- Current
- Browse
- Collections
-
For contributors
- For Authors
- Instructions to authors
- Article processing charge
- e-submission
- For Reviewers
- Instructions for reviewers
- How to become a reviewer
- Best reviewers
- For Readers
- Readership
- Subscription
- Permission guidelines
- About
- Editorial policy
Articles
- Page Path
- HOME > Diabetes Metab J > Volume 35(1); 2011 > Article
-
Original ArticleBasal C-peptide Level as a Surrogate Marker of Subclinical Atherosclerosis in Type 2 Diabetic Patients
- Sung-Tae Kim1, Byung-Joon Kim1,2, Dong-Mee Lim1,2, In-Geol Song1, Jang-Han Jung1, Kang-Woo Lee1,2, Keun-Young Park1,2, Youn-Zoo Cho1, Dae-Ho Lee3, Gwan-Pyo Koh3
-
Diabetes & Metabolism Journal 2011;35(1):41-49.
DOI: https://doi.org/10.4093/dmj.2011.35.1.41
Published online: February 28, 2011
1Department of Internal Medicine, Konyang University Hospital, Konyang University School of Medicine, Daejon, Korea.
2Konyang University Myunggok Medical Research Institute, Daejon, Korea.
3Department of Internal Medicine, Jeju National University Hospital, Jeju National University School of Medicine, Jeju, Korea.
- Corresponding author: Dong Mee Lim. Division of Endocrinology and Metabolism, Department of Internal Medicine, Konyang University School of Medicine, 685 Gasuwon-dong, Seo-gu, Daejeon 302-718, Korea. mdldm@hanmail.net
Copyright © 2011 Korean Diabetes Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Background
- Recent studies have revealed that C-peptide induces smooth muscle cell proliferation and causes human atherosclerotic lesions in diabetic patients. The present study was designed to examine whether the basal C-peptide levels correlate with cardiovascular risk in type 2 diabetes mellitus (T2DM) patients.
-
Methods
- Data was obtained from 467 patients with T2DM from two institutions who were followed for four years. The medical findings of all patients were reviewed, and patients with creatinine >1.4 mg/dL, any inflammation or infection, hepatitis, or type 1 DM were excluded. The relationships between basal C-peptide and other clinical values were statistically analyzed.
-
Results
- A simple correlation was found between basal C-peptide and components of metabolic syndrome (MS). Statistically basal C-peptide levels were significantly higher than the three different MS criteria used in the present study, the Adult Treatment Panel III (ATP III) of the National Cholesterol Education Program's (NCEP's), World Health Organization (WHO), and the International Diabetes Federation (IDF) criteria (NCEP-ATP III, P=0.001; IDF, P<0.001; WHO, P=0.029). The multiple regression analysis between intima-media thickness (IMT) and clinical values showed that basal C-peptide significantly correlated with IMT (P=0.043), while the analysis between the 10-year coronary heart disease risk by the United Kingdom Prospective Diabetes Study risk engine and clinical values showed that basal C-peptide did not correlate with IMT (P=0.226).
-
Conclusion
- Basal C-peptide is related to cardiovascular predictors (IMT) of T2DM, suggesting that basal C-peptide does provide a further indication of cardiovascular disease.
- Diabetic subjects show a remarkable increase in cardiovascular complications, including myocardial infarctions and strokes, which are responsible for the majority of morbidity and mortality [1]. Many individual biomarkers, such as fibrinogen, C-reactive protein, uric acid, intima-media thickness (IMT) of the carotid artery, Framingham Risk Score (FRS), and the United Kingdom Prospective Diabetes Study (UKPDS) risk engine have been used as predictors of cardiovascular disease in diabetic patients. However, the predictive values of biomarkers have not been thoroughly studied [2].
- Type 2 diabetes mellitus (T2DM) is a heterogeneous group of disorders characterized by variable degrees of insulin resistance, impaired insulin secretion, and increased glucose production [3]. The increases in cardiovascular morbidity and mortality appear to relate to the synergism of degree of insulin resistance and hyperglycemia, even pre-diabetes [4]. Insulin resistance, as reflected by elevated serum insulin level, is associated with an increased risk of cardiovascular complications in individuals with and without DM. Serum C-peptide is not as well extracted by the liver and, due to the linearity of its kinetics, reflects the true pancreatic secretion of insulin [5,6].
- The currently available information establishes that C-peptide is not as biologically inert as previously believed. Instead, C-peptide is emerging as an active peptide hormone with potentially important physiological effects. In recent studies, the foregoing considerations have dealt primarily with the macrovascular complications of diabetes, with elevated levels of C-peptide being the main focus [7]. However, this concept remains controversial and few studies have reported the relationship between serum C-peptide and chronic complications of diabetes. Therefore, the authors of the present study hypothesized that basal C-peptide levels can be used as a cardiovascular predictor in T2DM patients.
- The present study was designed to examine whether the basal C-peptide level correlates with cardiovascular risk in T2DM patients via comparison with IMT, the 10-year coronary heart disease (CHD) risk by UKPDS engine and the metabolic syndrome (MS) components.
INTRODUCTION
- Study population
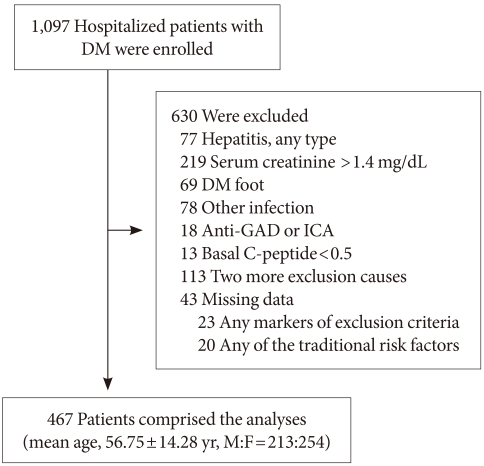
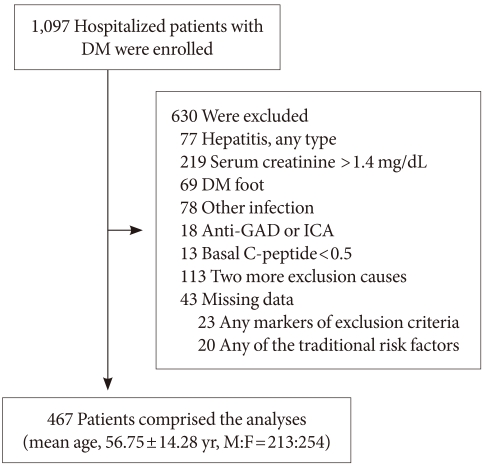
- From October 2005 to June 2009, data was obtained from 1,097 patients with DM who were hospitalized due to various reasons in two university hospitals in Chungcheongnam Province and Jeju Island, Republic of Korea (Fig. 1).
- Among the 1,097 participants, 630 with serum creatinine >1.4 mg/dL, DM foot, any inflammatory and infection diseases (urinary tract infection, upper respiratory infection), hepatitis or type 1 DM (basal C-peptide<0.5, elevated serum ketone level, and autoimmune islet antibody positive) were excluded. In addition, 23 participants with missing data for markers of the exclusion criteria and 20 participants with missing data for the traditional risk factors were excluded. The final sample for the analyses was comprised of 467 participants with T2DM (mean age, 56.75±14.28 years; M:F=213:254).
- Data collection and assays
- All subjects underwent a clinical examination. Blood samples from patients for all biochemical evaluations were collected after an overnight fast. Concentrations of lipids, glucose, blood urea nitrogen, creatinine, uric acid, homocysteine, fibrinogen and routine chemical markers were measured using the standard laboratory techniques.
- Glucose, total cholesterol (TC), triglyceride (TG), high density lipoprotein (HDL), and low density lipoprotein (LDL) cholesterol were measured using enzymatic methods (AU 5400; Olympus, Melville, NY, USA). Serum C-peptide levels were assessed using radioimmunoassay (SR 300; STRATEC, Birkenfeld, Germany). The intra-assay coefficient of variation (CV) was 1.78% and the inter-assay CV was 9.25%. The two institutes had the same models of laboratory instruments with the same CV values.
- Waist circumference (at the midpoint between the anterior superior iliac crest and the lowest rib) was obtained by trained researchers using standard techniques. The body mass index (BMI) was calculated as weight in kilograms divided by height in meters squared. Blood pressure was recorded in duplicate after 5 minutes of rest using random-zero sphygmomanometers.
- The 10-year CHD risk according to the UKPDS risk engine and IMT of the left carotid artery
- The 10-year CHD (non-fatal and fatal CHD) risk was calculated for each patient using the UKPDS risk engine (version 2.0 for Windows, University of Oxford, Oxford, UK) with admission demographics and fasting lipid profiles. The risk predictors used were age, duration of diabetes, gender, atrial fibrillation, ethnicity, smoking status, glycated hemoglobin (HbA1c), systolic blood pressure (SBP), TC, and HDL.
- The IMT of the left carotid artery was measured by an expert radiologist on the far wall of the distal common carotid artery using a 12 MHz linear probe. Carotid ultrasound, followed by a duplex color Doppler examination, was performed with a GE LogiQ9 (GE Healthcare, Milwaukee, WI, USA) and a linear probe of 7.5 to 12 MHz while the patient was in a supine position. Both left and right common carotid arteries were analyzed. Multiple measurements of the distal wall from anterior, lateral, and posterior longitudinal projections were recorded. Maximal IMT was measured in two segments of 1 cm each, from the flow divider caudally (carotid bulb) and from the beginning of the common carotid bulb (common carotid). The IMT value was calculated as an arithmetical mean from the bulb and common carotid segments of both sides. The IMT measurement was performed in hospitalized patients in Chungcheongnam province.
- Definition of MS
- Metabolic syndrome was defined according to criteria of the Adult Treatment Panel III (ATP III) of the National Cholesterol Education Program (NCEP's), World Health Organization (WHO), and the International Diabetes Federation (IDF).
- The WHO criteria [8] for MS required the presence of DM or impaired fasting plasma glucose (FPG ≥110 mg/dL) and at least two of the following components: 1) diagnosed with hypertension or blood pressure ≥140/90 mm Hg; 2) dyslipidemia: TG ≥150 mg/dL or HDL ≤40 mg/dL (male), ≤50 mg/dL (female); 3) central obesity: waist-hip ratio >0.90 (male); >0.85 (female), or BMI ≥30 kg/m2; or 4) microalbuminuria: urinary albumin to creatinine ratio ≥30 mg/g. The modified ATP III definition of MS [9] required the presence of at least three or more of the following five components: 1) elevated waist circumference ≥90 cm (male), ≥80 cm (female); 2) elevated TG >150 mg/dL (1.695 mmol/L); 3) reduced HDL<40 mg/dL (male), <50 mg/dL (female); 4) hypertension or elevated blood pressure ≥130/85 mm Hg; or 5) diabetes or elevated FPG ≥5.6 mmol/L. The 2006 IDF definition classified a person with MS in the same way as did ATP III but required the presence of central adiposity (elevated waist circumference) as an essential component [10].
- Statistical analysis
- A statistical analysis was performed with the PASW statistics, version 18.0 for Windows (SPSS Inc., Chicago, IL, USA). The differences between continuous variables between groups were compared using ANOVA and the independent t-test. Pearson's product-moment correlation was used for analysis between the basal C-peptide level and MS components. Multiple regression analysis was used for analysis of the relationship among the IMT, 10-year CHD risk by the UKPDS risk engine, and clinical variables. Differences were considered statistically significant when P<0.05.
METHODS
- General and biochemical characteristics
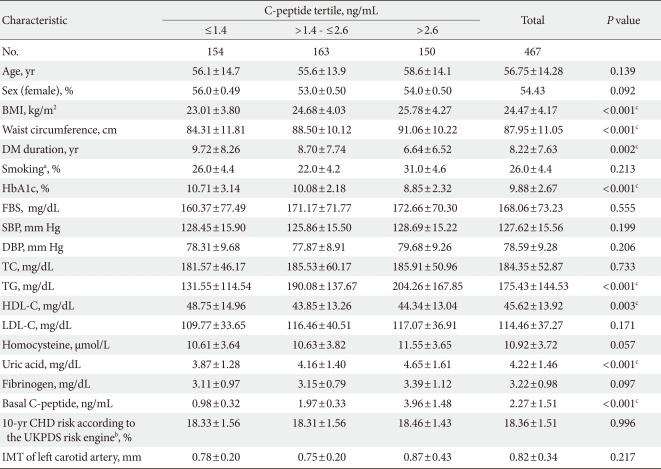
- General and biochemical characteristics of the 467 study subjects (213 men, 254 women) are presented in Table 1. The mean age of the subjects was 56.75±14.28 years, and the age range was 16-92 years. A total of 413 (67%) subjects from the base population of 467 were identified as having MS. The 10-year CHD risk according to the UKPDS risk engine was 18.36±1.51%, and IMT of the left carotid artery was 0.82±0.34 mm.
- The mean patient BMI was 24.47±4.17 kg/m2, and overweight but not obese subjects were also included. The mean DM duration was 8.22±7.63 years, and the mean value was 9.88±2.67%.
- Clinical characteristics of T2DM patients according to C-peptide tertile
- Basal C-peptide measured on an empty stomach was 2.27±1.51 ng/mL. Several clinical parameters were significantly different across the C-peptide tertiles, including BMI, waist circumference, DM duration, and levels of HbA1c, TG, HDL, and uric acid. However, the 10-year CHD risk according to the UKPDS and IMT of the left carotid artery were not significantly different by group (Table 1).
- Correlations between basal C-peptide level and cardiovascular biomarkers
- To date, there is no confirmed method to predict specific cardiovascular events. Accordingly, several markers of inflammation have been used as predictors of cardiovascular disease, resulting in dependence on indirect estimations such as cholesterol level, blood pressure, and waist circumference. Recently, IMT and the UKPDS risk engine have been the focus of many studies; therefore, the authors of the present study attempted to draw a comparison between cardiovascular risk and above-mentioned components.
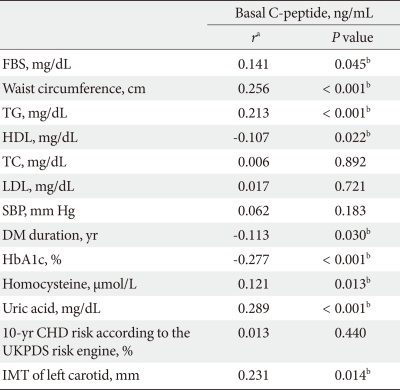
- Correlations were found between basal C-peptide level and the clinical components. Simple positive correlations were found with FPG, waist circumference, TG, and homocysteine, and simple negative correlations were observed for HDL, DM duration, and HbA1c. All values were statistically significant except for TC, LDL, and SBP, known predictors of cardiovascular disease (TC, P=0.892; LDL, P=0.721; SBP, P=0.183). IMT is known as a good correlation of macrovascular complications and also for having a positive correlation with C-peptide (P=0.014) (Table 2).
- Basal C-peptide level according to the presence of MS under three different definitions
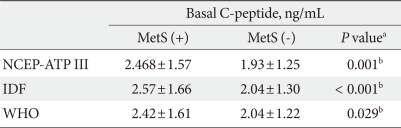
- Previous results suggested that C-peptide was more correlated with MS components such as fasting glucose, TG, waist circumference, and HDL than it was with SBP, TC, and LDL. Hence, the authors determined whether the basal C-peptide level had statistically significant relationships with the three MS criteria (NCEP-ATP III, IDF, WHO) using the independent t-test. Basal C-peptide levels tended to increase according to the presence of MS (NCEP-ATP III, P=0.001; IDF, P<0.001; WHO, P=0.029) (Table 3).
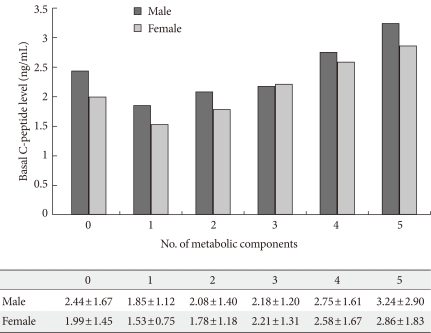
- The trend of basal C-peptide level according to the number of metabolic components
- Basal C-peptide level increased with the number of metabolic components according to the NCEP-ATP III criteria, and the increments were statistically significant (P<0.001) (Fig. 2).
- Multiple regression analysis with IMT and the 10-year CHD risk according to the UKPDS risk engine using clinical variables
- The factors which influence the IMT and FRS and which are known to be established predictors of macrovascluar complications were investigated.
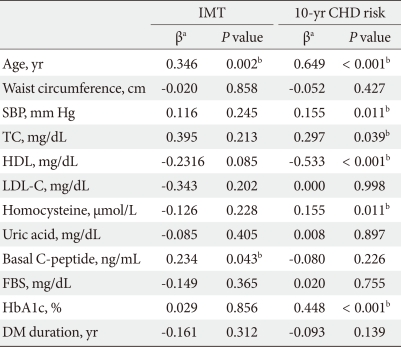
- The multiple regression analysis between IMT and the clinical values showed that basal C-peptide level had an independent positive correlation (b=0.234) with IMT that was statistically significant (P=0.043). The basal C-peptide level did not correlate with the 10-year CHD risk according to the UKPDS risk engine (P=0.226) (Table 4).
RESULTS
- C-peptide, formed during cleavage of insulin from proinsulin, is a by-product of insulin biosynthesis. After the discovery of the mode of insulin biosynthesis, several early studies addressed the question of possible physiological effects of C-peptide. However, because C-peptide has not been hormonally demonstrated, this proinsulin-connecting peptide has been regarded as a biologically inert by-product [11]. Recently, the G protein-coupled receptor with subsequent activation of the Ca2+-dependent intracellular signaling pathways and the specific binding of the C-peptide to human cell membranes have been demonstrated [12]. C-peptide effects have been suggested to act upon biologically active peptides [13]. According to recent studies, C-peptide induces smooth muscle cell (SMC) proliferation, immune response, cell growth and may play a pivotal role in the regulation of endothelial function. Previous studies have suggested that such mechanisms could facilitate cardiovascular events [14,15]. Until now, there have been few studies regarding C-peptide and diabetes complications. The authors of the present study aimed to determine whether the basal C-peptide levels were related to cardiovascular risk in T2DM patients.
- The present study was designed to evaluate the correlations between C-peptide levels and clinical values of known cardiovascular risk factors such as uric acid, homocystein, SBP, TC, LDL-C, TG, HDL-C, waist circumference, CHD risk according to the UKPDS risk engine and IMT. In Table 2, C-peptide had simple correlations with uric acid, homocystein, TG, HDL-C, and waist circumference, all of which are components of MS. However, the C-peptide level did not significantly correlate with TC, LDL-C, or SBP. Cho et al. [16] showed very similar results. Significant differences were observed in fasting serum C-peptide levels between the abdominal obesity group and the other groups of T2DM patients (diagnosed for over 10 years) (1.80±1.87 µg/L vs. 1.45±1.02 µg/L). Furthermore, C-peptide was also correlated with fibrinogen, TG, HDL-C, and waist circumference.
- Basal C-peptide level has a strong association with insulin resistance. Thus, the direct correlations between C-peptide and three different MS definitions (NCEP-ATP III, WHO, IDF) were verified. In Table 3 and Fig. 2, the basal C-peptide level was increased significantly in the MS group with diabetes. Fasting insulin levels are a crude index of insulin secretion and insulin resistance and may underestimate the magnitudes of the associations between insulin resistance and components of MS [17]. C-peptide appeared to correlate better to the well-known variables of MS than it did to insulin, possibly suggesting that C-peptide is a better surrogate than insulin for estimating insulin resistance in epidemiological studies [18].
- According to the results from the Multiple Risk Factor Intervention Trial (MRFIT) [19], the Veteran Affairs High Density Lipoprotein Intervention Trial (VA-HIT) [20] and the Insulin Resistance Atherosclerosis Study (IRAS) [21], hyperinsulinemia and insulin resistance are supported by showing a direct relationship between insulin level and cardiovascular risk [22]. However, the molecular mechanisms underlying the association between insulin resistance and atherosclerosis are still unclear. Hyperglycemia, advanced glycation end products, and dyslipidemia also have been suggested to create vascular events. Although hyperglycemia has been demonstrated to stimulate SMC proliferation in vitro and is thought to contribute to neointima formation, recent reports challenge the concept by demonstrating no mitogenic activity in high glucose environments. Park et al. [23] showed that hyperglycemia in streptozotocin-induced diabetic rats was not associated with increased neointima formation.
- The Diabetes Control and Complications Trial (DCCT) [24] and the UKPDS [25] have provided consistent evidence that intensive glycemic control prevents the development and progression of microvascular complications in patients with types 1 or 2 diabetes. However, whether intensive glucose reduction also prevents macrovascular disease and major cardiovascular events remains unclear. Therefore, hyperglycemia is not thought to be the main mechanism of cardiovascular complications in T2DM.
- Marx and colleagues [26] demonstrated co-localization of C-peptide with SMC in early human atherosclerotic lesions of diabetic subjects. In vitro stimulation of SMC with C-peptide via insulin resistance and compensatory hyperinsulinemia resulted in a dose-dependent induction of smooth cell proliferation. The study outlined a previously unrecognized role for C-peptide to act as mitogen for SMC. Wang et al. [27] proposed that the presence of metabolic insulin resistance (i.e., diminished strength of the PI 3-kinase signaling) and the resulting compensatory hyperinsulinemia cause SMC proliferation, which results in a selective impairment of the PI 3-kinase pathway with intact signaling along the ERK1/2-MAPK pathway, rather than a role in conveying the metabolic action. Currently, insulin acts as a weak mitogen which is not sufficient to influence the proliferation effect. In other words, C-peptide, in conditions which lead to insulin resistance, increases compensatory pathways as well as induces several other signaling pathways including the ERK1/2-MAPK and PI 3-kinase pathways through Src kinase. C-peptide may also have proathergenic effects, such as stimulation of monocytes and T-cell chemotaxis, in atherosclerotic lesions from diabetic patients [28].
- IMT is a good marker of early atherosclerotic changes and its progression. IMT is increased in groups of patients with several cardiovascular risk factors [29]. The authors of the present study attempted to determine the independent factors of commonly used methods and markers. In Table 4, C-peptide is an independent factor for IMT but not for the 10-year CHD risk according to the UKPDS risk engine.
- The 10-year CHD risk according to the UKPDS risk engine was calculated for each patient based on smoking status, total serum cholesterol, age, serum LDL-C, and SBP. In the present study, Table 2 also shows that basal C-peptide was not associated with the UKPDS risk engine-related factors. Basal C-peptide was not considered to be an independent factor that influences the 10-year CHD risk. However, IMT can be directly assessed based on arterial vessel wall changes and SMC proliferation. As mentioned above, insulin resistance and C-peptide are associated with SMC proliferation. Thus, C-peptide was thought to be an independent factor for IMT, as shown in Table 4. In the Atherosclerosis Risk in the Communities (ARIC) study [30], higher levels of endogenous insulin were significantly associated with increased thickness of the carotid artery wall.
- The Wisconsin Epidemiologic Study of Diabetic Retinopathy (WESDR) [31] is an ongoing prospective, population-based cohort study analyzing the relationships of exogenous insulin and C-peptide level with ischemic heart disease mortality over a 16-year period. In the WESDR study, higher levels of plasma C-peptide were also associated with increased risks of death.
- The present study has several limitations. First, the study was based on a cross-sectional design, thus the nature of the investigation and the results do not imply a general case, and longitudinal studies are needed. Second, most of the subjects had uncontrolled blood sugar, which may be a risk factor of cardiovascular disease. Third, a correlation between insulin resistance and C-peptide was not considered when using HOMA-IR in the present study. Fourth, basal C-peptide level may have been influenced by various medications because the study population consisted of newly diagnosed, treated or untreated diabetes patients.
- In conclusion, the present study suggests that basal C-peptide level in T2DM is related to MS in that it may be a surrogate marker of subclinical atherosclerosis. Further large prospective studies are needed to examine the hypothesis of C-peptide's proatherogenic effects. Moreover, additional work is necessary to identify the C-peptide receptor.
DISCUSSION
- 1. Haffner SM, Lehto S, Ronnemaa T, Pyorala K, Laakso M. Mortality from coronary heart disease in subjects with type 2 diabetes and in nondiabetic subjects with and without prior myo cardial infarction. N Engl J Med 1998;339:229-234. ArticlePubMed
- 2. Ridker PM, Brown NJ, Vaughan DE, Harrison DG, Mehta JL. Established and emerging plasma biomarkers in the prediction of first atherothrombotic events. Circulation 2004;109(25 Suppl 1):IV6-IV19. ArticlePubMed
- 3. Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 2003;26(Suppl 1):S5-S20. ArticlePubMedPDF
- 4. Air EL, Kissela BM. Diabetes, the metabolic syndrome, and ischemic stroke: epidemiology and possible mechanisms. Diabetes Care 2007;30:3131-3140. PubMed
- 5. Clark PM, Hales CN. How to measure plasma insulin. Diabetes Metab Rev 1994;10:79-90. ArticlePubMed
- 6. O'Rahilly S, Burnett MA, Smith RF, Darley JH, Turner RC. Haemolysis affects insulin but not C-peptide immunoassay. Diabetologia 1987;30:394-396. ArticlePubMedPDF
- 7. Haban P, Simoncic R, Zidekova E, Ozdin L. Role of fasting serum C-peptide as a predictor of cardiovascular risk associated with the metabolic X-syndrome. Med Sci Monit 2002;8:CR175-CR179. PubMed
- 8. Alberti KG, Zimmet PZ. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabet Med 1998;15:539-553. ArticlePubMed
- 9. Denke MA, Pasternak RC. Defining and treating the metabolic syndrome: a primer from the Adult Treatment Panel III. Curr Treat Options Cardiovasc Med 2001;3:251-253. ArticlePubMedPDF
- 10. Alberti KG, Zimmet P, Shaw J. IDF Epidemiology Task Force Consensus Group. The metabolic syndrome--a new worldwide definition. Lancet 2005;366:1059-1062. PubMed
- 11. Kitabchi AE. Proinsulin and C-peptide: a review. Metabolism 1977;26:547-587. ArticlePubMed
- 12. Rigler R, Pramanik A, Jonasson P, Kratz G, Jansson OT, Nygren P, Stahl S, Ekberg K, Johansson B, Uhlen S, Uhlen M, Jornvall H, Wahren J. Specific binding of proinsulin C-peptide to human cell membranes. Proc Natl Acad Sci U S A 1999;96:13318-13323. ArticlePubMedPMC
- 13. Johansson J, Ekberg K, Shafqat J, Henriksson M, Chibalin A, Wahren J, Jornvall H. Molecular effects of proinsulin C-peptide. Biochem Biophys Res Commun 2002;295:1035-1040. ArticlePubMed
- 14. Nordquist L, Johansson M. Proinsulin C-peptide: friend or foe in the development of diabetes-associated complications? Vasc Health Risk Manag 2008;4:1283-1288. ArticlePubMedPMCPDF
- 15. Schlessinger J. New roles for Src kinases in control of cell survival and angiogenesis. Cell 2000;100:293-296. ArticlePubMed
- 16. Cho M, Park JS, Nam J, Kim CS, Nam JH, Kim HJ, Ahn CW, Cha BS, Lim SK, Kim KR, Lee HC, Huh KB. Association of abdominal obesity with atherosclerosis in type 2 diabetes mellitus (T2DM) in Korea. J Korean Med Sci 2008;23:781-788. ArticlePubMedPMC
- 17. Manolio TA, Savage PJ, Burke GL, Liu KA, Wagenknecht LE, Sidney S, Jacobs DR Jr, Roseman JM, Donahue RP, Oberman A. Association of fasting insulin with blood pressure and lipids in young adults. The CARDIA study. Arteriosclerosis 1990;10:430-436. ArticlePubMed
- 18. Chen CH, Tsai ST, Chou P. Correlation of fasting serum C-peptide and insulin with markers of metabolic syndrome-X in a homogenous Chinese population with normal glucose tolerance. Int J Cardiol 1999;68:179-186. PubMed
- 19. Orchard TJ, Eichner J, Kuller LH, Becker DJ, McCallum LM, Grandits GA. Insulin as a predictor of coronary heart disease: interaction with apolipoprotein E phenotype. A report from the Multiple Risk Factor Intervention Trial. Ann Epidemiol 1994;4:40-45. ArticlePubMed
- 20. Rubins HB, Robins SJ, Collins D, Fye CL, Anderson JW, Elam MB, Faas FH, Linares E, Schaefer EJ, Schectman G, Wilt TJ, Wittes J. Veterans Affairs High-Density Lipoprotein Cholesterol Intervention Trial Study Group. Gemfibrozil for the secondary prevention of coronary heart disease in men with low levels of high-density lipoprotein cholesterol. N Engl J Med 1999;341:410-418. ArticlePubMed
- 21. Howard G, O'Leary DH, Zaccaro D, Haffner S, Rewers M, Hamman R, Selby JV, Saad MF, Savage P, Bergman R. Insulin sensitivity and atherosclerosis. The Insulin Resistance Atherosclerosis Study (IRAS) Investigators. Circulation 1996;93:1809-1817. ArticlePubMed
- 22. Semenkovich CF. Insulin resistance and atherosclerosis. J Clin Invest 2006;116:1813-1822. ArticlePubMedPMC
- 23. Park SH, Marso SP, Zhou Z, Foroudi F, Topol EJ, Lincoff AM. Neointimal hyperplasia after arterial injury is increased in a rat model of non-insulin-dependent diabetes mellitus. Circulation 2001;104:815-819. ArticlePubMed
- 24. The Diabetes Control and Complications Trial Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med 1993;329:977-986. ArticlePubMed
- 25. UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet 1998;352:837-853. ArticlePubMed
- 26. Marx N, Walcher D, Raichle C, Aleksic M, Bach H, Grub M, Hombach V, Libby P, Zieske A, Homma S, Strong J. C-peptide colocalizes with macrophages in early arteriosclerotic lesions of diabetic subjects and induces monocyte chemotaxis in vitro. Arterioscler Thromb Vasc Biol 2004;24:540-545. ArticlePubMed
- 27. Wang CC, Goalstone ML, Draznin B. Molecular mechanisms of insulin resistance that impact cardiovascular biology. Diabetes 2004;53:2735-2740. ArticlePubMedPDF
- 28. Bruemmer D. C-Peptide in insulin resistance and vascular complications: teaching an old dog new tricks. Circ Res 2006;99:1149-1151. PubMedPMC
- 29. Lonn E. Carotid artery intima-media thickness: a new noninvasive gold standard for assessing the anatomic extent of atherosclerosis and cardiovascular risk? Clin Invest Med 1999;22:158-160. PubMed
- 30. Folsom AR, Eckfeldt JH, Weitzman S, Ma J, Chambless LE, Barnes RW, Cram KB, Hutchinson RG. Relation of carotid artery wall thickness to diabetes mellitus, fasting glucose and insulin, body size, and physical activity. Atherosclerosis Risk in Communities (ARIC) Study Investigators. Stroke 1994;25:66-73. ArticlePubMed
- 31. Hirai FE, Moss SE, Klein BE, Klein R. Relationship of glycemic control, exogenous insulin, and C-peptide levels to ischemic heart disease mortality over a 16-year period in people with older-onset diabetes: the Wisconsin Epidemiologic Study of Diabetic Retinopathy (WESDR). Diabetes Care 2008;31:493-497. PubMed
REFERENCES

Values are presented as mean±standard deviation or number (%).
P value was analyzed using ANOVA.
T2DM, type 2 diabetes mellitus; BMI, body mass index; HbA1c, glycated hemoglobin; FBS, fasting blood sugar; SBP, systolic blood pressure; DBP, diastolic blood pressure; TC, total cholesterol; TG, triglyceride; HDL-C, high density lipoprotein cholesterol; LDL-C, low density lipoprotein cholesterol; CHD, coronary heart disease; UKPDS, United Kingdom Prospective Diabetes Study; IMT, intima-media thickness.
aThis value means the percentage of ex- and current-smokers, bValues were non-fatal and fatal CHD risk calculated according to the UKPDS risk engine, cP values<0.05.
FBS, fasting blood sugar; TG, triglyceride; HDL, high density lipoprotein; TC, total cholesterol; LDL, low density lipoprotein; SBP, systolic blood pressure; DM, diabetes mellitus; CHD, coronary heart disease; UKPDS, United Kingdom Prospective Diabetes Study; IMT, intima-media thickness.
aPearson's product-moment correlation coefficient, bP values<0.05.
Values are presented as mean±standard deviation.
NCEP, National Cholesterol Education Program; ATP III, Adult Treatment Panel III; IDF, International Diabetes Federation; WHO, World Health Organization.
aP between subjects with and without metabolic syndrome using independent t-test, bP values<0.05.
IMT, intima-media thickness; CHD, coronary heart disease; UKPDS, United Kingdom Prospective Diabetes Study; SBP, systolic blood pressure; TC, total cholesterol; HDL, high density lipoprotein; LDL-C, low density lipoprotein cholesterol; FBS, fasting blood sugar; DM, diabetes mellitus.
aRegression coefficient, bP values<0.05.
Figure & Data
References
Citations
- The Correlation Between C-Peptide and Severity of Peripheral Atherosclerosis in Type 2 Diabetes Mellitus
Maisa A Wahab, Alshaymaa Alhabibi, Ahmed Khairy Sakr, Mohamed Yahia Zakaria, Ola I Saleh, Inass Hassan Ahmad, Eman Abdelrahman, Randa Taha, Fayka Karem Abdel Azeem Ahmed, Bothayna Ismail, Lamiaa Hosney Azel, Asmaa S Hassan, Hanaa Mohammed Eid El Sayed, Sa
Diabetes, Metabolic Syndrome and Obesity.2023; Volume 16: 2617. CrossRef - Blood C‐peptide concentration as a proxy marker of cardiovascular disease: An observational cross‐sectional study
Laurinda Adusu‐Donkor, Emmanuel Kwaku Ofori, Fleischer C. N. Kotey, Francis Kwaku Dogodzi, Wormenor Dziedzorm, Alfred Buabeng, Segla Kwame Bernard, Seth K. Amponsah, Henry Asare‐Anane
Health Science Reports.2023;[Epub] CrossRef - The impact of insulin induced lipohypertrophy on carotid intima-media thickness in patients with type 2 diabetes mellitus
Cem Onur Kirac, Vehbi Sirikci, Huseyin Avni Findikli
Medicine.2023; 102(39): e34696. CrossRef - Effects of Serum C-Peptide Level on Blood Lipid and Cardiovascular and Cerebrovascular Injury in Patients with Type 2 Diabetes Mellitus: A Meta-Analysis
Juan Qin, Rongli Sun, Ding Ding, Yuvaraja Teekaraman
Contrast Media & Molecular Imaging.2022; 2022: 1. CrossRef - Correlation between serum C-peptide-releasing effects and the risk of elevated uric acid in type 2 diabetes mellitus
Yanyan Liu, Xue Zhao, Zequn Yang, Shurui Wang, Cong Han, Huijuan Zhang
Endocrine Journal.2022; 69(7): 773. CrossRef - Human C-peptide is a ligand of the elastin-receptor-complex and therewith central to human vascular remodelling and disease in metabolic syndrome
Gert Wensvoort
Medical Hypotheses.2022; 168: 110964. CrossRef - Influence of blood glucose fluctuation, C-peptide level and conventional risk factors on carotid artery intima–media thickness in Chinese Han patients with type 2 diabetes mellitus
Min Liu, Li Ao, Xinyu Hu, Jianning Ma, Kena Bao, Ye Gu, Jing Zhao, Weiping Huang
European Journal of Medical Research.2019;[Epub] CrossRef - Serum C peptide and carotid intima-medial thickness are independent markers of glucose intolerance among patients with ischemic cerebrovascular stroke
Nearmeen M. Rashad, Ghada M. Samir, Hanan M. Sabry, Nesreen M. Mohy, Shereen M. El Shabrawy
The Egyptian Journal of Internal Medicine.2019; 31(3): 368. CrossRef - Biomarker potential of C-peptide for screening of insulin resistance in diabetic and non-diabetic individuals
Haseeb A. Khan, Samia H. Sobki, Aishah Ekhzaimy, Isra Khan, Mona A. Almusawi
Saudi Journal of Biological Sciences.2018; 25(8): 1729. CrossRef - SERUM C-PEPTIDE LEVEL IN OBESE AND NON-OBESE PATIENTS WITH TYPE 2 DIABETES MELLITUS
Shamha Beegum Mariyam, Saboora Beegum Muthubeevi, Sandhya Chandrasekharan Vasantha
Journal of Evolution of Medical and Dental Sciences.2017; 6(05): 350. CrossRef - Mechanisms of action and therapeutic potential of proinsulin C-peptide
A. O. Shpakov
Journal of Evolutionary Biochemistry and Physiology.2017; 53(3): 180. CrossRef - Hemolysis Affects C‐Peptide Immunoassay
Zhi‐Qi Wu, Ju Lu, Hua‐Guo Xu
Journal of Clinical Laboratory Analysis.2016; 30(6): 1232. CrossRef - Lipid and inflammatory biomarker profiles in early insulin resistance
Itahisa Marcelino Rodríguez, José Oliva García, José Juan Alemán Sánchez, Delia Almeida González, Santiago Domínguez Coello, Buenaventura Brito Díaz, Fadoua Gannar, María del Cristo Rodríguez Pérez, Roberto Elosua, Antonio Cabrera de León
Acta Diabetologica.2016; 53(6): 905. CrossRef - C-Peptide Is Independently Associated with an Increased Risk of Coronary Artery Disease in T2DM Subjects: A Cross-Sectional Study
Lingshu Wang, Peng Lin, Aixia Ma, Huizhen Zheng, Kexin Wang, Wenjuan Li, Chuan Wang, Ruxing Zhao, Kai Liang, Fuqiang Liu, Xinguo Hou, Jun Song, Yiran Lu, Ping Zhu, Yu Sun, Li Chen, Marta Letizia Hribal
PLOS ONE.2015; 10(6): e0127112. CrossRef - C-peptide as a risk factor of coronary artery disease in the general population
Antonio Cabrera de León, José Gregorio Oliva García, Itahisa Marcelino Rodríguez, Delia Almeida González, José Juan Alemán Sánchez, Buenaventura Brito Díaz, Santiago Domínguez Coello, Vicente Bertomeu Martínez, Armando Aguirre Jaime, María del Cristo Rodr
Diabetes and Vascular Disease Research.2015; 12(3): 199. CrossRef - Gender differences in the association of insulin resistance and high-sensitivity c-reactive protein in obese adolescents
Ramin Alemzadeh, Jessica Kichler
Journal of Diabetes & Metabolic Disorders.2014;[Epub] CrossRef - Cytokinome Profile of Patients with Type 2 Diabetes and/or Chronic Hepatitis C Infection
Susan Costantini, Francesca Capone, Eliana Guerriero, Raffaele Marfella, Angela Sorice, Patrizia Maio, Michele Di Stasio, Giuseppe Paolisso, Giuseppe Castello, Giovanni Colonna, Patricia Fitzgerald-Bocarsly
PLoS ONE.2012; 7(6): e39486. CrossRef - Serum glycated albumin predicts the progression of carotid arterial atherosclerosis
Sun Ok Song, Kwang Joon Kim, Byung-Wan Lee, Eun Seok Kang, Bong Soo Cha, Hyun Chul Lee
Atherosclerosis.2012; 225(2): 450. CrossRef - C-Peptide: A New Mediator of Atherosclerosis in Diabetes
Dusica Vasic, Daniel Walcher
Mediators of Inflammation.2012; 2012: 1. CrossRef - Letter: Basal C-peptide Level as a Surrogate Marker of Subclinical Atherosclerosis in Type 2 Diabetes Patients (Diabetes Metab J 2011;35:41-9)
Min Suk Lee, Hae Jin Kim
Diabetes & Metabolism Journal.2011; 35(2): 188. CrossRef - Response: Basal C-peptide Level as a Surrogate Marker of Subclinical Atherosclerosis in Type 2 Diabetic Patients (Diabetes Metab J 2011;35:41-9)
Sung-Tae Kim, Byung-Joon Kim, Dong-Mee Lim, In-Geol Song, Jang-Han Jung, Kang-Woo Lee, Keun-Young Park, Youn-Zoo Cho, Dae-Ho Lee, Gwan-Pyo Koh
Diabetes & Metabolism Journal.2011; 35(2): 190. CrossRef
 PubReader
PubReader Cite
Cite