Performance of Fast-Acting Aspart Insulin as Compared to Aspart Insulin in Insulin Pump for Managing Type 1 Diabetes Mellitus: A Meta-Analysis
Article information

Abstract
Background
No meta-analysis has analysed efficacy and safety of fast-acting aspart insulin (FIAsp) with insulin pump in type 1 diabetes mellitus (T1DM).
Methods
Electronic databases were searched for randomised controlled trials (RCTs) involving T1DM patients on insulin pump receiving FIAsp in intervention arm, and placebo/active comparator insulin in control arm. Primary outcome was to evaluate changes in 1- and 2-hour post-prandial glucose (1hPPG and 2hPPG). Secondary outcomes were to evaluate alterations in percentage time with blood glucose <3.9 mmol/L (hypoglycaemia), time in range (TIR) blood glucose 3.9 to 10 mmol/L, insulin requirements and adverse events.
Results
Data from four RCTs involving 640 patients was analysed. FIAsp use in insulin pump was associated with significantly greater lowering of 1hPPG (mean difference [MD], –1.35 mmol/L; 95% confidence interval [CI], –1.72 to –0.98; P<0.01; I2=63%) and 2hPPG (MD, –1.19 mmol/L; 95% CI, –1.38 to –1.00; P<0.01; I2=0%) as compared to controls. TIR was comparable among groups (MD, 1.06%; 95% CI, –3.84 to 5.96; P=0.67; I2=70%). Duration of blood glucose <3.9 mmol/L was lower in FIAsp group, approaching significance (MD, –0.91%; 95% CI, –1.84 to 0.03; P=0.06; I2=0%). Total hypoglycaemic episodes (risk ratio [RR], 1.35; 95% CI, 0.55 to 3.31; P=0.51; I2=0%), severe hypoglycaemia (RR, 2.26; 95% CI, 0.77 to 6.66; P=0.14), infusion site reactions (RR, 1.35; 95% CI, 0.63 to 2.93; P=0.77; I2=0%), and treatment-emergent adverse events (RR, 1.13; 95% CI, 0.80 to 1.60; P=0.50; I2=0%) were comparable.
Conclusion
FIAsp use in insulin pump is associated with better post-prandial glycaemic control with no increased hypoglycaemia or glycaemic variability.
INTRODUCTION
Insulin pumps, based on closed loop systems are recommended for managing type 1 diabetes mellitus (T1DM). Hybrid close loop systems typically have associated continuous glucose monitoring (CGM) using proprietary algorithms which help in adjusting insulin infusion rates with the aim of proving better glycaemic control with lower risks of hypoglycaemia [1]. However one issue which remains a challenge even with the best of close loop system insulin pumps is the slower than physiologic absorption of analogue mealtime insulin like insulin glulisine, insulin lispro or insulin aspart, making postprandial blood glucose control difficult [2]. Fast-acting aspart insulin (FIAsp) is a novel insulin that contains niacinamide and l-arginine resulting in faster initial absorption of insulin aspart (IAsp). FIAsp subcutaneously has been shown to have greater early glucose lowering effect than aspart insulin [3]. Clamp studies have confirmed 57% earlier onset of appearance and a 35% earlier time to reach 50% maximum concentration for FIAsp as compared to aspart insulin [4]. In a pooled analysis of data from 218 adult people with T1DM from six randomised controlled trials (RCTs), comparing subcutaneous FIAsp injections with subcutaneous aspart injections revealed FIAsp potential to better mimic the physiologic prandial insulin secretion and thereby to improve post-prandial glucose control compared to aspart insulin [2].
Hence mechanistically FIAsp insulin should be better for using in insulin pumps as compared to aspart and other analogue short acting insulins. There have been several RCTs published evaluating the role of FIAsp with different insulin pumps [5]. However till date, no meta-analysis have been published evaluating the performance of FIAsp insulin in insulin pump devices. This meta-analysis was undertaken to address this knowledge-gap.
METHODS
Methodology
The meta-analysis was carried out according to the recommendations of the Cochrane Handbook for Systematic Reviews of Interventions [6]. The predefined protocol has been registered in the International Prospective Register of Systematic Reviews (PROSPERO) having Registration number of CRD42021291584. All RCTs published till October 2021 were considered for this meta-analysis. This meta-analysis has been reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [6]. Since ethical approval already exists for the individual studies included in the meta-analysis, our review was exempt from ethics approval.
The PICOS (patient, intervention, control, outcome and study type) criteria was used to screen and select the studies for this meta-analysis, with patients (P) being people living with T1DM; intervention (I) being use of FIAsp insulin in insulin pump device for managing T1DM; control (C) being patients either on any other approved insulin in insulin pump for managing T1DM; outcomes (O) being evaluated were impact on blood glucose parameters, time in range (TIR), hypoglycaemia and any adverse effects noted. Only patients with T1DM were considered for this meta-analysis. Only those studies were included in this meta-analysis which had at least two treatment arms/groups, with one of the groups having patients with T1DM on FIAsp in insulin pump and the other arm/group receiving any other insulin in place of FIAsp in insulin pump.
The primary outcomes were to evaluate the changes in 1- and 2-hour post-prandial glucose (1hPPG and 2hPPG). The secondary outcomes of this study was to evaluate alterations in different parameters of CGM like percentage of time in blood glucose <3.9 mmol/L, TIR blood glucose 3.9 to 10 mmol/L, daily insulin requirements, hypoglycaemia, and adverse events.
Search method for identification of studies
A detailed electronic databases of Medline (Via PubMed), Embase (via Ovid SP), Cochrane central register of controlled trials (CENTRAL) (for trials only), ctri.nic.in, clinicaltrials.gov, global health, and Google scholar were searched using a Boolean search strategy: (fast acting aspart) OR (aspart insulin) AND (diabetes).
Data extraction and study selection
Data extraction was carried out independently by two authors using standard data extraction forms. In cases where more than one publication of a single study group were found, results were grouped and relevant data from each report were used in the analyses. Data on the primary and secondary outcomes as stated above was extracted. Patient characteristics (including demographic information and comorbidities) from the different studies included in the analysis were noted in a tabular form (Table 1). All disagreements were resolved by the third and fourth authors. The flow of data extraction and study selection has been elaborated in Supplementary Fig. 1.

Patients characteristics of the different randomised controlled trials evaluated in this meta-analysis
Assessment of risk of bias in included studies
Three authors independently assessed the risk of bias using the risk of bias assessment tool in Review Manager (Revman) version 5.3 (The Cochrane Collaboration, Oxford, UK, 2014) software. The different types of bias looked for have been elaborated in a previous metanalysis by our group [7].
Measures of treatment effect
For continuous variables, the outcomes were expressed as mean difference (MD). International System (SI) units were used for analysis, and all studies reporting results in conventional units were converted to SI units for analysis. RevMan version 5.3 was used for comparing different primary and secondary outcomes between FIAsp insulin and control group.
Assessment of heterogeneity
Heterogeneity was initially assessed by studying the forest plot generated for the primary and secondary outcomes. Subsequently heterogeneity was analysed using a chi2 test on N-1 degrees of freedom, with an alpha of 0.05 used for statistical significance and with the I2 test [8]. The detail of assessment and interpretation of heterogeneity has already been elaborated elsewhere [7].
Grading of the results
An overall grading of the evidence (certainty of the evidence) related to each of the primary and secondary outcomes of the meta-analysis was done using the Grades of Recommendation, Assessment, Development and Evaluation (GRADE) approach [9]. The details of how grading of the study results was done and how the summary of findings table was developed (Table 1) has been elaborated elsewhere [7]. Publication bias was assessed by plotting the funnel plot, which specifically targets small study bias, in which small studies tend to show larger estimates of effects and greater variability than larger studies [9]. Presence of one or more of the smaller studies outside the inverted funnel plot was taken as evidence of presence of significant publication bias [10]. The funnel plots of the key outcomes of this study have been elaborated in Supplementary Fig. 2.
Data synthesis
Data was pooled as random effect model for the analysis of primary and secondary outcomes. The outcomes were expressed as 95% confidence intervals (CIs). Forrest plots were plotted with the left side of the graph favouring FIAsp insulin and the right side of the graph favouring control using RevMan 5.3 software. P<0.05 was considered statistically significant.
RESULTS
A total of 257 articles were found after the initial search (Supplementary Fig. 1). Following the screening of the titles, abstracts, followed by full-texts, the search was reduced down to 105 studies which were evaluated in detail for inclusion in this meta-analysis (Supplementary Fig. 1). Four RCTs which fulfilled all criteria were analysed in this meta-analysis [5,11-13].
In the study by Ozer et al. [5], 40 people with T1DM were randomized to receive FIAsp or aspart insulin through Med-tronic 670G system in a cross-over fashion. In the study by Boughton et al. [11], 25 people with T1DM were randomized to receive FIAsp or aspart insulin through the Dana Diabecare RS insulin pump, where the insulin delivery is directed through the CamAPS FX app (CamDiab, Cambridge, UK) which resides on an any Android phone, that receives sensor glucose data from the Dexcom G6 transmitter creating a closed loop system. In the study by Klonoff et al. [12], 472 people with T1DM were randomized to receive either FIAsp or aspart insulin through MiniMed530G insulin pump (Paradigm Veo, Paradigm Revel or Paradigm, Medtronic Inc., Minneapolis, MN, USA) for continuous subcutaneous insulin infusion therapy. In the study by Hsu et al. [13], 19 people with T1DM were randomized to receive either FIAsp or aspart insulin through MiniMed670G insulin pump (Medtronic, Northridge, CA, USA). The duration of study was 6, 8, 16, and 2 weeks respectively in the RCTs by Ozer et al. [5], Boughton et al. [11], Klonoff et al. [12], and Hsu et al. [13] respectively, after which cross-over switch was done for the study participants for same time period.
The RCT by Russel et al. [14] was excluded as it used only FIAsp insulin with different settings of the insulin pump in the three different arms of the RCT. The study by Grosman et al. [15] was excluded as it was done using a virtual patient simulation and not in real patients. The study by Tsoukas et al. [16] was excluded as it used pramlintide along with FIAsp insulin in the insulin pump closed loop system. The details of the studies included in this meta-analysis have been elaborated in Table 1.
Risk of bias in the included studies
The summaries of risk of bias of the four studies included in the meta-analysis have been elaborated in Fig. 1. Random sequence generation, allocation concealment, attrition bias and, reporting bias were judged to be at low risk of bias in all the four studies (100%). Performance and detection bias were low risk in three out of four studies (75%). Source of funding, especially pharmaceutical, authors from the pharmaceutical organizations and conflict of interests were looked into the “other bias” section. Other bias were judged to be at low risk in two out of four studies (50%) (Fig. 1). Further details have been elaborated in Supplementary Table 1.
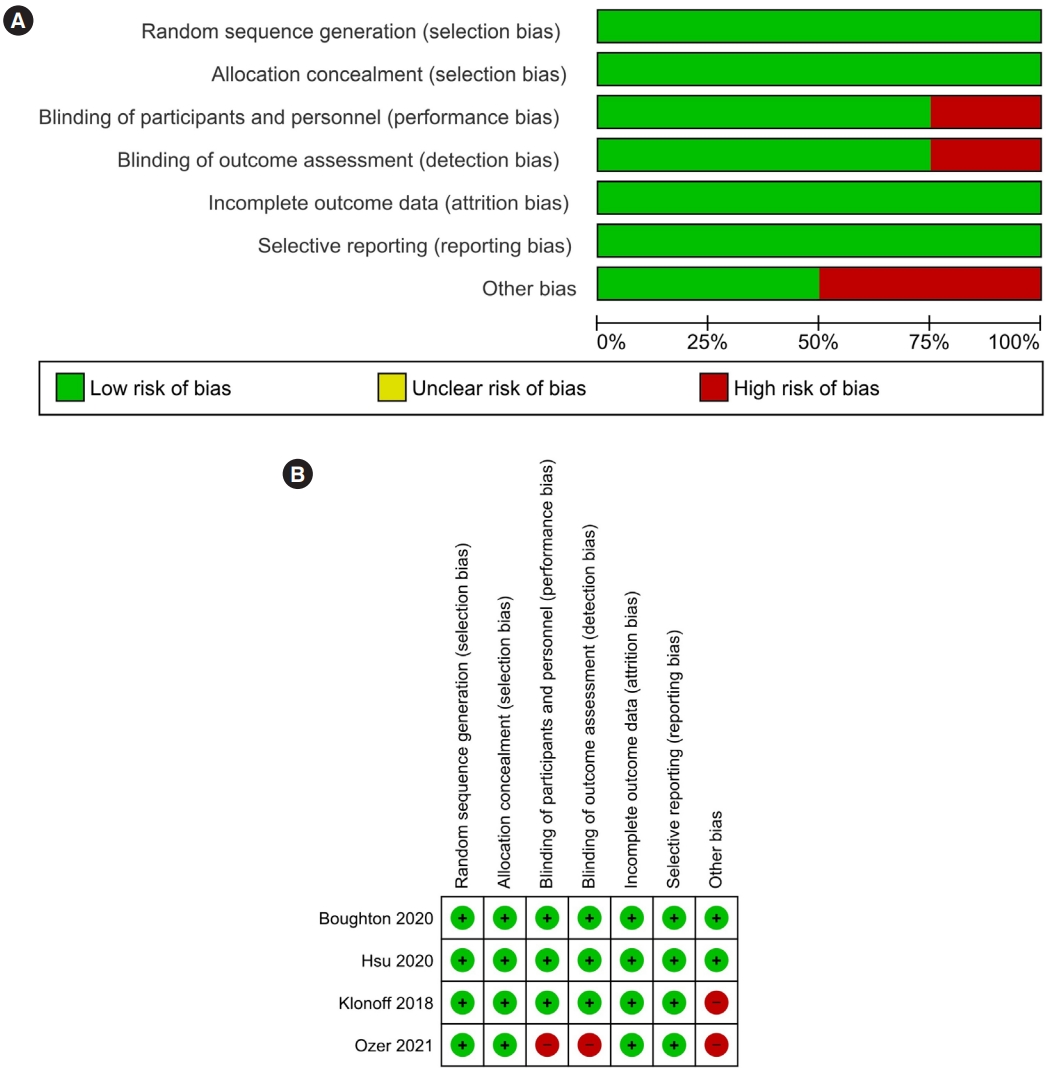
(A) Risk of bias graph: review authors’ judgements about each risk of bias item presented as percentages across all included studies. (B) Risk of bias summary: review authors’ judgements about each risk of bias item for each included study.
Effect of FIAsp on primary outcomes
One-hour and 2-hour post-prandial glucose
Data from two studies involving 535 people with T1DM was analysed to find out the impact of FIAsp on 1hPPG. Individuals receiving FIAsp had significantly greater lowering of 1hPPG as compared to those receiving conventional aspart insulin (MD, –1.35 mmol/L; 95% CI, –1.72 to –0.98); P<0.01; I2=63% for moderate heterogeneity) (Fig. 2A). Data from two studies involving 552 people with T1DM was analysed to find out the impact of FIAsp on 2hPPG. Individuals receiving FIAsp had significantly greater lowering of 2hPPG as compared to those receiving conventional aspart insulin (MD, –1.19 mmol/L; 95% CI, –1.38 to –1.00; P<0.01; I2=0% for low heterogeneity) (Fig. 2B).
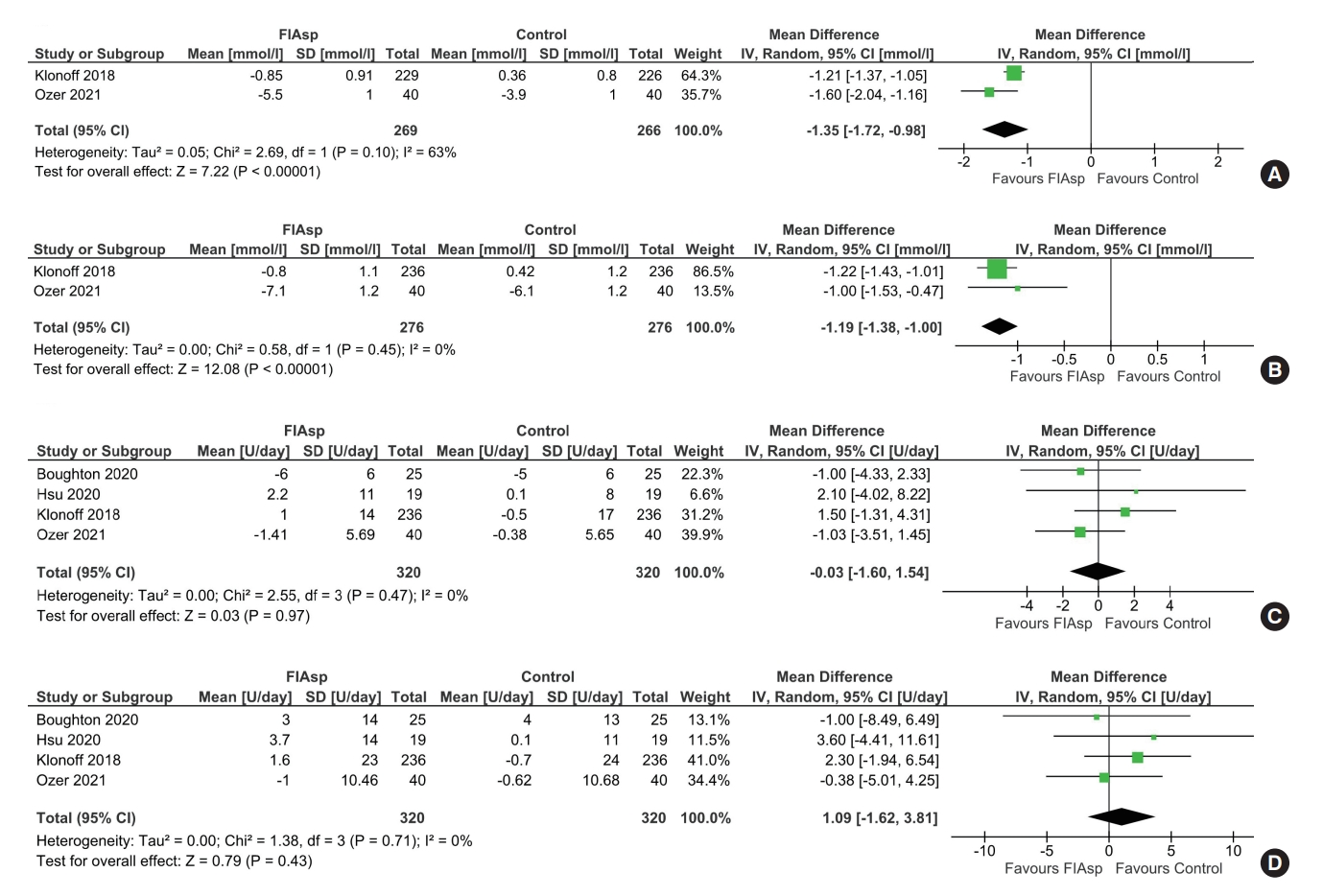
Forest plot highlighting the impact of fast-acting aspart insulin (FIAsp) as compared to aspart insulin on (A) 1-hour postprandial glucose, (B) 2-hour post-prandial glucose, (C) total daily bolus insulin, and (D) total daily insulin requirement. SD, standard deviation; IV, inverse variance; CI, confidence interval.
Effect of FIAsp on secondary outcomes
Insulin requirements
Data from four studies involving 640 people with T1DM was analysed to find out the impact of FIAsp on daily bolus insulin requirement and well as total daily insulin requirement via the insulin pump as compared to those receiving aspart insulin. Daily bolus insulin requirement (MD, –0.03 U; 95% CI, –1.60 to 1.54; P=0.97; I2=0% for low heterogeneity) (Fig. 2C) as well as total daily insulin requirement (MD, 1.09 U; 95% CI, –1.62 to 3.81; P=0.43; I2=0% for low heterogeneity) (Fig. 2D) were similar among the two study groups.
CGM glycaemic parameters
Data from two studies (88 patients) were analysed to evaluate the impact of using FIAsp insulin in place of conventional aspart insulin in insulin pump on the TIR, defined as percentage time having blood glucose in the range of 3.9 to 10.0 mmol/L, and on time in hypoglycaemia on CGM, defined as percentage time having blood glucose <3.9 mmol/L. TIR was comparable among the two study groups (MD, 1.06%; 95% CI, –3.84 to 5.96; P=0.67; I2=70% for moderate heterogeneity) (Fig. 3A). Time in hypoglycaemia was lower among patients receiving FIAsp as compared to conventional aspart insulin, which approached statistical significance (MD, –0.91%; 95% CI, –1.84 to 0.03; P=0.06; I2=0% for low heterogeneity) (Fig. 3B).
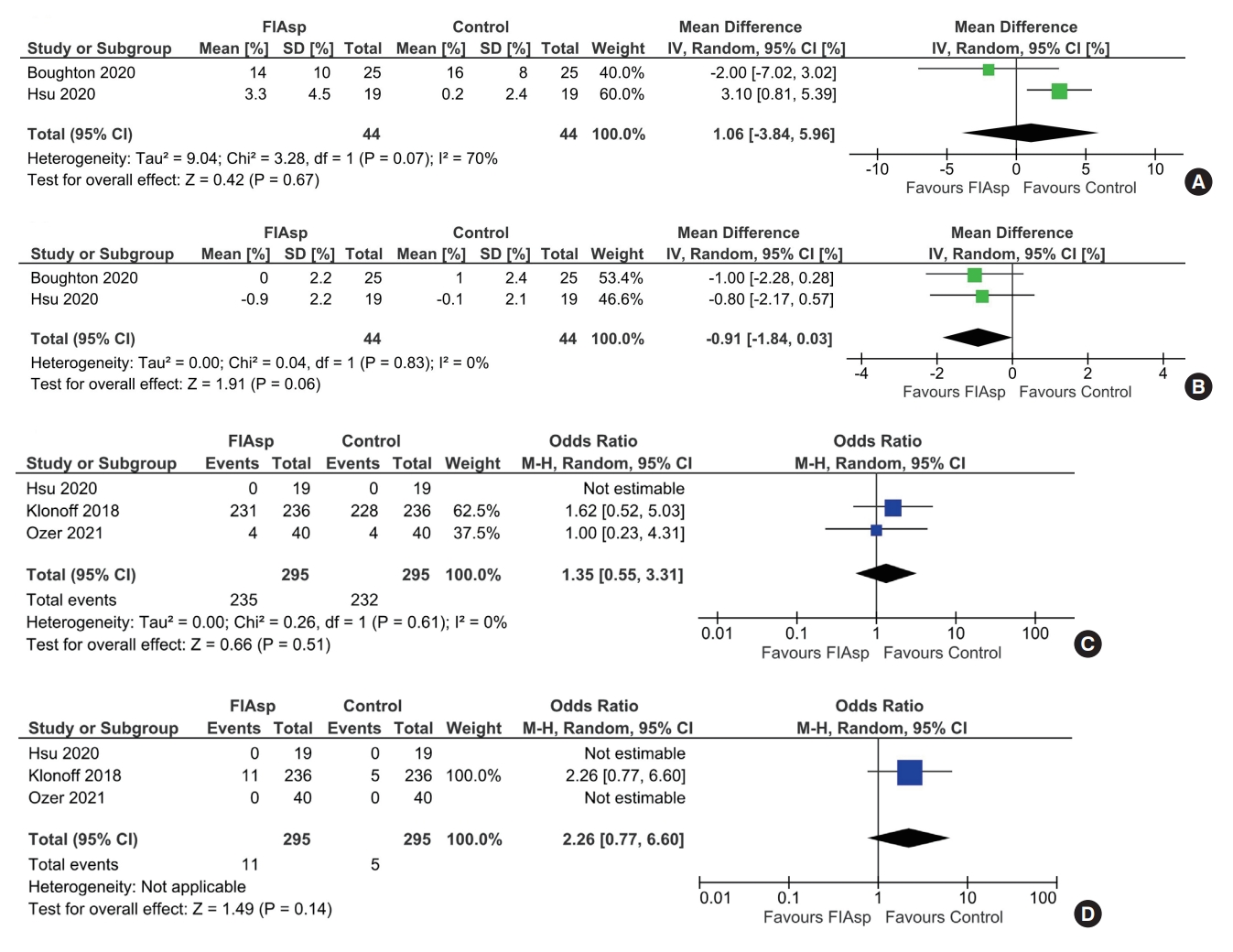
Forest plot highlighting the impact of fast-acting aspart insulin (FIAsp) as compared to aspart insulin on (A) percent time in hypoglycaemia range (blood glucose <3.9 mmol/L), (B) time in range (blood glucose 3.9 to 10 mmol/L), (C) total hypoglycaemia episodes, and (D) severe hypoglycaemia episodes. SD, standard deviation; IV, inverse variance; CI, confidence interval; M-H, Mantel-Haenszel.
Glycosylated hemoglobin reduction
Data from one study involving 472 patients [12] was available analysing percentage of people achieving glycosylated hemoglobin (HbA1c) <7% (53 mmol/mol). The percentage of people achieving glycaemic targets was comparable among the two study groups (MD, 0.84; 95% CI, 0.54 to 1.3; P=0.44). In the study by Ozer et al. [5], HbA1c reduction was marginally better in the FIAsp group (–0.06%) as compared to the aspart group, but statistically not significant.
Safety
Data from three studies (590 patients) was analysed to evaluate the impact of FIAsp as compared to aspart insulin on the occurrence of total hypoglycaemic episodes and severe hypoglycaemia episodes. The occurrence of total hypoglycaemic episodes (risk ratio [RR], 1.35; 95% CI, 0.55 to 3.31; P=0.51; I2=0% for low heterogeneity) high certainty of evidence (Fig. 3C) and severe hypoglycaemia episodes (RR, 2.26; 95% CI, 0.77 to 6.66; P=0.14) (Fig. 3D) was comparable among two study groups. Data from four studies (640 patients) was analysed to evaluate impact of FIAsp insulin as compared to aspart insulin on occurrence of adverse events (treatment-emergent adverse events [TAEs] and severe adverse events [SAEs]). The occurrence of TAEs (RR, 1.13; 95% CI, 0.80 to 1.60; P=0.50; I2=0% for low heterogeneity) (Fig. 4A) and SAEs (RR, 1.00; 95% CI, 0.25 to 4.05; P=1.00) (Fig. 4B) were not significantly different among the two study groups.
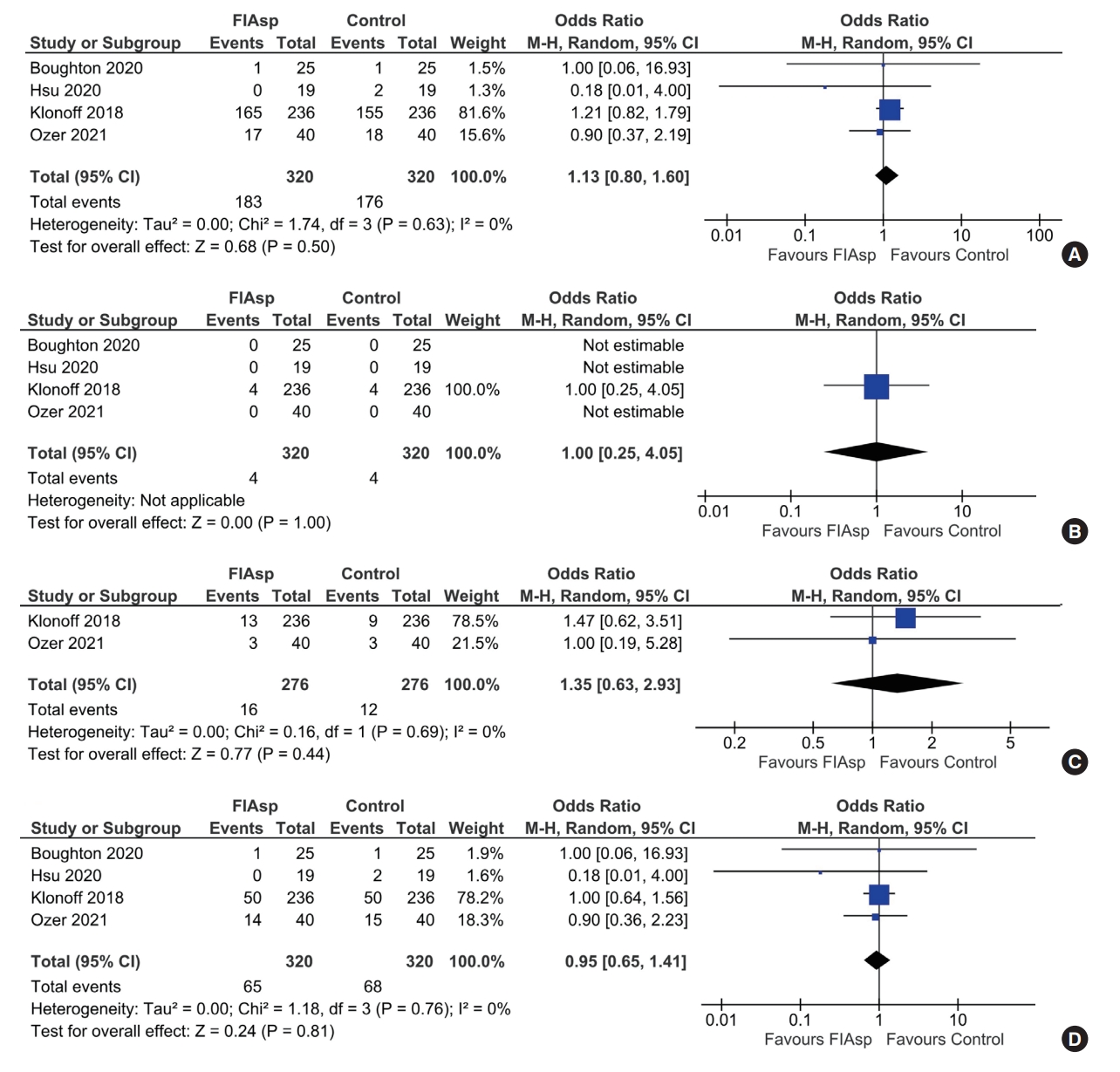
Forest plot highlighting the impact of fast-acting aspart insulin (FIAsp) as compared to aspart insulin on (A) treatment-emergent adverse events, (B) severe adverse events, (C) infusion site reactions, and (D) occlusion events. M-H, Mantel-Haenszel; CI, confidence interval.
Data from two studies (552 patients) was analysed to evaluate the occurrence of insulin infusion site reactions in patients receiving FIAsp as compared to aspart insulin. The occurrence of infusion site reactions was comparable across the study groups (RR, 1.35; 95% CI, 0.63 to 2.93; P=0.77; I2=0% for low heterogeneity) (Fig. 4C). Data from four studies (640 patients) was analysed to evaluate the occurrence of occlusion episodes in patients receiving FIAsp as compared to aspart insulin. The occurrence of infusion site reactions was comparable across study groups (RR, 0.95; 95% CI, 0.65 to 1.41; P=0.81; I2=0% for low heterogeneity) (Fig. 4D). The summary of findings of the key outcomes of this study has been elaborated in Table 2.

Summary of findings of the key outcomes of the study
DISCUSSION
The story of development of prandial insulins have always been about faster onset of action to mimic as close as possible to endogenous prandial insulin secretion. Monomeric insulins like conventional aspart insulin, lispro insulin, and apidra insulin were found to be better than regular human insulin with regards to control of post-prandial glycaemic excursions both in T1DM and type 2 diabetes mellitus, with increased treatment satisfaction especially in people living with T1DM [17,18]. A recent meta-analysis documented subcutaneous aspart and lispro insulin injections to be more effective in controlling 1-hour and 2-hour post meal hyperglycaemia without any increase in hypoglycaemia or glycaemic variability [17]. FIAsp insulin is a further advancement in the field of monomeric insulins towards faster onset of insulin action. Heise et al. [2] in a pooled analysis of pharmacology trials data showed that subcutaneous FIAsp insulin injection use was associated with 4.9 minutes (95% CI, –5.3 to –4.4) earlier onset of action, two times greater exposure to insulin in the first 30 minutes post-injection, 74% greater (odds ratio, 1.74; 95% CI, 1.47to 2.10) early glucose lowering effect in the first 30 minutes postinjection and 12.2 minutes (95% CI, –17.9 to –6.5) earlier offset of exposure, as compared to monomeric aspart insulin. FIAsp insulin when administered subcutaneously up to 20 minutes after the start of meals continued to provide similar glycaemic control as compared to pre-prandial aspart insulin administration [19]. Our meta-analysis showed that these pharmacokinetic and pharmacodynamic benefits actually translates into meaningful clinical benefits when FIAsp insulin is used in insulin pump.
This is the first meta-analysis to highlight the glycaemic efficacy and side effect profile of FIAsp insulin as compared to aspart insulin in insulin pumps for managing T1DM. Over 2 to 12 weeks of clinical use, FIAsp had similar glycaemic efficacy as compared to aspart in insulin. FIAsp performed significantly better than aspart insulin with regards to control of 1hPPG and 2hPPG. Percentage of time spent in TIR on CGM was comparable for both the insulins. FIAsp use was associated with lower time spent in hypoglycamia range (<3.9 mmol/L) which approached statistical significance. Total daily insulin dose requirement was marginally higher with FIAsp but not statistically significant. Totally hypoglycaemia and severe hypoglycaemic episodes were comparable across both the insulin groups. Also TAEs, SAEs, infusion site reaction, and occlusions were not different with regards to FIAsp or aspart insulin use. The accelerated absorption kinetics of FIAsp insulin suggested that when switching to FIAsp in insulin pump, the bolus dosing will need to be adjusted to reduce the potential risk of early post‐prandial hypoglycaemia or late post‐prandial hyperglycaemia [20]. A good understanding of glycaemic index and the meal composition would further help in improving the glycaemic outcomes.
Limitations of this meta-analysis include the relative small number of patients in few studies. Three of the four studies used hybrid closed loop insulin pump system, and one study used conventional insulin pump with CGM. Hence analysing them together is also a limitation of this study. However sub-group analysis could not be done as there was only one study in the conventional insulin pump with CGM sub-group. The duration of study was short in most of the studies. Hence long term impact on HbA1c is not available from this meta-analysis. This meta-analysis highlights the need for larger RCTs with longer follow-up of at least 1 year to evaluate the efficacy, safety and glycaemic durability of FIAsp insulin in insulin pump as compared to other short acting insulin. The cost of one 3 mL cartridge of 100 IU/mL of FIAsp insulin is similar to marginally lower than conventional aspart insulin (Novorapid, Novo Nordisk, Bagsværd, Denmark) and lispro insulin (Humalog, Eli Lilly, Indianapolis, IN, USA) is different countries across the globe [21-24].
To conclude it may be said that FIAsp insulin may be considered as the best available mimic of the physiologic prandial insulin secretion. This meta-analysis provides us with reassuring data that use of FIAsp insulin in insulin pump is advantageous cause of better post-prandial glycaemic control with no increased risk of hypoglycaemia or glycaemic variability. Fiasp is a useful option especially in people with diabetes with difficulty in post-prandial glycemic control.
SUPPLEMENTARY MATERIALS
Supplementary materials related to this article can be found online at https://doi.org/10.4093/dmj.2022.0035.
Risk of bias assessment table
Flowchart elaborating on study retrieval and inclusion in the meta-analysis. Reason 1: lack of a valid control group [14]; Reason 2: was a virtual simulated study [15]; Reason 3: pramlintide was used along with fast-acting aspart insulin [16].
Funnel plot of all the included studies in the meta-analysis (assessing the publication bias) of the main outcomes assessed (A) 1-hour post-prandial glucose, (B) 2-hour post-prandial glucose, (C) treatment-emergent adverse events, (D) total hypoglycamia episode, and (E) occlusion episodes. SE, standard error; MD, mean difference; OR, odds ratio.
Notes
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTIONS
Conception or design: D.D., M.S.
Acquisition, analysis, or interpretation of data: R.M., K.M., M.S.
Drafting the work or revising: D.D., K.M., M.S.
Final approval of the manuscript: D.D., R.M., K.M., M.S.
FUNDING
None
Acknowledgements
None