Fasting Glucose Variability and the Risk of Dementia in Individuals with Diabetes: A Nationwide Cohort Study
Article information

Abstract
Background
We investigated whether fasting glucose (FG) variability could predict the risk of dementia.
Methods
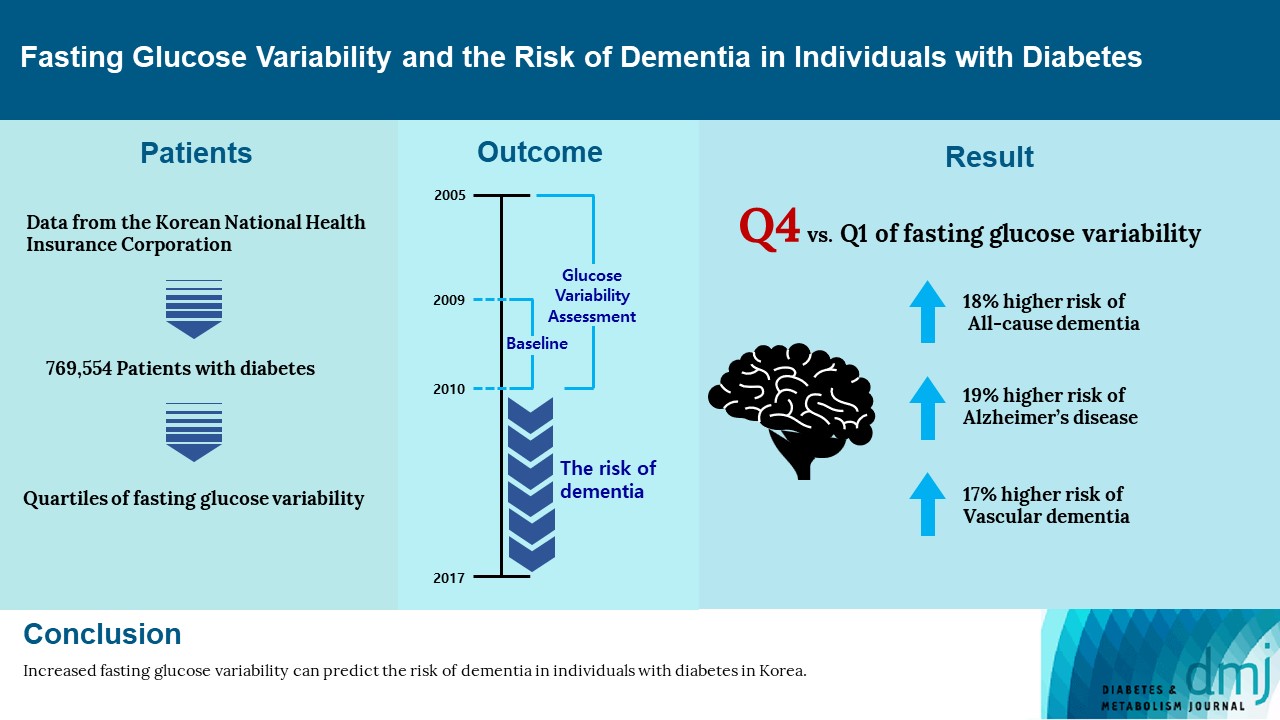
This cohort study analyzed data from Koreans with diabetes after at least three health examinations by the Korean National Health Insurance Corporation between 2005 and 2010, which included at least one examination between 2009 and 2010. A total of 769,554 individuals were included, excluding those aged <40 years and those with dementia. FG variability was measured using the variability independent of the mean (FG-VIM). The incidence of dementia was defined by the International Classification of Diseases 10th Revision codes and prescription of anti-dementia medication and was subdivided into Alzheimer’s disease (AD) and vascular dementia (VD).
Results
During the 6.9-year follow-up, 54,837, 41,032, and 6,892 cases of all-cause dementia, AD, and VD, respectively, were identified. Cox proportional regression analyses showed that as the FG-VIM quartile increased, the risk of dementia serially increased after adjustment for metabolic factors, income status, and diabetes-related characteristics, including the mean FG. Participants in FG-VIM quartile 4 showed a 18%, 19%, and 17% higher risk for all-cause dementia, AD, and VD, respectively, than those in quartile 1; this particularly included non-obese patients with a longer duration of diabetes, high FG levels, dyslipidemia, and those taking glucose-lowering medications. Conversely, the baseline FG status and dementia showed a U-shaped association.
Conclusion
Increased FG variability over 5 years can predict the risk of dementia in individuals with diabetes in Korea. This finding was more pronounced in patients with less favorable metabolic profiles.
INTRODUCTION
With the global increase in aging population, dementia is considered the primary cause of disability and dependency, with its prevalence nearly doubling every 20 years [1,2]. A growing body of evidence shows the adverse effects of diabetes on cognitive function and a 73% higher risk of all-cause dementia in people with diabetes than in those without [3,4]. Therefore, early correction of modifiable risk factors is essential to reduce the incidence of dementia.
Although the predictive value of diabetes-related biochemical indicators of cognitive disorders was inconsistent in previous studies, a recently published meta-analysis proved that elevated fasting glucose (FG), glycosylated hemoglobin (HbA1c), and insulin levels are associated with a high risk of dementia, and FG illustrated a nonlinear positive association with cognitive disorders [5]. However, another population-based study suggested that a history of hypoglycemia correlated with the risk of dementia [6]. Thus, considerable oscillation in FG levels is also a risk factor for the incidence of dementia.
Numerous population-based studies showed the effects of variability in cardiometabolic parameters, including blood pressure (BP) variability, weight change, and metabolic health status, on the development of dementia in patients with [7] or without diabetes [8,9]. In individuals with diabetes, high shortterm glucose variability (GV), assessed through a continuous glucose monitoring system, has been shown to predict cognitive decline independent of FG or HbA1c levels [10,11]. Fasting glucose variability (FGV) over several months to years, reflecting the stability of medication effect, adherence, and residual insulin secretion, was independently associated with dementia in two large population-based studies [12,13]. However, the risks of all-cause dementia, Alzheimer’s disease (AD), and vascular dementia (VD) were evaluated separately.
Therefore, we aimed to investigate the relationship between FGV over several years and the future risk of dementia from all causes, AD, and VD. We also explored the factors that modify this association using a nationwide cohort database in Korea.
METHODS
Study design
We analyzed the datasets of Korean individuals with diabetes obtained from the National Health Insurance Corporation (NHIC) of Korea that record information regarding health check-ups and claims information between January 2005 and December 2017. The NHIC is a universal healthcare system operated by the Korean government that covers approximately 97% of the Korean population. It contains eligibility information, an annual or biannual health examination database provided by the NHIC and claims data for prescriptions under the International Classification of Diseases, 10th Revision (ICD-10). Income status was estimated by the pricing of health insurance premiums or eligibility for medical care [14,15]. The health examination consisted of blood and urine tests, lifestyle questionnaires, and anthropometric measurements. The database is accessible to all researchers.
Study participants
As shown in Supplementary Figs. 1 and 2, we selected individuals with diabetes who underwent health check-ups at least twice from 2005 to 2008 and concomitantly at least once from January 2009 to December 2010 (baseline examination). Thus, the study participants underwent at least three health examinations during the 5 years from 2005 to 2010 (referred to as the GV assessment period). The presence of diabetes was defined as at least one claim per year for the prescription of a glucose-lowering medication (GLM) under ICD-10 codes E10–14 or a fasting plasma glucose level ≥126 mg/dL. We subdivided the participants into type 1 and type 2 diabetes mellitus based on ICD-10 codes E10 and E11–14, respectively.
Among them, participants aged <40 years, those with a history of dementia, those with missing data, and those diagnosed with dementia 1 year after baseline were excluded. In total, 769,554 individuals were included in the study. The present study was approved by the official review committee of the NHIC and the Institutional Review Board of the Korea University Ansan Hospital (2019AS0138) and was conducted in accordance with the Helsinki Declaration of 1975. Written informed consent by the patients was waived due to a retrospective nature of our study.
Definition of dementia
Dementia was defined using ICD-10 codes (F00, G30, F01, F02, F03, G23.1, G31.0, G31.1, G31.82, G31.83, G31.88, or F10.7), and concurrently, based on the prescription of one or more anti-dementia medications (acetylcholinesterase inhibitor [donepezil, rivastigmine, or galantamine] or N-methyl-D-aspartate receptor antagonist [memantine]) [16]. To define the subtypes of dementia, we grouped incident dementia into AD (ICD-10 codes F00 or G30) or VD (ICD-10 code F01), according to the diagnosis at the first visit [7,8]. If both AD and VD were identified, the ICD-10 code for the main diagnosis was used. When codes for both AD and VD, as additional diagnoses, were recorded at the first visit, we used the main diagnosis at the next visit. In cases where neither AD nor VD was the main diagnosis until the second visit, the subtype of dementia was defined as “other dementia.”
Definition of GV
Using at least three measurements of FG levels during the 5-year variability assessment period, we calculated the variability independent of the mean (VIM) of FG as a primary GV indicator.
To compare the predictive effect between parameters, the average real variability (ARV), standard deviation (SD), and coefficient of variation (CV, which is SD/mean) of the FG were computed.
β is obtained from a nonlinear regression analysis based on the natural logarithm of the SD over the natural logarithm of the mean [17].
n is the number of FG assessments and k ranges from 1 to n–1.
Measurements of covariates
Demographic information, lifestyle behavior, and medical history were recorded from the self-reported questionnaire during the health examination. Alcohol drinking habits were classified as near abstinence, moderate (<30 g/day), and heavy (≥30 g/day). Smoking history was graded as never smoker, ex-smoker, or current smoker. Regular exercise was defined as >30 minutes of moderate-intensity activity at least five times a week or >20 minutes of vigorous-intensity exercise at least three times a week [18].
Body mass index (BMI) was calculated as weight (kg) divided by the square of height (m). The BP was measured after ≥5 minutes of rest.
Blood sampling via vein was performed in the morning after at least 8 hours of overnight fasting to identify the concentrations of plasma glucose, total cholesterol, triglycerides, high-density lipoprotein cholesterol, creatinine, and hemoglobin. Low-density lipoprotein cholesterol levels were calculated using the Friedewald formula [19]. Quality control was performed in accordance with the guidelines of the Korean Association for Laboratory Quality Control.
Operational definition of comorbidities
Hypertension was defined as systolic BP ≥140 mm Hg, diastolic BP ≥90 mm Hg, or at least one prescription of antihypertensive medications per year under ICD-10 codes I10–I15. A total cholesterol level ≥240 mg/dL or at least one prescription of an antihyperlipidemic agent under ICD-10 code E78 was defined as dyslipidemia.
History of stroke or ischemic heart disease was identified based on self-reports of patients’ experiences after a physician’s diagnosis of stroke, angina, or myocardial infarction. The presence of chronic kidney disease was defined as an estimated glomerular filtration rate <60 mL/min/1.73 m2, calculated by the Modification of Diet in Renal Disease formula [20]. At least one recognition per year for the ICM-10 codes F32 or F33 was regarded as the presence of a depressive disorder. The lowest 20% income proportion was dichotomized into a low-income status.
Over an 1-year period before the baseline examination, the prescription histories for oral GLMs among metformin, sulfonylurea, meglitinide, thiazolidinedione, inhibitors of dipeptidyl peptidase 4, α-glucosidase inhibitors (AGIs), and insulin were identified.
Statistical analysis
Data are presented as the mean±SD, number (%), or median (interquartile range [IQR]). Study participants were stratified according to the FG VIM quartile. Baseline characteristics were compared using the chi-square test for categorical variables and analysis of variance for continuous variables. Variables, including triglyceride levels, that did not follow a normal distribution were log-transformed.
To estimate the risk of dementia according to the FG VIM quartile, we conducted a Cox proportional hazards analysis with quartile 1 as the reference group. The risk is presented as hazard ratio (HR) and Bonferroni-adjusted 95% confidence interval (CI). Deceased individuals were identified by the Korean National Statistical Office. Follow-up was defined as the period from baseline to the first diagnosis of dementia, the date of death, or December 31, 2017.
We adjusted for several previously well-known metabolic factors: age, sex, BMI, smoking status, alcohol consumption, regular exercise, presence of chronic kidney disease, dyslipidemia, and hypertension; the lowest 20% income status; and hemoglobin levels in model 1. At least 5-year duration of diabetes, number of prescriptions for GLMs, mean FG levels during the 5-year variability assessment period, and presence of a depressive disorder were additionally adjusted for in model 2.
To investigate the influence of the cutoff value of VIM and the variability parameter, we stratified the participants according to the VIM decile, SD, CV, and ARV quartile and analyzed the risk of dementia using the previously described Cox regression analysis with decile 1 or quartile 1 as the reference group.
To explore the factors modifying the association between GV and the risk of dementia, we conducted interaction analyses after stratifying the participants according to several demographic factors and diabetes characteristics. Using the same adjustment strategy, we calculated HRs and 95% CIs of FG VIM quartile 4 compared with quartile 1–3 for dementia.
As competing death was prevalent and shared similar risk factors with dementia, we conducted a sensitivity analysis after excluding deceased individuals during the follow-up period using the same model.
To compare the association between a single FG concentration and the risk of dementia, we repeated the Cox regression analyses according to the five groups of baseline FG levels, with 100 to 119 mg/dL as the reference group. The mean FG level was excluded as a confounding factor in the analysis.
The variable inflation factor for all covariates was less than 2.0, indicating that there was no multicollinearity. Statistical analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA). Statistical significance was set at P<0.05.
RESULTS
As shown in Table 1, compared with the participants in FG VIM quartile 1, those in FG VIM quartile 4 were younger and included a higher proportion of men, current smokers, and heavy drinkers, with a lower proportion of comorbidities, except for chronic kidney disease.

Regarding the characteristics of diabetes, participants in FG VIM quartile 4 had a higher proportion of those receiving insulin treatment, taking at least two classes of GLM for 1 year before baseline, and duration of diabetes of at least 5 years.
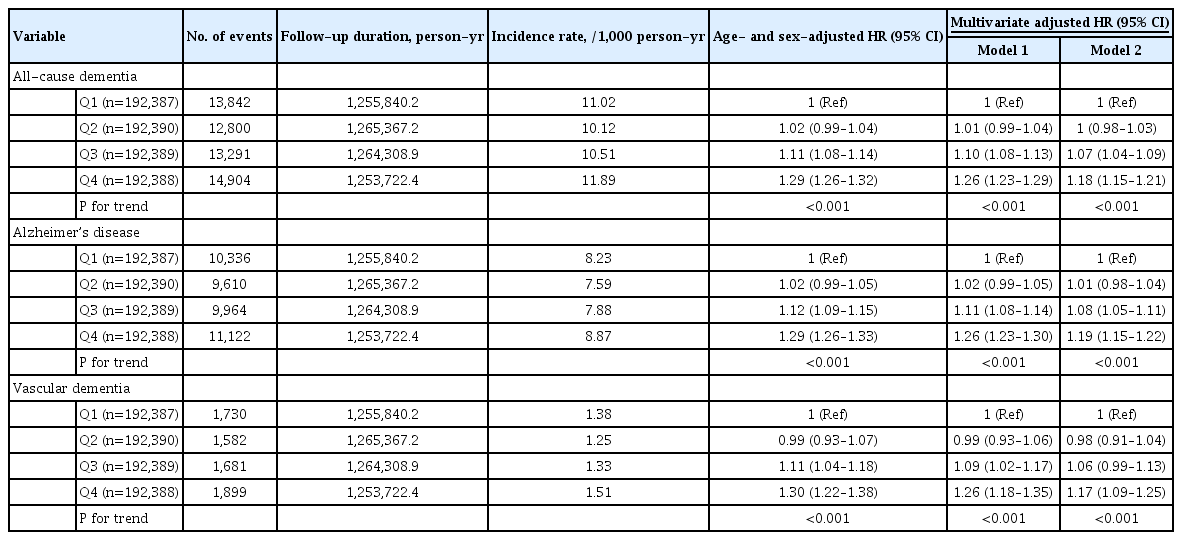
During 6.9 years (IQR, 6.3 to 7.4) of the follow-up period, a total of 54,837, 41,032, and 6,892 cases of all-cause dementia, AD, and VD were identified, respectively (Table 2). As the FG VIM quartile increased, the age-and sex-adjusted HRs for allcause dementia, AD, and VD also serially increased. In the fully adjusted model 2, the significance remained consistent. The HRs for all-cause dementia, AD, and VD of individuals in FG VIM quartile 4 compared to those in quartile 1 were 1.18 (95% CI, 1.15 to 1.21), 1.19 (95% CI, 1.15 to 1.22), and 1.17 (95% CI, 1.09 to 1.25), respectively. This finding did not change when the participants were divided into FG VIM deciles (Supplementary Table 1).
Quartiles of SD, CV, and ARV, instead of VIM, also showed a positive association between high GV and the risk of the three dementia outcomes (Supplementary Table 2).
In the subgroup analyses, a higher risk of all three outcomes of VIM quartile 4 compared with those of VIM quartiles 1–3 was found, regardless of the eligibility features, lifestyle habits, comorbidities, and diabetes-related characteristics (Tables 3 and 4). However, there was a significant interaction between FG VIM and the risk of all-cause dementia according to the presence or absence of obesity, dyslipidemia (Table 3), duration of diabetes, baseline FG levels, and prescription of metformin, sulfonylurea, thiazolidinedione, AGI, and insulin (Table 4). These interactions were partially observed during AD and VD development. In the sensitivity analysis after excluding 64,656 deceased participants, similar trends were observed (Supplementary Table 3).

Subgroup analysis according to clinically relevant factors in quartile 4 versus fasting glucose variability of quartiles 1–3

Subgroup analysis according to the characteristics of diabetes in quartile 4 versus fasting glucose variability of quartiles 1–3
Conversely, the relationship between the range of FG concentrations and the risk of the three dementia outcomes exhibited a U-shaped association (Supplementary Table 4). Considering individuals with FG levels of 100 to 119 mg/dL as the reference group, those with FG <100 or ≥180 mg/dL had a higher risk for all three outcomes.
DISCUSSION
Major findings of the present study
Using a Korean nationally representative database, this study clarified that FGV calculated over 5 years was positively related to the risk of all-cause dementia, AD, and VD among individuals with diabetes. Moreover, this significance was maintained regardless of previously well-known confounding factors and detailed characteristics of diabetes, including the mean FG. The impact of a higher GV was more prominent in patients with less favorable metabolic features of diabetes. Conversely, in the analysis using baseline FG levels, individuals in both the low and high FG groups had an increased risk of all three outcomes, representing a U-shaped association.
Fasting glucose variability and cognitive decline or dementia outcomes
Prior clinical and epidemiological studies have reported the impact of GV on cognitive impairment or dementia [12,21-23]. An analysis of young individuals aged 18 to 30 years without diabetes in the Coronary Artery Risk Development in Young Adults (CARDIA) study showed that higher intra-individual variability in FG was associated with worsening processing, memory, and language fluency 25 years after the baseline examination [21]. In a pooled analysis of two prospective studies including 6,237 participants, there was a significant relationship between HbA1c variability over 8 years and cognitive deficits among participants without diabetes, but this was not observed in participants with diabetes [23].
Another study conducted in individuals with diabetes showed that elevated 1,5-anhydroglucitol levels, a surrogate marker of glucose peaks [24], and postprandial glucose excursions could lead to a decline in cognitive function or risk of dementia [22]. Regarding FGV in diabetes, in an analysis of 16,706 participants of the Taiwan Diabetes Study, an independent significance between FG CV and HbA1c CV and the risk of AD in individuals with type 2 diabetes mellitus was found [12]. However, despite a long median follow-up period of 8.88 years and several confounding factors, the study outcome was confined to AD and not all-cause dementia. A recent publication analyzing 457,902 individuals with diabetes also showed that high and unstable HbA1c levels were associated with increased dementia risk using the UK Clinical Practice Research Datalink [13]. However, they only showed all-cause dementia incidence, they did not specify the incidence of AD and VD risks.
Nonetheless, in the present study, we included more than 700,000 eligible individuals with diabetes among almost all Koreans with diabetes and conducted a comprehensive assessment of dementia from all-cause, AD, and VD with various confounding factors at baseline and detailed subgroup analyses.
Interpretation for the anticipating effect of glucose variability on dementia
Multiple mechanisms may contribute to the relationship between GV and cognitive decline or the development of dementia [25]. Hyperglycemia, compensatory excessive insulin secretion, and enhanced peripheral or cerebral insulin resistance can cause inflammatory cytokine secretion in astrocytes, nitric oxide-mediated vasodilation, and attenuated neuronal survival [26]. Glucose oscillation is more related to neuronal dysfunction or oxidative stress than to constant high glucose concentrations in individuals with diabetes and in vitro studies [27,28]. Moreover, this might induce hyperphosphorylation of the microtubule-associated protein tau, which could disrupt neuronal function, a typical pathology of AD [29]. Recently, it is suggested that glucose excursion in individuals with diabetes may be responsible for changes in apolipoprotein A1 and complement C3 levels, which are AD-related proteins [30].
GLMs usage in individuals with diabetes could affect the natural course of GV, thereby weakening the association of GV with cognitive decline or dementia [23]. Previous studies have shown that insulin injection is associated with a 1.44-fold higher likelihood of dementia [5]. Conversely, the use of pioglitazone reduced the risk of dementia by 47% [10]. In the present study, subgroup analysis revealed that a prescription history of metformin, sulfonylurea, thiazolidinedione, AGI, and insulin was significantly associated with an increased risk of dementia. These findings should be interpreted cautiously rather than concluding that GLMs increase FGV. Considering that VIM quartile 4 consisted of a higher proportion of combination users of ≥2 GLMs, individuals with uncontrolled diabetes and high GV may be treated with various GLMs to reduce their blood glucose levels. If GLMs are not used for treatment, the association between GV and dementia would be stronger than the reported results. The above-mentioned drugs accounted for the top five GLM classes during 2008 to 2009, the period during which prescription history was estimated [31]. Future randomized controlled trials should compare the effects of GLMs on GVs.
In the present study, we should note that patients who were not obese and those with a longer duration of diabetes, higher blood glucose levels, GLM treatment, and dyslipidemia were more vulnerable to GV. These results were partially in line with those of previous research regarding GV and various outcomes showing the accentuated effect of GV in individuals with diabetes with uncontrolled glycemia [32,33]. The combination of GV and these confounders may have additive or synergistic effects on dementia development.
Throughout this study, the lower significance of VD outcomes than that of all-cause dementia or AD may be attributed to the low incidence rate of VD. Furthermore, despite the inclusion of type 1 diabetes mellitus in this study, the impact is expected to be minimal considering the low proportion of ICD-10 E10 codes (2.1%). Following sub-analysis according to ICD-10 codes, similar trends were noted throughout the three study outcomes without any interaction (Table 4).
There are no standardized methods for estimating glycemic variability. Although most previous studies adopted CV or SD, we selected VIM, which is independent of the mean value [17,34]. The CV and SD analyses were similar.
Conversely, when we investigated the association between FG levels and the risk of dementia, individuals with FG <100 mg/dL or FG ≥180 mg/dL had a higher risk of all-cause dementia, AD, and VD. A prior meta-analysis of 144 prospective studies also clarified a nonlinear dose-response association between hypoglycemia and hyperglycemia, presenting an increased risk for all-cause dementia, AD, and VD [5].
This is the first nationwide population-based study focusing on the predictive capacity of FGV on the risk of dementia from all-cause, AD, and VD in individuals with diabetes. Individuals with diabetes are vulnerable to dementia and cognitive impairment, which makes comprehensive self-care management difficult [10]; thus, it is essential to identify modifiable factors related to dementia.
We demonstrated the anticipating capacity of FGV for future dementia events even after adjusting for traditional diabetes-related factors; thus, reducing FGV can be a treatment target for diabetes for dementia prevention beyond lowering the average glucose levels. Measuring FG levels is easier and cheaper than measuring HbA1c levels; thus, this simple strategy for estimating FGV could help establish public health policies to identify and prioritize populations at high risk for dementia among individuals with diabetes; this strategy can in turn aid the active prevention of dementia.
Limitations of study
This study has several limitations. First, given that the definition of dementia is based on claims data from the NHIC, which lacks neuroimaging data and pathologic confirmation, incident dementia can be over-diagnosed. For improved accuracy of dementia diagnosis, we used information on prescription history for anti-dementia drugs, although the misclassification of patients with mild cognitive impairment (MCI) to AD patients persists. The incidence rate of all-cause dementia in the present study was 9.8 per 1,000 person-years, which is consistent with the rates reported in previous studies in Japan, China, and Europe [35-37], thus supporting the reliability of this study. In Korea, for reimbursement of the prescription of anti-dementia medications, there is a need for (1) Clinical Dementia Rating 1–3 or Global Deterioration Scale stage 3–7, and (2) Mini-Mental State Exam (MMSE) score ≤26, which suggests a low probability of misclassification of other neuropsychological diseases misdiagnosed as dementia [38]. This would be helpful in differentiating MCI/mild dementia patients from moderate to severe dementia patients to identify detailed prescription histories of anti-dementia medications in future studies. Second, we had no information about the educational status, familial history of dementia, psychiatric history, or apolipoprotein E4 phenotype, which are well-known risk factors for AD and VD [39,40]. Instead, we considered a history of depressive disorder from ICD-10 codes [5] and used the income level for socioeconomic status. Third, a reverse association is also possible. People with dementia are more likely to be diagnosed with diabetes than those without dementia [41], and patients with undiagnosed dementia due to the absence of clinical manifestations could be included in this study. To overcome this issue, we excluded the incidence of dementia within 1 year of baseline examination. Fourth, we could not adjust for changes in FG levels and/or prescriptions for GLMs in study participants during the follow-up period. Finally, we did not have any information on HbA1c levels. However, as HbA1c levels indicate the average glucose status [42], FG levels are more suitable for estimating GV than HbA1c levels. Similar results were found in other studies that used GV and HbA1c variability [12].
In conclusion, we illustrated the positive association between FGV over 5 years and the risk of dementia in this extensive nationwide population-based study. The highest quartile of FG VIM exhibited a 17% to 19% higher risk of all-cause dementia, AD, and VD than the lowest quartile, which was more pronounced among individuals with less favorable metabolic profiles. This phenomenon underscores the notion that GV management and glycemic control are essential to reduce the increasing prevalence of dementia in individuals with diabetes.
SUPPLEMENTARY MATERIALS
Supplementary materials related to this article can be found online at https://doi.org/10.4093/dmj.2021.0346.
HR and 95% CI for the incidence of dementia by deciles of variability independent of mean fasting glucosea
HR and 95% CI for dementia incidence by quartiles of fasting glucose variability were assessed by standard deviation, coefficient of variation, and average real variability
Results of the sensitivity analysis after excluding deceased participants
HR and 95% CI for the incidence of dementia by quartiles of baseline fasting glucose levels
Selection of study participants.
A representation of the study design.
Notes
CONFLICTS OF INTEREST
Ji A Seo has been associate editors of the Diabetes & Metabolism Journal since 2021. Hye Jin Yoo was been associate editors of the Diabetes & Metabolism Journal from 2020 to 2021. They were not involved in the review process of this article. Otherwise, there was no conflict of interest.
AUTHOR CONTRIBUTIONS
Conception or design: D.Y.L., J.K., S.Y.P., K.H., N.H.K.
Acquisition, analysis, or interpretation of data: D.Y.L., J.K., S.P., J.A.S., N.H.K., H.J.Y., K.H., N.H.K.
Drafting the work or revising: D.Y.L., J.K., S.Y.P., J.H.Y.
Final approval of the manuscript: S.G.K., K.M.C., S.H.B., K.H., N.H.K.
FUNDING
This research was supported by the Bio & Medical Technology Development Program of the National Research Foundation (NRF) funded by the Korean government (MSIT) (NRF-2019M3E5D3073102 and NRF-2019R1H1A2039682), a Korea University Grant (K1810951), the Basic Science Research Program through NRF funded by the Ministry of Education (NRF-2020R1I1A1A01071665), and a Korea University Ansan Hospital grant (O2000291). However, the funders did not participate in study design or reporting
Acknowledgements
None