exon 4 that causes an amino acid change from lysine to glutamine at codon 121 (K121Q) has been associated with insulin resistance in several populations [6,9-11]. Furthermore, Q variant carriers are associated with an early onset of coronary artery disease in Caucasians [7,12].
- Eller et al. [13] reported that patients who are heterozygous for the ENPP1 K121Q polymorphism have higher coronary calcification scores and increased aortic stiffness in patients with end-stage renal failure. However, patients with chronic renal disease have an abnormal calcium phosphate homeostasis, and the CAC results might be confounded by deranged mineral metabolism. To our knowledge, no data are available on the association between ENPP1 K121Q polymorphism and severity of coronary artery calcifications in T2DM patients or even in healthy subjects. Recently, Lee et al. [14] reported that aortic arch calcification, which was measured qualitatively (all or none) using a plain chest radiograph, is associated with the Q allele in healthy Korean subjects. However, the limited resolution of plain X-rays may render an inconsistent and relatively low sensitivity detection for aortic calcification [15], not to mention that this feature is an indirect marker of coronary atherosclerosis, in contrast with direct quantification of CAC.
- We evaluated whether or not the ENPP1 K121Q polymorphism is associated with increased coronary artery calcification in patients with T2DM who showed no evidence of clinical cardiovascular disease. Confirmation of this association would suggest that genotyping of the ENPP1 gene could be useful in risk stratification for cardiovascular events in patients with T2DM.
INTRODUCTION
- Study subjects
- This study was carried out on 150 patients with T2DM who visited the diabetes clinic at Kangwon National University Hospital between March and June 2007, and who agreed to participate upon our explanation of the purpose and procedures of the study. Diagnosis of T2DM was done in accordance with the diagnostic criteria established by the American Diabetes Association in 1997. Patients who showed typical symptoms of ischemic heart disease or who had previously received coronary angiography or cardiovascular intervention were excluded. We also excluded patients with an accompanying chronic disease such as chronic liver disease, chronic kidney disease where serum creatinine (Cr) levels exceed 2.0 mg/dL, chronic obstructive pulmonary disease, or chronic arthritis. Also excluded were those with an accompanying endocrine disease such as hypothyroidism, hyperparathyroidism, or Cushing's syndrome. We analyzed the results from 140 subjects as 8 of the original 150 subjects did not undergo testing despite their agreement to do so, and 2 subjects were confirmed to have hypothyroidism and idiopathic hypoparathyroidism following study completion. This study was approved by the Institutional Review Board at Kangwon National University Hospital.
- Quantification of CAC scores and laboratory measurements
- We carried out our interviews and physical examinations together with a review of the subjects' medical records. We examined if the subjects had cardiovascular disease, history of smoking, and the duration of diabetes, and obtained individual body mass index. We also measured the waist circumference of each subject and measured blood pressure twice, 5 minutes apart, with the patient in a stable state, using a hemodynamometer (Omron HEM-780; Omron Healthcare Co. Ltd., Kyoto, Japan). The mean value of the two measurements was then used in analysis. For the CAC score, we measured both area and volume using multi-slice computed tomography (MSCT) (LightSpeed Plus; GE Medical Systems, Milwaukee, WI, USA), and used the measured value for volume in our statistical process. Conditions under which we collected information when taking the MSCT were similar to those employed in our previous article [16]. Blood sampling was done following an 8-hour fast. General chemistry, serum lipid test, microalbuminuria, and high sensitivity C-reactive protein (hs-CRP) tests were carried out. For hs-CRP testing, we used Latex agglutination method that can detect levels as low as 0.01 mg/dL. If a patient was affected by an acute episode, laboratory results for at least 1 month following complete resolution of the episode were excluded from the data collection.
- Genotyping
- We analyzed genotype using a commercialized 5' nuclease assay method. We separated the buffy coat from the subject's venous blood sample and, then stored them at -80℃. We extracted genomic DNA from the above samples using a DNA purification kit. SNP genotyping of rs1044498 in exon 4 of the ENPP1 gene was performed using allelic discrimination TaqMan® SNP Genotyping Assays (Assay ID: C_1207994_20; Applied Biosystems, Foster City, CA, USA). All primers and probes were obtained from Applied Biosystems. Real-time PCR was carried out in a final volume of 20 µL, containing a 2 µM concentration of each probe, 5 µM forward and reverse primers, 1 × PCR Master Mix (Applied Biosystems), and 10 ng genomic DNA. Using the 7300 real-time PCR system (Applied Biosystems), we measured fluorescence intensity, and using automated software, we determined genotype.
- Statistical analyses
- In genotype analysis, we ran χ2 verification to check if the allelic frequency of the gene conformed to the Hardy-Weinberg equilibrium. To check if an association existed between gene polymorphism and the CAC score, we performed multiple regression analysis taking age, body mass index, waist circumference, and the duration of diabetes, which are known as influencing factors on coronary arterial calcification, as covariates.
- For comparison of wild type and variant, we matched to each patient with the KQ genotype to a respective control with the KK genotype using a stratified random selection method by age, gender, and the duration of diabetes, owing to too small a number of subjects with the KQ genotype compared to that of the 121KK genotype (Fig. 1). This design was adopted from the study by Eller et al. [13]. Differences in mean values between the two groups with different ENPP1 genotypes were determined using unpaired Student's t-test, and those of medians with the Mann-Whitney U test. The χ2 test was used to compare categorical variables such as smoking history and medications used at enrollment. We used the SPSS version 12.0 software program (SPSS Inc., Chicago, IL, USA) and determined P value significance for values less than 0.05.
METHODS
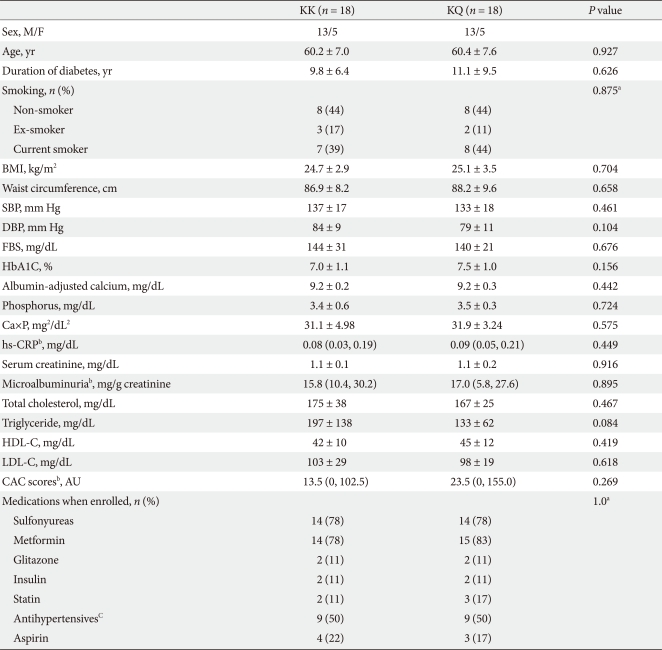
- The mean age of the subjects was 62.1 ± 8.2 years and the mean duration of diabetes was 9.4 ± 7.1 years. The mean body mass index was 25.3 ± 3.0 kg/m2 and mean value of waist circumference was 89.0 ± 7.4 cm. Detailed characteristics of the subjects are shown on Table 1. A total of 46 patients (32.9%) had no CAC (< 0 AU, Agatston Unit); the remaining 94 patients (67.1%) had varying degrees of CAC. According to the guidelines on the interpretation of calcium scores proposed by Rumberger et al. [17], lesions were minimal (score, 1 to 10) in 16 subjects (11.4%), mild (score, 11 to 100) in 34 subjects (24.3%), moderate (score, 101 to 400) in 31 subjects (22.1%), and severe with a high probability for stenosis (score, > 400) in 13 subjects (9.3%). The median CAC score was 16.5 AU (interquartile range, 0 to 128.8).
- The allele distribution of study subjects was in Hardy-Weinberg equilibrium (χ2 = 0.66, P = 0.72). The frequency of minor allelic gene variation was 0.064. The distribution of the ENPP1 K121Q alleles in the study subjects was as follows: 122/140 (87.1%) were homozygous for the KK genotype, 18/140 (12.9%) were heterozygous, and there were no homozygous subjects for the QQ genotype (Fig. 1). There were no significant differences in the clinical and biochemical characteristics and CAC scores between the KK genotype groups and KQ genotype groups (Tables 2 and 3).
- Each patient with the KQ genotype (n = 18) was matched with a control subject with the KK genotype by age, gender, and duration of diabetes in a 1:1 study design (Fig. 1), as described in the methods section. There were no significant differences in blood pressure, A1C levels, smoking habits, serum calcium, serum phosphate, microalbuminuria, lipid profiles, and use of oral antidiabetic medications and statins between the two groups with different ENPP1 genotypes. We did not find any significant differences in the CAC scores between the two ENPP1 genotype groups (Table 4).
RESULTS
- To summarize the results of this study, coronary artery calcification was observed in 67% of the study subjects, and no significant association was observed between ENPP1 K121Q genotypes and coronary artery calcification scores.
- Vascular calcification is widespread in patients with atherosclerosis, T2DM, and end-stage renal disease, although the mechanisms may differ in each of these disease contexts. As in skeletal calcifications, vascular calcification is governed by positive and negative regulators, and under normal conditions, constitutive inhibition dominates. The balance between levels of inorganic phosphate and pyrophosphates determine whether hydroxyapatite mineral crystals form and grow in cartilage and bone. Under certain physiological conditions, calcification is inhibited by extracellular PPi through cleavage of nucleotide triphosphates by ENPP1 and cellular export. The extracellular PPi levels are reduced, and calcification can proceed. As described earlier, there have been several in vitro and in vivo studies demonstrating associations between vascular calcification and a deficiency of ENPP1 and/or mutations of ENPP1 genotypes; however, we know of no previous studies that have investigated the association of the ENPP1 K121Q polymorphism with the severity of coronary artery calcifications in T2DM patients, or even in healthy subjects.
- To date, few clinical studies have investigated the relationship between vascular calcification and genetic polymorphisms, although these have been extensively demonstrated in non-diabetic subjects. In type 2 diabetic patients, several genetic variations related to calcium metabolism are reportedly associated with coronary artery calcifications. Polymorphisms of α2-Heremans-Schmid (AHSG) glycoprotein, traditionally known as fetuin-A, which is an important mineralization inhibitor, were associated with CAC scores in European Americans with T2DM [18]. It was thought that this result was consistent with the known biological role of AHSG in vascular calcification. The concentration of circulating fetuin-A protein has been shown to predict the risk of vascular calcification, inflammation, and all-cause and cardiovascular disease mortality. This is especially true for patients with end-stage renal disease [19]. However, this association was not consistent across various ethnic populations. In the recent Diabetes Heart Study [20], bone morphogenetic protein 7 gene polymorphisms were reported to be associated with inverse relationships between vascular calcification and bone mineral density. Bone morphogenetic protein has been proposed to play an inhibitory role in vascular calcification, but its inhibitory effect has not been extensively studied.
- Our data indicate that the 121Q variant of the ENPP1 gene is not associated with coronary artery calcification scores in patients with T2DM. This may be a result of several factors, including sample size, concurrent medications, unknown disturbed mineral metabolism, and other hormonal and genetic effects. The Q allele frequency in our study was 0.064, and there was no QQ homozygote. This very low minor allele frequency in our study subjects is similar to that recently reported in a study of a Korean cohort population [14]. These authors reported that the minor allele frequency of ENPP1 121Q is 0.031 in healthy subjects and 0.084 in type 2 diabetic patients, with no QQ homozygote. This frequency was lower than among Caucasians (23.2-36.4%) [9,10], South Asian Indians (27.5-34.2%) [6], and Chinese (18.8%) [21]. We assume that these differences of allele frequencies among ethnic groups might play certain roles in the association of CAC scores and ENPP1 genotypes. Small sample size and the lack of homozygous carriers of the ENPP1 K121Q genotype is an important limitation of our study.
- Medications at enrollment, which included statins, may also affect vascular pathology. However, there are no reports that statins might influence the forming of CAC and the progression of calcium deposition in vascular beds. Statins significantly lower low density lipoprotein cholesterol and reduce atheroma formation but are largely powerless against extensive calcification [22]. Coronary artery calcification is common and progressive in young adults with end-stage renal disease who have been undergoing dialysis for years [23]. Whether a disturbed mineral metabolism might exist in type 2 diabetic patients with apparently normal serum creatinine levels is largely unknown. In our study, there was no difference in serum calcium or phosphate level between the genotype groups. Calcium-phosphate product, a marker of extraskeletal calcification, which should be maintained at less than 55 mg2/dL2 in patients with chronic kidney disease, was also within normal range and showed no differences between the two genotype groups.
- Lee et al. [14] reported that ENPP1 K121Q polymorphisms are associated with T2DM and that the Q allele is associated with increased aortic arch calcification in a Korean population. However, they did not measure coronary artery calcification scores, as in our study, and unfortunately the measurement of calcification was not quantitative but qualitative, which they mentioned as a limitation of their study.
- The limitations of this study are, first, a possible selection bias due to the fact that our subjects were not from the general population group but were visiting patients to a single hospital. However, the possibility of selection bias for genotype in our study is less likely because the distribution of genotype was within the Hardy-Weinberg equilibrium. Also, the minor allele frequency in our study is within the range reported by another study of a Korean population [14]. Secondly, the study subjects were medicated with several anti-diabetics, antihypertensives, and statins; however, there were no differences in medications at enrollment between comparison groups. In fact, the medication might affect the vascular calcification process; however, for ethical reasons, a non-medicated study could not be allowed in patients with T2DM. Third, we had statistical difficulties in comparing the groups due to low authenticity caused by the relatively small population and due to a low frequency of gene variants. These problems could be resolved with further study using a greater number of subjects. In conclusion, we did not observe an association between K121Q polymorphism of ENPP1 and CAC scores in Korean type 2 diabetic patients.
DISCUSSION
- 1. Giachelli CM, Speer MY, Li X, Rajachar RM, Yang H. Regulation of vascular calcification: roles of phosphate and osteopontin. Circ Res 2005;96:717-722. PubMed
- 2. Doherty TM, Fitzpatrick LA, Inoue D, Qiao JH, Fishbein MC, Detrano RC, Shah PK, Rajavashisth TB. Molecular, endocrine, and genetic mechanisms of arterial calcification. Endocr Rev 2004;25:629-672. ArticlePubMed
- 3. Budoff MJ, Achenbach S, Blumenthal RS, Carr JJ, Goldin JG, Greenland P, Guerci AD, Lima JA, Rader DJ, Rubin GD, Shaw LJ, Wiegers SE. American Heart Association Committee on Cardiovascular Imaging and Intervention. American Heart Association Council on Cardiovascular Radiology and Intervention. American Heart Association Committee on Cardiac Imaging, Council on Clinical Cardiology. Assessment of coronary artery disease by cardiac computed tomography: a scientific statement from the American Heart Association Committee on Cardiovascular Imaging and Intervention, Council on Cardiovascular Radiology and Intervention, and Committee on Cardiac Imaging, Council on Clinical Cardiology. Circulation 2006;114:1761-1791. ArticlePubMed
- 4. Qu W, Le TT, Azen SP, Xiang M, Wong ND, Doherty TM, Detrano RC. Value of coronary artery calcium scanning by computed tomography for predicting coronary heart disease in diabetic subjects. Diabetes Care 2003;26:905-910. ArticlePubMedPDF
- 5. Ruf N, Uhlenberg B, Terkeltaub R, Nurnberg P, Rutsch F. The mutational spectrum of ENPP1 as arising after the analysis of 23 unrelated patients with generalized arterial calcification of infancy (GACI). Hum Mutat 2005;25:98Article
- 6. Abate N, Chandalia M, Satija P, Adams-Huet B, Grundy SM, Sandeep S, Radha V, Deepa R, Mohan V. ENPP1/PC-1 K121Q polymorphism and genetic susceptibility to type 2 diabetes. Diabetes 2005;54:1207-1213. ArticlePubMedPDF
- 7. Bacci S, Ludovico O, Prudente S, Zhang YY, Di Paola R, Mangiacotti D, Rauseo A, Nolan D, Duffy J, Fini G, Salvemini L, Amico C, Vigna C, Pellegrini F, Menzaghi C, Doria A, Trischitta V. The K121Q polymorphism of the ENPP1/PC-1 gene is associated with insulin resistance/atherogenic phenotypes, including earlier onset of type 2 diabetes and myocardial infarction. Diabetes 2005;54:3021-3025. ArticlePubMedPDF
- 8. Bochenski J, Placha G, Wanic K, Malecki M, Sieradzki J, Warram JH, Krolewski AS. New polymorphism of ENPP1 (PC-1) is associated with increased risk of type 2 diabetes among obese individuals. Diabetes 2006;55:2626-2630. ArticlePubMedPDF
- 9. Pizzuti A, Frittitta L, Argiolas A, Baratta R, Goldfine ID, Bozzali M, Ercolino T, Scarlato G, Iacoviello L, Vigneri R, Tassi V, Trischitta V. A polymorphism (K121Q) of the human glycoprotein PC-1 gene coding region is strongly associated with insulin resistance. Diabetes 1999;48:1881-1884. ArticlePubMedPDF
- 10. Gu HF, Almgren P, Lindholm E, Frittitta L, Pizzuti A, Trischitta V, Groop LC. Association between the human glycoprotein PC-1 gene and elevated glucose and insulin levels in a paired-sibling analysis. Diabetes 2000;49:1601-1603. ArticlePubMedPDF
- 11. Kubaszek A, Pihlajamaki J, Karhapaa P, Vauhkonen I, Laakso M. The K121Q polymorphism of the PC-1 gene is associated with insulin resistance but not with dyslipidemia. Diabetes Care 2003;26:464-467. ArticlePubMedPDF
- 12. Endler G, Mannhalter C, Sunder-Plassmann H, Schillinger M, Klimesch A, Exner M, Kapiotis S, Meier S, Kunz F, Raiger E, Huber K, Wagner O, Sunder-Plassmann R. The K121Q polymorphism in the plasma cell membrane glycoprotein 1 gene predisposes to early myocardial infarction. J Mol Med 2002;80:791-795. ArticlePubMedPDF
- 13. Eller P, Hochegger K, Feuchtner GM, Zitt E, Tancevski I, Ritsch A, Kronenberg F, Rosenkranz AR, Patsch JR, Mayer G. Impact of ENPP1 genotype on arterial calcification in patients with end-stage renal failure. Nephrol Dial Transplant 2008;23:321-327. ArticlePubMed
- 14. Lee JE, Choi YK, Seo HA, Jeon JH, Jeong JY, Moon SS, Kim JG, Kim BW, Kim SW, Min Yoo, Kim JY, Lee IK. Impact of ENPP1 and MMP3 gene polymorphisms on aortic calcification in patients with type 2 diabetes in a Korean population. Diabetes Res Clin Pract 2010;88:87-96. ArticlePubMed
- 15. Li J, Galvin HK, Johnson SC, Langston CS, Sclamberg J, Preston CA. Aortic calcification on plain chest radiography increases risk for coronary artery disease. Chest 2002;121:1468-1471. ArticlePubMed
- 16. Jung HH, Kim SW, Han H. Inflammation, mineral metabolism and progressive coronary artery calcification in patients on haemodialysis. Nephrol Dial Transplant 2006;21:1915-1920. ArticlePubMed
- 17. Rumberger JA, Brundage BH, Rader DJ, Kondos G. Electron beam computed tomographic coronary calcium scanning: a review and guidelines for use in asymptomatic persons. Mayo Clin Proc 1999;74:243-252. ArticlePubMed
- 18. Lehtinen AB, Burdon KP, Lewis JP, Langefeld CD, Ziegler JT, Rich SS, Register TC, Carr JJ, Freedman BI, Bowden DW. Association of alpha2-Heremans-Schmid glycoprotein polymorphisms with subclinical atherosclerosis. J Clin Endocrinol Metab 2007;92:345-352. PubMed
- 19. Ketteler M, Bongartz P, Westenfeld R, Wildberger JE, Mahnken AH, Bohm R, Metzger T, Wanner C, Jahnen-Dechent W, Floege J. Association of low fetuin-A (AHSG) concentrations in serum with cardiovascular mortality in patients on dialysis: a cross-sectional study. Lancet 2003;361:827-833. ArticlePubMed
- 20. Freedman BI, Bowden DW, Ziegler JT, Langefeld CD, Lehtinen AB, Rudock ME, Lenchik L, Hruska KA, Register TC, Carr JJ. Bone morphogenetic protein 7 (BMP7) gene polymorphisms are associated with inverse relationships between vascular calcification and BMD: the Diabetes Heart Study. J Bone Miner Res 2009;24:1719-1727. ArticlePubMedPMC
- 21. Chen MP, Chung FM, Chang DM, Tsai JC, Huang HF, Shin SJ, Lee YJ. ENPP1 K121Q polymorphism is not related to type 2 diabetes mellitus, features of metabolic syndrome, and diabetic cardiovascular complications in a Chinese population. Rev Diabet Stud 2006;3:21-30. ArticlePubMedPMC
- 22. Nicoll R, Henein M. Extensive coronary calcification: a clinically unrecognised condition. Curr Vasc Pharmacol 2010;8:701-705. ArticlePubMed
- 23. Goodman WG, Goldin J, Kuizon BD, Yoon C, Gales B, Sider D, Wang Y, Chung J, Emerick A, Greaser L, Elashoff RM, Salusky IB. Coronary-artery calcification in young adults with end-stage renal disease who are undergoing dialysis. N Engl J Med 2000;342:1478-1483. ArticlePubMed
REFERENCES

BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; Ca×P, calcium phosphorus product; FBS, fasting blood sugar; HbA1C, hemoglobin A1C; hs-CRP, high sensitivity C-reactive protein; HDL-C, high density lipoprotein cholesterol; LDL-C, low density lipoprotein cholesterol; CAC, coronary artery calcium.
aMedian and inter-quartile ranges of hs-CRP, microalbuminuria, CAC scores, bAntihypertensives included ACE inhibitor, Angiotensin receptor blocker ARB, Calcium-channel blocker, and thiazides.
BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; FBS, fasting blood sugar; HbA1C, hemoglobin A1C; hs-CRP, high sensitivity C-reactive protein; HDL-C, high density lipoprotein cholesterol; LDL-C, low density lipoprotein cholesterol; CAC, coronary artery calcium.
aχ2 test, bMedian and inter-quartile ranges of hs-CRP, microalbuminuria, and CAC scores, cAntihypertensives included ACE inhibitor, Angiotensin receptor blocker ARB, Calcium-channel blocker, and thiazides.
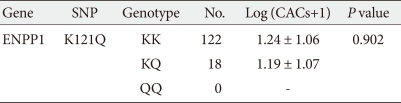

Figure & Data
References
Citations
- Evaluation of NPP1 as a Novel Biomarker of Coronary Artery Disease: A Pilot Study in Human Beings
Amir Hooshang Mohammadpour, Saeed Nazemi, Fatemeh Mashhadi, Atefeh Rezapour, Mohammad Afshar, Sepideh Afzalnia, Afsaneh Mohammadi, Hamid Reza Mashreghi Moghadam, Maryam Moradian, Seyed Mohammad Hasan Moallem, Saeed Falahaty, Azadeh Zayerzadeh, Sepideh Ely
Advanced Pharmaceutical Bulletin.2018; 8(3): 489. CrossRef - ENPP1 121Q functional variant enhances susceptibility to coronary artery disease in South Indian patients with type 2 diabetes mellitus
S. Sumi, Surya Ramachandran, V RamanKutty, Maulin M. Patel, T. N. Anand, Ajit S Mullasari, C. C. Kartha
Molecular and Cellular Biochemistry.2017; 435(1-2): 67. CrossRef - Genetics in Arterial Calcification
Frank Rutsch, Yvonne Nitschke, Robert Terkeltaub, Dwight A. Towler
Circulation Research.2011; 109(5): 578. CrossRef - Distribution of allelic variants of genes inhibitors and activators ectopic calcification in patients with acute coronary syndrome
V. Yu. Harbuzova, O. A. Obukhova, I. O. Rozumenko, Ye. I. Dubovyk, T. M. Oleshko, Ye. A. Harbuzova, D. V. Shvachko, O. V. Ataman
Faktori eksperimental'noi evolucii organizmiv.1970; 21: 306. CrossRef
 PubReader
PubReader Cite
Cite- Figure
-

- Related articles
-
- Optimal Low-Density Lipoprotein Cholesterol Level for Primary Prevention in Koreans with Type 2 Diabetes Mellitus
- Non-Alcoholic Fatty Liver Disease with Sarcopenia and Carotid Plaque Progression Risk in Patients with Type 2 Diabetes Mellitus
- Intensified Multifactorial Intervention in Patients with Type 2 Diabetes Mellitus
- A Real-World Study of Long-Term Safety and Efficacy of Lobeglitazone in Korean Patients with Type 2 Diabetes Mellitus
- Advanced Liver Fibrosis Is Associated with Chronic Kidney Disease in Patients with Type 2 Diabetes Mellitus and Nonalcoholic Fatty Liver Disease



