Is A1C Variability an Independent Predictor for the Progression of Atherosclerosis in Type 2 Diabetic Patients?
Article information
Abstract
Background
Little is known about the relative contribution of long-term glycemic variability to the risk of macrovascular complications in type 2 diabetes. This study was conducted to evaluate the effect of A1C variability on the progression of carotid artery intima-media thickness (IMT) in type 2 diabetic patients.
Methods
Among type 2 diabetic patients who visited Hallym University Sacred Heart Hospital from March 2007 to September 2009, 120 patients who had carotid artery IMT measured annually and A1C checked every three months for at least one year were analyzed. Individual A1C variability was defined as the standard deviation (SD) of five A1C levels taken every three months for approximately one year. Change in IMT was defined as an increase in IMT on follow-up measurement. The association between the SD of A1C and changes in IMT was evaluated.
Results
With greater A1C variability, there was a greater increase in the mean IMT (r = 0.350, P < 0.001) of the carotid artery. After adjusting for confounding factors that may influence IMT, A1C variability was significantly associated with the progression of IMT (r = 0.222, P = 0.034). However, the SD of A1C was not a significant independent risk factor for the progression of IMT in multiple regression analysis (β = 0.158, P = 0.093).
Conclusion
Higher A1C variability is associated with IMT progression in type 2 diabetic patients; however, it is not an independent predictor of IMT progression. Overall glycemic control is the most important factor in the progression of IMT.
INTRODUCTION
Diabetes is characterized by a high incidence of accelerated atherosclerosis [1]. Although researchers have examined the roles of numerous factors involved in the macrovascular complications of diabetes, a precise judgment of their individual contributions remains challenging [2]. Diabetic complications are mainly dependent on dysglycemia [1,3], and diabetes is characterized by both sustained chronic hyperglycemia and acute glucose fluctuation, both of which lead to diabetic complications [4].
Similar glycemic levels can be generated by different glucose profiles [4,5]. Among patients with similar glycemic levels, those with larger glucose variability might be at greater risk for developing chronic complications [4-6]. There is firm evidence that postprandial glycemia is a stronger risk factor for the development of macrovascular complications than are fasting or preprandial concentrations [7,8]. Therefore, diabetic management primarily focuses on the attenuation of glycemic excursions following meals with the belief that glycemic control reduces the risk of cardiovascular disease [9]. However, little is known about the relative contribution of long-term glycemic variability to the risk of developing macrovascular complications in type 2 diabetes.
Intima-media thickness (IMT) is a well-described surrogate marker for cardiovascular risk [10-13]. In cross-sectional analyses, increased IMT was correlated with myocardial infarction and stroke [14].
Understanding the risks of long-term glycemic variability is fundamental to the management of diabetes. In this study, we evaluated the relationship between A1C variability and the progression of IMT in type 2 diabetic patients.
METHODS
Subjects
Among type 2 diabetic patients who visited Hallym University Sacred Heart Hospital from March 2007 to September 2009, patients who had annual carotid artery IMT measurements and who had their A1C level checked every three months for at least one year were enrolled. We analyzed data from patients who had visited the clinic on more than three consecutive occasions prior to enrollment since biochemical parameters such as A1C show marked changes after initial treatment (n = 120).
Exclusion criteria were type 1 diabetes; history or clinical evidence of coronary artery disease or cerebral or peripheral vascular disease; renal dysfunction (defined as creatinine blood level ≥ 2.0 mg/dL); hepatic dysfunction (defined as alanine aminotransferase and/or aspartate aminotransferase blood level ≥ 3 × the upper normal limit); use of glucocorticoids; pregnancy; severe concomitant disease such as cancer, infection, Cushing's syndrome, acromegaly, or any other disorder likely to alter glycemia; primary hypercholesterolemia, hypothyroidism or hyperthyroidism; use of any hormonal drugs; and alcoholism or drug abuse.
Hypertension was defined as systolic blood pressure of at least 140 mm Hg and/or a diastolic blood pressure of at least 90 mm Hg, use of antihypertensive drugs, or a combination of these parameters. Dyslipidemia was defined as an low density lipoprotein cholesterol (LDL-C) level ≥ 100 mg/dL or an high density lipoprotein cholesterol (HDL-C) level < 40 mg/dL for men, < 50 mg/dL for women, or the use of lipid-lowering drugs. Proteinuria was defined as a 24 hour albuminuria ≥ 30 mg/day. Retinopathy was defined by at least one retinal microaneurysm with or without hemorrhages, venous beading, soft exudates, or intraretinal microvascular abnormalities. Neuropathy was defined as the presence of bilateral pain and paresthesias in the lower limbs or the presence of a positive finding on the current perception threshold test. The protocol was approved by the Ethics Committee of Hallym University, and informed written consent was obtained from each participant.
Clinical characteristics
Height, weight, and blood pressure were measured for each participant, with blood pressure measured twice in a sitting position using a sphygmomanometer at the level of the heart. The average of the measurements was used as the reference data. Body weight and height were measured in the morning with participants wearing light clothing. Body mass index (BMI) was calculated as body weight in kilograms divided by height in meters squared (kg/m2). Waist circumference was determined using a measuring tape placed midway between the lowest rib and the iliac crest, with the participant standing on a flat floor with feet 30 cm apart.
Biochemical characteristics
Blood samples were collected from subjects after more than 10 hours of fasting. A1C was determined using high-performance liquid chromatography (Variant II; Bio-Rad, Hercules, CA, USA). Plasma glucose levels were measured immediately after sampling with an autoanalyzer, using the hexokinase method (Hitachi 747; Roche, Montclair, NJ, USA). Serum insulin levels were determined using an INS-IRMA Kit (BioSource Europe S.A., Nevelles, Belgium), and serum total cholesterol and HDL-C were measured using a direct enzymatic method (Hitachi 747; Daiichi, Tokyo, Japan). Serum triglyceride levels were measured using an enzymatic colorimetric method (Hitachi 747; Roche, Japan/Germany), and LDL-C was calculated using the Friedewald formula, i.e., total cholesterol - {(triglyceride/5) + HDL-C}. Insulin resistance was estimated after fasting using the homeostasis model assessment method (HOMA-IR): HOMA-IR = fasting insulin (µU/mL) × fasting plasma glucose (mmol/L) / 22.5. Individual A1C variability was defined as the standard deviation (SD) of five A1C levels taken every three months for about one year.
Carotid artery IMT
We measured IMT at baseline and after 12 months of follow-up. Change in IMT was defined as an increase in IMT on the follow-up measurement. IMT was measured by one examiner using a B-mode ultrasound with an 8 MHz linear probe (Sequoia C512; Siemens, Munich, Germany). IMT was measured at three points of the common carotid artery 1 cm proximal to the bifurcation, and the mean value of six measurements from the right and left carotid arteries was used. Reproducibility was further tested, and the day-to-day coefficient of variation was 4.5% for carotid IMT measurements. Moreover, when calcifications or plaques showed heterogeneity in the area of IMT determination, measurements were performed proximally in order to exclude plaques.
Statistics
Descriptive statistics are presented as mean values ± SD. Subjects were divided into three groups according to the individual A1C variability (SD of five A1C levels taken every three months for about one year).
Comparisons of clinical and physiological characteristics of each group were performed using ANOVA.
Partial correlation analysis was used to assess the significance of the relationship between A1C variability and the progression of carotid IMT after controlling for age, gender, diabetes duration, menopause status, smoking status, hypertension status, dyslipidemia status, albuminuria status, BMI, waist circumference, blood pressure, LDL-C level, HDL-C level, HOMA-IR, fasting and postprandial glucose, mean A1C, baseline A1C, and use of medications likely to alter IMT (thiazolidinediones, statins, calcium channel blockers, angiotensin converting enzyme inhibitors, angiotensin receptor blockers, anti-platelet agents). The inclusion of the controlling factors in partial correlation analysis removed the possibility of their contributions to the outcome [15].
Moreover, independent risk factors for progression of IMT were identified using multiple linear regression analysis. We selected all of the variables which showed a potential association (P < 0.20) with the progression of IMT in the correlation analysis [16]. We also entered known cardiovascular risk factors such as gender, BMI, diabetes duration, blood pressure, baseline IMT, and lipid levels into the model.
All statistical analysis was performed using SPSS for Windows 11.5 (SPSS Inc., Chicago, IL, USA), and P values less than 0.05 were considered to be statistically significant.
RESULTS
Table 1 shows the baseline clinical and biochemical characteristics of the subjects. The mean baseline IMT of the subjects was 0.85 ± 0.12 mm, and the mean progression of IMT was 0.04 ± 0.09 mm. The mean follow-up period was 369.7 ± 15.2 days.
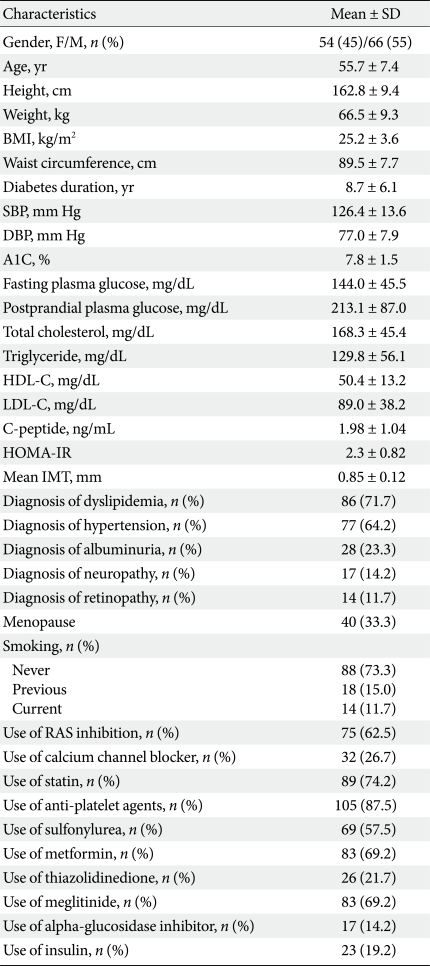
Baseline clinical and biochemical data
Change of A1C over 12 months
Fig. 1A shows the changes in A1C level at three month intervals, illustrating that the levels gradually decreased over 12 months. Fig. 1B demonstrates the changes in glucose level in the three groups with different A1C variabilities over a 12 month period. The group with the highest A1C variability had the highest baseline A1C and experienced the greatest decrease in plasma glucose level, while the group with the lowest A1C variability had the lowest baseline A1C and had stable plasma glucose levels over the study period (Table 2, Fig. 1B).
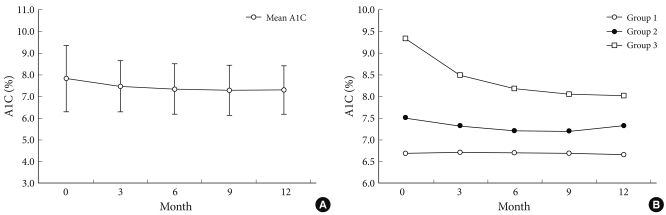
Changes in A1C levels during the 12 months. (A) All subjects. (B) Groups according to A1C variability. Group 1, low A1C variability group; Group 2, intermediate A1C variability group; Group 3, high A1C variability group.
Clinical and biochemical data according to A1C variability
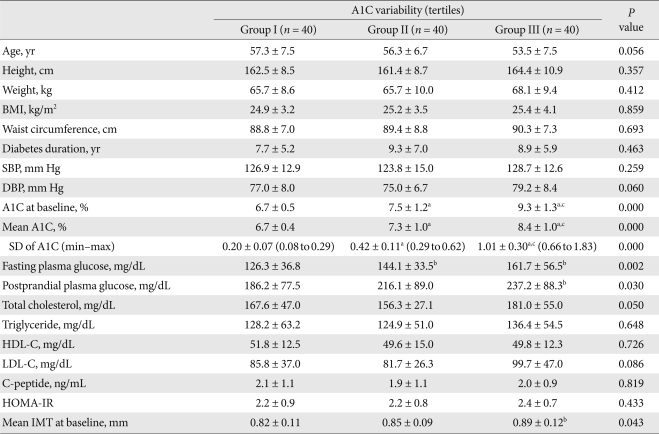
Clinical and biochemical characteristics according to A1C variability
Tables 2, 3 demonstrate the clinical and biochemical characteristics of the three groups with different A1C variabilities. There were no differences in age, body size, duration of diabetes mellitus, blood pressures, lipid profiles, insulin secretory function, insulin resistance, diagnoses of concurrent diseases, or diabetes-related drug history among the groups. However, the group with the greatest A1C variability had the highest baseline and mean A1C level compared to those of the other groups (Table 2). The A1C variability was also closely related to the mean A1C of all patients (r = 0.676, P < 0.001).
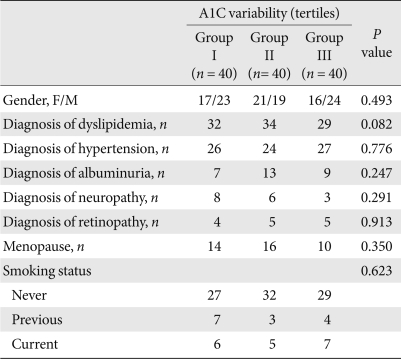
Clinical data according to A1C variability
A1C variability and progression of IMT
We found that, with greater A1C variability, there was a greater increase in the IMT (r = 0.350, P < 0.001) of the carotid artery (Fig. 2). Although this relationship weakened after adjusting for confounding factors that can influence the progression of IMT, it remained statistically significant (r = 0.222, P = 0.034, Fig. 2).
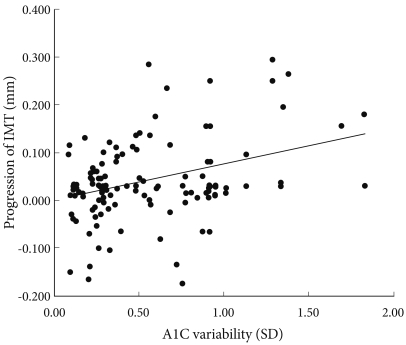
Correlation between A1C variability and progression of IMT of the carotid artery. r = 0.350, P < 0.001 (r = 0.222, P = 0.034 after adjusting for confounding factors). IMT, intimamedia thickness; SD, standard deviation.
Multiple regression analysis of the progression of IMT
In order to evaluate factors that influence the progression of IMT, multiple regression analysis was performed. Mean A1C (β = 0.314, P = 0.043) and fasting plasma glucose (β = 0.298, P = 0.046) were found to be independent predictors of the progression of IMT (Table 4). However, the SD of A1C was not a significant independent risk factor for the progression of IMT in multiple regression analysis (β = 0.158, P = 0.093).

Multiple regression analysis of the progression of carotid IMT
DISCUSSION
This study demonstrates that the long-term variability in A1C level has no significant influence on the progression of carotid atherosclerosis in patients with type 2 diabetes. Although A1C variability over 12 months was found to be associated with the progression of IMT, overall glycemic control is the most important factor in the progression of IMT.
Recently, Kilpatrick et al. [5] concluded that A1C variability may be an additional risk factor for the development of microvascular complications in type 1 diabetic patients. Previously, they had reported that daily glucose variability, as measured on a quarterly eight-point glucose profile, was not associated with the development or progression of retinopathy or nephropathy [17]. It has also been suggested that A1C variability might play an important role in the development of long-term macrovascular complications in type 1 diabetes [6].
Few studies have been conducted to evaluate the relationship between glycemic variability and the development of macrovascular complications in type 2 diabetics, the major cause of diabetic mortality. Previously, Muggeo et al. [18] reported that long-term instability in fasting plasma glucose concentrations was an independent predictor of cardiovascular-related five-year mortality in elderly type 2 diabetic patients with a mean age of 80 years and a short life expectancy. Subsequently, they confirmed these result over a period of 10 years in type 2 diabetics with an age range of 56-74 years [17]. The relationship between the variability of fasting plasma glucose and cardiovascular mortality could result from more frequent hypoglycemia, which predisposes patients to adverse outcomes [19,20].
When patients are exposed to hyperglycemia more frequently and for longer periods, more hyperglycemia-related complications are likely to develop because frequent exposure to hyperglycemia leads to excessive protein glycation and increased oxidative stress [4]. Also, there is data on the effect of glycemic changes on free radical production [21]. Moreover, sustained hyperglycemia has lasting effects, and patients are at higher risk for complications [22,23]. Therefore, the harmful effect of glycemic variability may be mediated through a mechanism similar to that underlying "metabolic memory" [22,24].
It remains unclear whether long-term glucose variability (week-to-week, as measured by A1C) has a similar influence on the development or progression of macrovascular complications in type 2 diabetics to that of short-term glucose instability (day-to-day, as measured by fasting plasma glucose). Our study demonstrates that long-term glucose variability, measured by A1C variability, has no significant influence on the progression of carotid atherosclerosis in patients with type 2 diabetes. Therefore, we conclude that A1C variability has no influence on the development of cardiovascular events. Instead of A1C variability, overall glycemic control was revealed to be the important factor in determining the progression of carotid atherosclerosis in type 2 diabetes.
In our study, there are several possible reasons that A1C variation itself was not revealed as an independent risk factor for the progression of atherosclerosis. First, this study was conducted on a relatively low-risk group for cardiovascular diseases (no past history of cardiovascular diseases, relatively good glucose control state at baseline, limited lipid and blood pressure problems, and a small number of smokers). Therefore, the progression of atherosclerosis in this group may have been slow. Moreover, we did not exclude patients receiving medications likely to alter IMT (statins, ACE inhibitors, angiotensin receptor blockers, and anti-platelet agents). Finally, 12 months is a relatively short period in which to assess meaningful progression of carotid atherosclerosis.
In our study, regression of IMT was found in 28 subjects. These patients had a shorter duration of diabetes (7.1 ± 4.1 vs. 9.1 ± 6.5 year, P = 0.049) and a lower mean A1C level (7.1 ± 0.9 vs. 7.8 ± 1.1%, P = 0.020) compared to those of subjects with progression of IMT. These results suggest that diabetic patients of long duration and poor glycemic control are prone to atherosclerosis development [15].
Frequent hypoglycemia predisposes patients to cardiovascular events in type 2 diabetes [20]. The stability of fasting plasma glucose seems to be protective and variability seems to be harmful. Moreover, postprandial glucose is a predictor of cardiovascular disease and its measurement is the other component of glycemic variability [25,26]. Change in IMT was significantly correlated with change in postprandial glucose rather than that of fasting glucose [9]. A1C is a standard clinical assessment of glycemia and is the basis of most data relating glycemic control to diabetic complications [27,28]. A1C reflects mean blood glucose levels including both fasting and postprandial glucose levels [25] and is not affected by glycemic instability [29]. Therefore, it is possible that A1C variability is not a sensitive measure for detecting the effects of hypoglycemia.
There is a tendency for greater A1C variability in subjects with poor glycemic control, and our study showed a strong correlation between A1C variability and baseline A1C as well as mean A1C over 12 months. After adjusting for glucose level, the correlation between A1C variability and IMT progression was attenuated.
We analyzed subjects with poor glycemic control (n = 40). As a result, the correlation between A1C variability and the progression of IMT was stronger than that of all subjects (r = 0.413, P = 0.008). Although this relationship was weakened after adjusting for confounding factors that can influence the progression of IMT, it remained statistically significant (r = 0.329, P = 0.012). However, in multiple regression analysis, A1C variability was not a significant independent risk factor for the progression of IMT (β = 0.256, P = 0.254).
In our study, glycemic status was a significant determining factor for the progression of IMT in type 2 diabetic patients. This finding indicates that blood glucose control may play the principal role in interventions to inhibit an increase of IMT in type 2 diabetics. Although overall glycemic control is the most important factor in the progression of IMT, this does not necessarily mean that glycemic variability is not important in determining outcomes in type 2 diabetes. Global anti-diabetic strategy should be aimed first at improving glycemic control and then at minimizing the different components of dysglycemia (especially hypoglycemia) in order to avoid excess risk of long-term complications [30].
There are several possible limitations in our study. First, the subjects were not randomly selected and the study was prospectively designed. Moreover, the modifications in individual medication dosages over the 12 months were not reflected in the results.
In conclusion, relatively long-term variability in A1C levels appears to be associated with progression in IMT over 12 months. However, the A1C variability itself was not revealed as an independent risk factor for the increase in IMT during the 12 month study period. Rather than A1C variability, overall glycemic control was the most important factor for the progression of carotid IMT. However, considering the gradual increase in IMT, a longer follow-up period may be needed to assess A1C variability as an independent predictor of progression of atherosclerosis in type 2 diabetic patients.
ACKNOWLEDGEMENT
This work was supported by the Health Fellowship Foundation (2007).