Prevalence, Awareness, and Management of Obesity in Korea: Data from the Korea National Health and Nutrition Examination Survey (1998-2011)
Article information
Abstract
Background
Obesity is a risk factor for diabetes and several cardiovascular diseases. This study was to investigate the trends in the prevalence, awareness, and management status of obesity among the Korean population for recent 13 years.
Methods
The prevalence, subjective awareness, and management of obesity were investigated in adults aged ≥19 years by using the data from the Korea National Health and Nutrition Examination Surveys (KNHANES) 1998 to 2011.
Results
The number of participants was 8,117, 5,826, 5,500, 3,025, 6,756, 7,506, 6,255, and 6,155 in the KNHANES in years 1998, 2001, 2005, 2007, 2008, 2009, 2010, and 2011, respectively. The prevalence of obesity was 26.9%, 29.2%, 32.9%, 32.5%, 32.0%, 32.6%, 32.0%, and 32.0% in 1998, 2001, 2005, 2007, 2008, 2009, 2010, and 2011, respectively, while the overall prevalence of obesity and abdominal obesity increased by 1.19-fold and 1.24-fold respectively in 2011 compared against 2001. In general, a gradual increase in the prevalence of severe obesity has been observed as years go by. Furthermore, trends of improvements in obesity awareness and management rates were visible over the period of surveys.
Conclusion
Although the management status of obesity has improved during the recent years, more effective strategy to control obesity is needed.
INTRODUCTION
Obesity is a chronic disease that is causally related to serious medical illnesses, whose worldwide prevalence has increased dramatically over the last several decades [1]. As a developing country, Korea is presently experiencing rapid economic, social, and cultural changes, including an accelerated pace of nutrition transition that may result in a greatly increased burden of chronic diseases, such as obesity [2]. The marked increase in the prevalence of obesity has become one of the major causes for the 25% increase in the prevalence of diabetes in the United States over the last 20 years [3].
The risk of diabetes increases linearly with body mass index (BMI) [3], as well as being correlated with abdominal obesity [4-6]. Obesity causes many serious medical complications that impair the quality of life and ultimately lead to increased morbidity and premature death [7,8]. Therefore, the assessment of the prevalence and management status of obesity that were conducted in recent years are crucial and would provide important information that could be useful for planning preventive strategy to reduce obesity-related complications.
Before 1995, there was no standardized epidemiological survey regarding the prevalence of obesity. However the Korea National Health and Nutrition Examination Survey (KNHANES) has been performed regularly from 1995 by the Ministry of Health and Welfare. Here, using these information to our advantage, we investigated the recent changes in the prevalence, subjective awareness, and management of obesity among Korean adults during 1998 to 2011 and discussed the changing trends.
METHODS
Study population and data collection
This study was based on the data acquired from the KNHANES I (1998), II (2001), III (2005), IV (2007 to 2009), and V (2010, 2011). The KNHANES is a nationwide and population-based cross-sectional health survey conducted by the Korean Ministry of Health and Welfare.
These surveys have been conducted periodically since 1998 for the assessment of the health and nutritional status of the Korean population, using a rolling sampling design, which involves a complex and stratified, multistage probability-cluster survey of a representative sample of a noninstitutionalized civilian population.
The KNHANES consisted of three distinct surveys: the health interview survey, the health examination survey, and the nutrition survey. The survey collected data via household interviews and by direct standardized physical examinations conducted in specially equipped mobile examination centers. Participants were selected from sampling units based on geographical area, sex, and age-groups using household registries with a stratified, multistage, clustered, and probability sampling design. The sample for each year was the probability sample representing all parts of the country, which was determined by assigning weights to each respondent, and each rolling sample had both homogenous and independent characteristics. The KNHANES was conducted according to the guidelines laid down in the Declaration of Helsinki. All subjects participated voluntarily and informed consent was obtained.
We analyzed subjects who were ≥19 years of age and completed both the health examination and health interview survey, excluding any measurements that were missing BMI or waist circumference.
Definition of each criterion
Obesity was diagnosed anthropometrically using the data from the health examination of each KNHANES. Height was measured using a portable stadiometer to the nearest 0.1 cm and weight was measured using a calibrated balance-beam scale to the nearest 0.1 kg, with which BMI was calculated and obesity was defined as BMI ≥25 kg/m2, according to the Korean Society for the Study of Obesity [9]. Moreover, waist circumference of ≥90 cm in men and ≥85 cm in women were used to define abdominal obesity according to the Korean Society for the Study of Obesity [10].
Next, we divided the participants into diabetic and nondiabetic subjects to compare the prevalence and management status of obesity between them. The diagnostic criteria for diabetes mellitus were obtained from the American Diabetes Association guidelines [11]. Subjects were diagnosed with diabetes if their fasting plasma glucose levels were over 126 mg/dL or if they responded to the health interview survey to have had been previously diagnosed with diabetes by a physician, or treated with antidiabetic agents or insulin.
Awareness and management of obesity were defined using the health interview survey and the health examination survey results from the KNHANES. Awareness of obesity was defined by participants whose responses to the health interview survey of KNHANES were little obese or very obese from the choice of: very skinny, little skinny, usual, little obese, and very obese. Moreover, answers to define the management of obesity were categorized to four items: tried to reduce weight, tried to maintain weight, trying to increase weight, or never tried to manage weight for 1 year.
Biochemical measurements
Blood was collected from the antecubital vein of each participant after fasting for at least 8 hours. The samples were properly processed, refrigerated at 2℃ to 8℃, and transported to the Central Testing institute in Seoul, Korea and the plasma was separated immediately by centrifugation. Blood samples were analyzed within 24 hours of transportation. Analysis of fasting glucose was performed with Hitachi Automatic Analyzer 7600 (Hitachi, Tokyo, Japan).
Statistical analyses
Sampling weights based on the sample design of each KNHANES were used to calculate the prevalence of obesity. For analyses, we used the KNHANES stratification variables and sampling weights designated by the Korean Centers for Disease Control and Prevention, which were based on the sample design of each different surveys. Nominal variables were presented as the number of cases and percentage. The PASW version 18.0 software (IBM Co., Armonk, NY, USA) was used for analyses. Every comparison among the studies was done after age adjustment.
RESULTS
Recent prevalence, awareness, and management of obesity (from the KNHANES 2011)
The prevalence of obesity and abdominal obesity in 2011 were 32.0% (male, 34.9%; female, 30.5%) and 27.7% (male, 28.1%; female, 27.5%), respectively. Moreover, in nondiabetic patients the prevalence of obesity and abdominal obesity were 30.8% (male, 34.6%; female, 28.7%) and 25.5% (male, 26.4%; female, 24.9%), respectively. In diabetic patients, abdominal obesity (50.4% [male, 42.1%; female, 58.8%]) was more common than general obesity (44.4% [male, 37.1%; female, 51.8%]), whose prevalence was roughly double of those of nondiabebic subjects.
The prevalence of obesity and abdominal obesity categorized by age in 2011 are shown in Table 1, from which a trend of increasing prevalence of obesity with older age was observable, reaching a peak in the 60 to 69 years age group in nondiabetic subjects. As for diabetic subjects, the prevalence of obesity and abdominal obesity peaked in the 40 to 49 year age group, which is much earlier than the nondiabetic subjects.
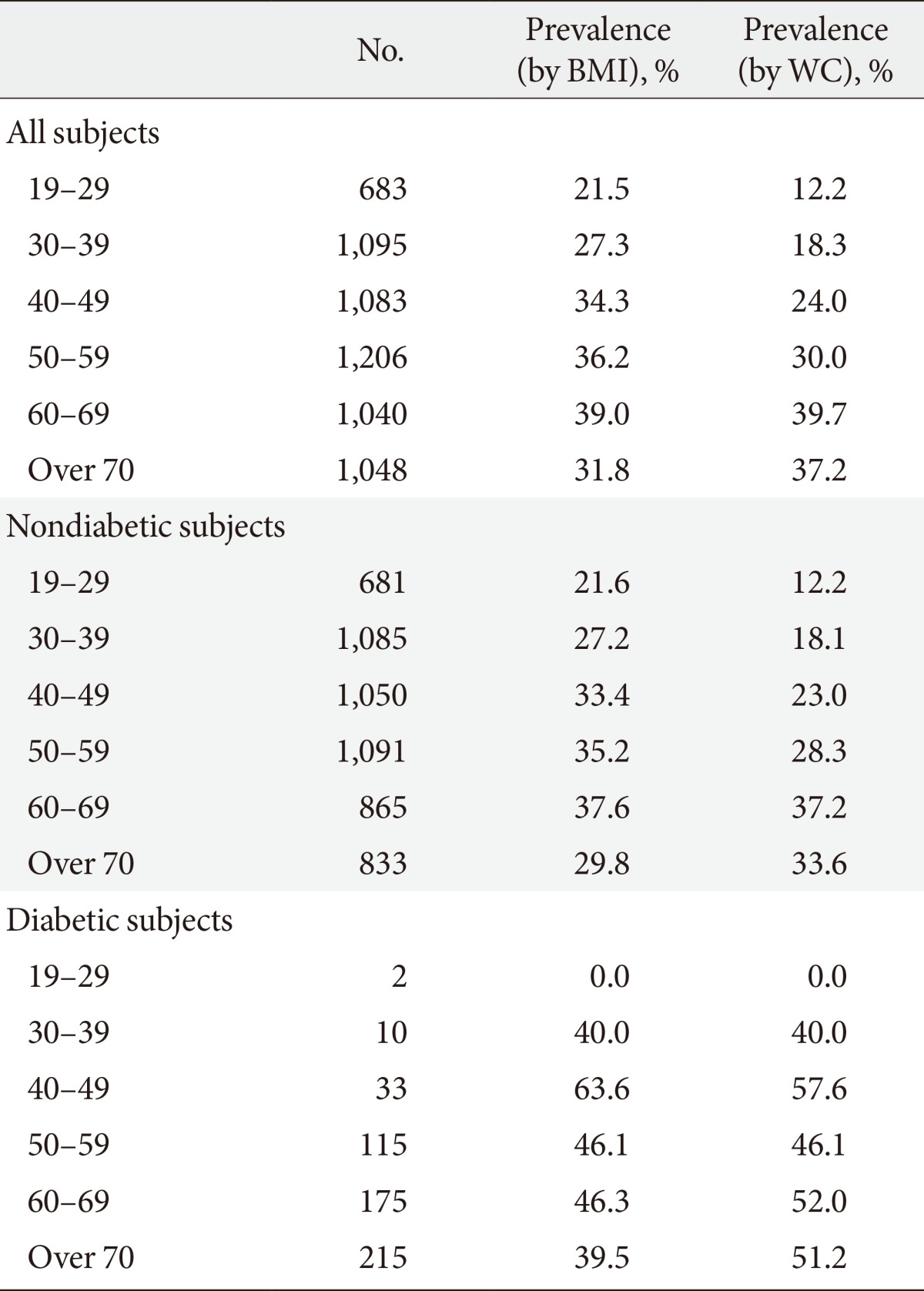
Prevalence of obesity and abdominal obesity by age-category in the Korea National Health and Nutrition Examination Survey in 2011
Subjective awareness and management for obesity are shown in Tables 2 and 3. Overall, the subjects who considered their body sizes to be normal were most common, followed by those who considered themselves to be a little obese. The group who thought their bodies were a little skinny was the smallest. Interestingly, the awareness for obesity was lower in diabetic subjects than nondiabetic subjects (38.4% vs. 41.2%) despite the prevalence of obesity being higher in diabetic subjects than nondiabetic subjects. More than half of the subjects tried to reduce or maintain their body weight. However the effort to reduce body weight in diabetic subjects was less than nondiabetic subject (33.1% vs. 39.5%), regardless of the higher prevalence of obesity.
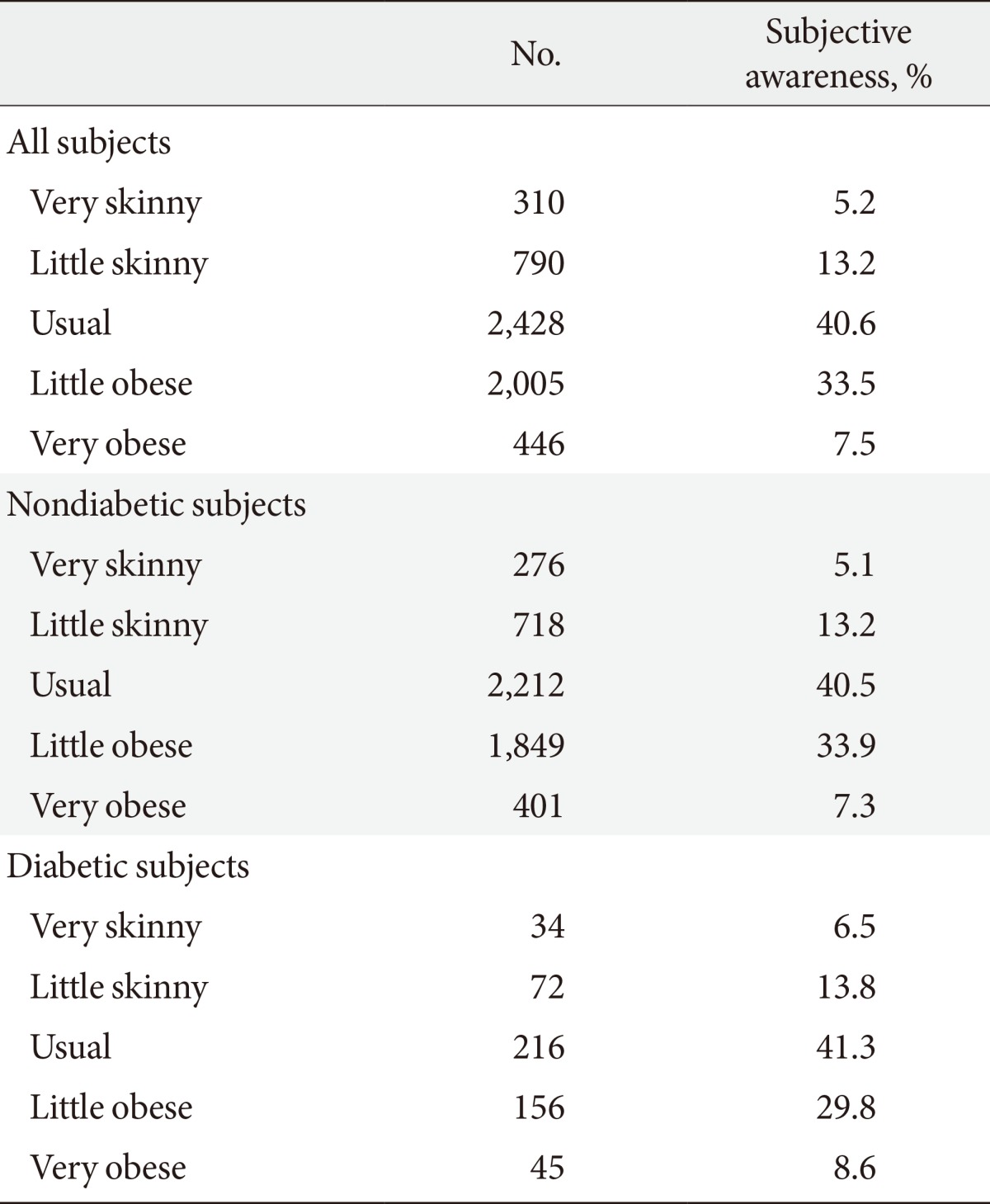
Subjective awareness for obesity in the Korea National Health and Nutrition Examination Survey in 2011
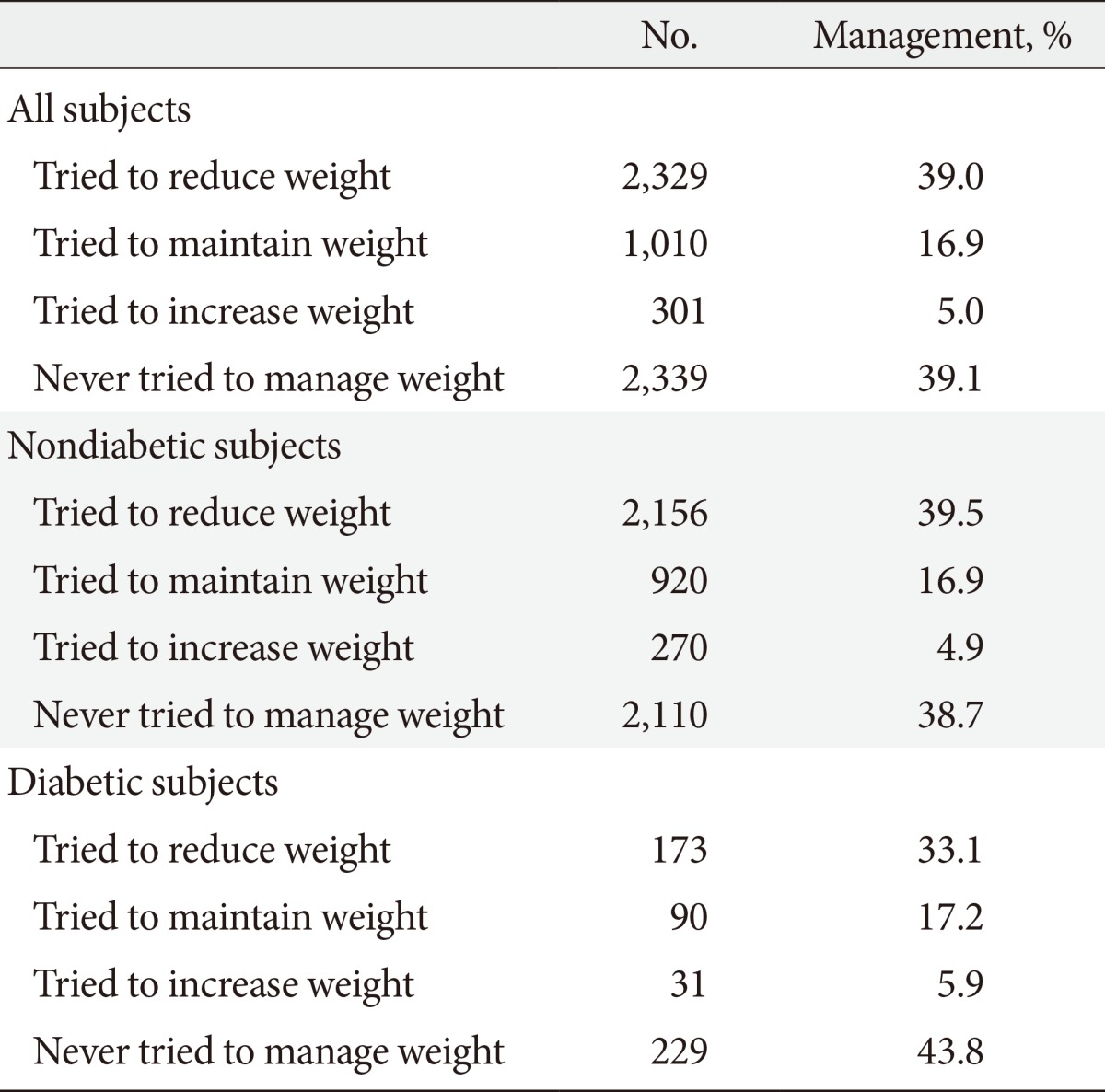
Management for obesity in the Korea National Health and Nutrition Examination Survey in 2011
The most common method for weight control was doing exercises in both groups (40.3%, 40.5%, respectively), while the second most common method was food intake reduction (32.6% in nondiabetic subjects, 26.2% in diabetic subjects, respectively). In both groups, other methods to control weight such as for fasting more than 24 hours, skipping meal, use of self-purchased antiobesity drugs, use of prescribed antiobesity drugs, taking Korean traditional herbal medication, taking health functional food, and one food diet were all attempted by less than 5% of the subjects.
Trends in prevalence, awareness, and management of obesity, 1998 to 2011
A total of 8,117, 5,826, 5,500, 3,025, 6,756, 7,506, 6,255, and 6,155 responses were available for analysis from the KNHANES in the 1998, 2001, 2005, 2007, 2008, 2009, 2010, and 2011, respectively.
Table 4 shows the prevalence of obesity and abdominal obesity in the KNHANES during 1998 to 2011. Although the prevalence of obesity in 2011 has increased by 1.19-fold compared to 1998, it has remained steady since 2005. In terms of abdominal obesity, its prevalence had gradually been increasing as years go by, reaching a peak in 2007. In diabetic patients, the prevalence of obesity and abdominal obesity in 2011 increased by 17.4% and 7.2% compared to 1998.
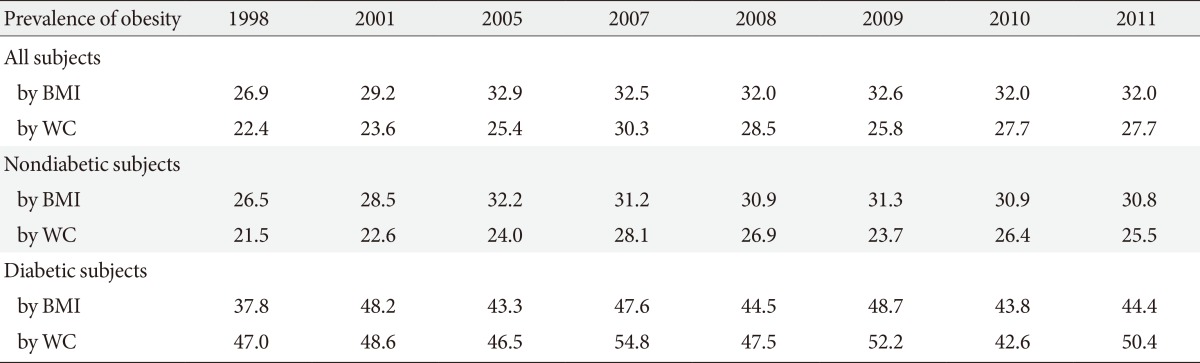
Prevalence of obesity and abdominal obesity in the Korea National Health and Nutrition Examination Survey during 1998 to 2011
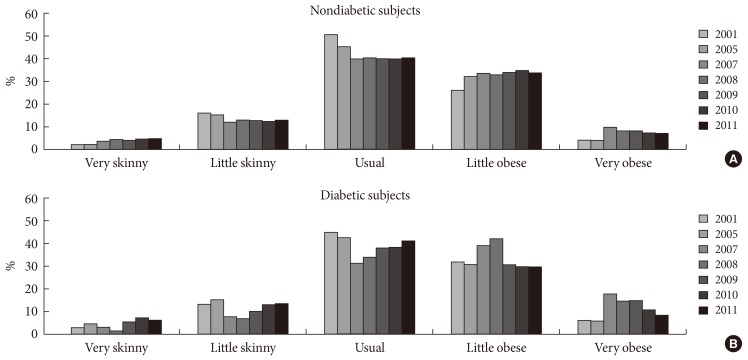
Participants with diabetes had higher prevalence of mild and severe obesity than nondiabetic subjects during 1998 to 2011 (Fig. 1). The prevalence of severe obesity showed a gradually increasing trend as years go by, and especially it reaching 7.6% in diabetic and 3.7% in nondiabetic subjects in 2009.

The proportion by body mass index-category according to the presence of diabetes in the Korea National Health and Nutrition Examination Survey during 1998 to 2011. (A) Nondiabetic subjects. (B) Diabetic subjects.
In nondiabetic subjects, subjective awareness for mild obesity showed an increasing tendency throughout 2001 to 2011, but subjects who considered their body sizes to be very obese gradually decreased since 2007 (Fig. 2). The number of subjects with diabetes who considered their body shape to be normal has been increasing since 2007. However subjective awareness for mild or severe obesity showed a decreasing trend from 2007 instead (Fig. 2).
The subjective awareness for obesity according to the presence of diabetes in the Korea National Health and Nutrition Examination Survey during 2001 to 2011. (A) Nondiabetic subjects. (B) Diabetic subjects.
Management rate for weight reduction tended to increase in nondiabetic subjects, reaching from 25.3% in 2001 to 39.0% in 2011 (Fig. 3). In case of diabetic subjects, treatment rate tended to decrease during 2008 to 2011, although compared to 17.6% in 2001 it increased significantly to 33.1% in 2011 (Fig. 3).
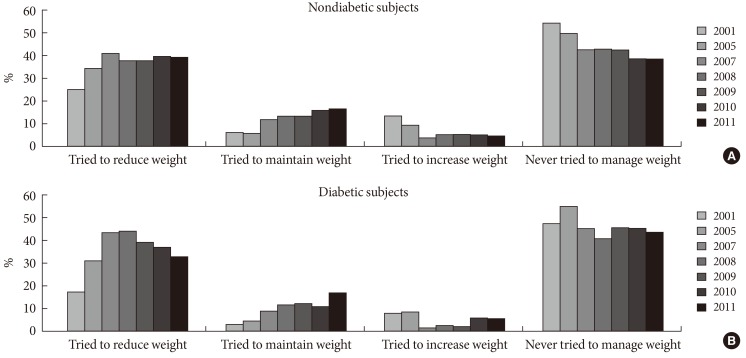
The management for obesity according to the presence of diabetes in the Korea National Health and Nutrition Examination Survey during 2001 to 2011. (A) Nondiabetic subjects. (B) Diabetic subjects.
The most frequently used method for weight control was exercise and food intake reduction in both nondiabetic and diabetic subjects throughout 2005 to 2011 (Fig. 4). Other methods tended to be unpopular, however in diabetic subjects skipping meals or fasting methods were employed by roughly 60% of nondiabetic subjects in 2011 (Fig. 4).
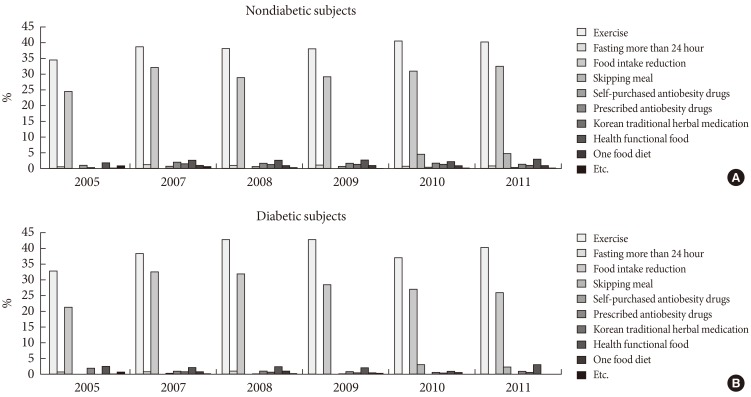
The method for weight control according to the presence of diabetes in the Korea National Health and Nutrition Examination Survey during 2005 to 2011. (A) Nondiabetic subjects. (B) Diabetic subjects.
DISCUSSION
The prevalence of obesity has risen above 30% in both men and women from 2005, but has stopped increasing since. The findings from the current study were consistent with those from the previous studies on general obesity using BMI [12]. The global trends of obesity epidemiology were quite different, being stable in the United States whereas increases were still observed in some European and Asian countries [13].
In general, obesity was more frequent in diabetic subjects than nondiabetic subjects throughout 1998 to 2011 in this analysis. As is well known, obesity increases the risk of long-term vascular complications of type 2 diabetes mellitus (T2DM), including stroke, chronic kidney disease, heart disease, peripheral vascular disease, and death [14].
Meanwhile, the prevalence of abdominal obesity did not exceed 30% during 1998 to 2011 except only for 2007. On the other hand, abdominal obesity was more common in diabetic subjects compared to nondiabetic subjects throughout 1998 to 2011, and unlike nondiabetic subjects the prevalence of abdominal obesity was higher than general obesity in diabetic subjects. These results mean that abdominal obesity is considered to be more closely associated with the risk of obesity-related complications such as diabetes [15]. Therefore measuring both BMI and waist circumference in clinical practice is still important although there have been some debates [16]. Indeed, although it is fortunate that the prevalence of obesity did not increase recently, a nationwide effort will be needed for the further reduction of obesity.
In this study we showed that the prevalence of obesity increased until 70 years of age and then begins to decline, which is a general trend [17], where diabetic subjects reach a peak prevalence of obesity in their 40s. This result may be associated with the recently elevated mortality rate of the 40s in Korea [18].
We tracked the changes of the proportion of subjects by BMI-category during 1998 to 2011. From this analysis we found that the subjects with diabetes had higher prevalence of mild and severe obesity compared to nondiabetic subjects over the analyzed period. The prevalence of mild obesity (BMI 25 to 29.9 kg/m2) had been gradually decreasing from 2007, but the prevalence of severe obesity (BMI ≥30 kg/m2) had been gradually increasing instead in nondiabetic subjects, although the overall obesity prevalence was the same during that period. This indicates that there has been a shift from mild to severe obesity in Korea. Perhaps for this reason bariatric surgeries for obesity management was introduced in Korea, and is now spreading over the nation and generating a great deal of public interest [19].
We investigated the awareness of obesity in a subjective manner. In nondiabetic subjects, the number of subjects who considered their body sizes to be a little skinny or normal has been gradually decreasing while subjects who thought that they are obese or very obese have been increasing during 2001 to 2011. Ironically, although the actual obesity rate was more common in diabetic subjects, the awareness for obesity was higher in nondiabetic subjects in the two most recent analyses. This phenomenon means that current diabetic subjects in Korea do not have appropriate insight for obesity, which we consider to be a serious problem [20].
The unmet need for obesity management of a concern. More than half of the subjects exceeded the normal body size in this analysis. Nevertheless, the number of subjects who tried to reduce body weight did not exceed 40% throughout 1998 to 2011 except in 2007, though fortunately the percentage of subjects trying to reduce or maintain body weight has gradually increased over the decade. This unmet need is greater among subjects with T2DM; the number of those who tried to reduce body weight weren't different to nondiabetic subjects, even though the percentage of being overweight and obesity during 1998 to 2011 was near 70% in this study. This effort did not increase but rather decreased constantly since 2007 in diabetic subjects. Moreover, in the two most recent analyses (2010 and 2011), the effort to reduce body weight in diabetic subjects was less than nondiabetic subject in spite of higher prevalence of obesity, which is a serious problem.
The most commonly used methods for obesity management were doing exercises and reducing food intake in both nondiabetic and diabetic subjects. However the proportion of diabetic subjects who manage their body weight by skipping or fasting meals were lower than nondiabetic subjects. This is thought to be due to diabetes-related education such as how to avoid hypoglycemia. Indeed, if diabetic subjects skip or eat the meal incorrectly the risk of hypoglycemia becomes greater. Furthermore, uses of self-purchased or prescribed anti-obesity drugs were very low (both less than 5% in total), which may be due to related adverse effects or because antiobesity drugs are not covered by the medical insurance in Korea. Instead, the use of easily available health promotion food was more frequent than antiobesity drugs.
In this study, the prevalence of obesity was assessed primarily by BMI and waist circumference, although some studies also assessed obesity by waist to hip ratio [21,22]. Moreover, the need for measuring both BMI and waist circumference in clinical practice is debated [16] even though waist circumference is a strong predictor of cardiometabolic risks.
There can be some possible limitations in this study. Firstly, although the KNHANES is national representative, it is a cross-sectional evaluation of the health and nutritional status of Koreans. Nevertheless, the KNHANES is one of the most accurate cross-sectional evaluations of the health status of contemporary Koreans. To our knowledge, this is the first nationwide epidemiologic study to evaluate the trends of the prevalence of obesity including awareness and management situations in Korean adults. Secondly, social and environmental factors which could affect obesity were not considered. Further studies are required to investigate the detailed reasons for the observed upward trends in obesity prevalence. Finally, the results of diabetic subjects analyses should also be interpreted with caution because of the relatively small sample size.
In conclusion, the prevalence of obesity in Korea showed a gradually increasing trend which have now become steady with the recent prevalence of over 30%. Moreover, the prevalence of severe obesity had gradually been increasing as years go by. In diabetic subjects, obesity is more common than nondiabetic subjects throughout 1998 to 2011. Awareness and management rates of obesity improved over the period of surveys. However, the awareness for obesity is higher in nondiabetic subjects in the most recent two analyses even though the actual obesity rate was higher in diabetic subjects. Thus more attention should be paid to diabetic subjects with chronic diseases, pertinent to obesity that may in future be manifested in Korea. Finally, although the management status of obesity has improved during the recent years, proper lifestyle management with weight reduction and regular exercises are recommended to reduce the burden of obesity.
Notes
No potential conflict of interest relevant to this article was reported.