Effect of Lactobacillus plantarum LMT1-48 on Body Fat in Overweight Subjects: A Randomized, Double-Blind, Placebo-Controlled Trial
Article information

Abstract
Background
We investigated whether Lactobacillus plantarum strain LMT1-48, isolated from Korean fermented foods and newborn feces, is a suitable probiotic supplement to treat overweight subjects.
Methods
In this randomized, double-blind, placebo-controlled clinical trial, 100 volunteers with a body mass index of 25 to 30 kg/m2 were assigned randomly (1:1) to receive 2×1010 colony forming units of LMT1-48 or to a placebo treatment group. Body composition was measured by dual-energy X-ray absorptiometry, and abdominal visceral fat area (VFA) and subcutaneous fat area were measured by computed tomography scanning. Changes in body fat, VFA, anthropometric parameters, and biomarkers were compared between the two treatment groups (ClinicalTrials.gov number: NCT03759743).
Results
After 12 weeks of treatment, the body weight decreased significantly from 76.6±9.4 to 75.7±9.2 kg in the LMT1-48 group but did not change in the placebo group (P=0.022 between groups). A similar pattern was found in abdominal VFA between the two groups (P=0.041). Serum insulin levels, the corresponding homeostasis model assessment of insulin resistance, and leptin levels decreased in the LMT1-48 group but increased in the placebo group (all P<0.05). Decrease in body weight and body mass index by treatment with LMT1-48 was correlated with increase in Lactobacillus levels significantly. LMT1-48 also increased Oscillibacter levels significantly, which were negatively correlated with triglyceride and alanine transaminase levels.
Conclusion
Administration of LMT1-48 decreased body weight, abdominal VFA, insulin resistance, and leptin levels in these subjects with overweight, suggesting its anti-obesogenic therapeutic potential.
INTRODUCTION
Obesity is defined as excessive fat accumulation and is a complex and chronic medical condition that increases the risk of other disorders, such as cardiovascular diseases, diabetes mellitus, and several types of cancers [1]. Obesity is becoming a worldwide public health problem, and globally 39% and 13% of adults were overweight and obese, respectively, in 2016 [2]. Although treatment of obesity starts with comprehensive lifestyle management including dietary, exercise, and behavioral modifications [3], pharmacological interventions are frequently required. However, newly developed anti-obesity medications should be used with caution as they have potential adverse effects; therefore, there is a need for safe and effective new therapies that can be used for treating obesity.
Among contributing factors for obesity, the gut microbiome has recently received considerable attention because it affects the processes of obtaining nutrients, energy regulation, and fat storage [4]. Thousands of different bacterial species live within the human gut, where they maintain a symbiotic relationship with the host and play a critical role in host metabolism [5]. By host–microbial cometabolism, polysaccharides are fermented to short-chain fatty acids and can be used as an energy source or bind to G protein-coupled receptors, which regulate hormones such as peptide YY and glucagon-like peptide-1 (GLP-1) [5]. Although mechanisms to explain the link between the changes in the gut microbiome and the development of obesity are still incomplete, various methods aiming to restore microbial dysbiosis and maintain intestinal homeostasis have been attempted as promising therapeutic alternatives to treat obesity. These include supplementation with prebiotics, probiotics, and/or synbiotics, and fecal microbial transplantation [6].
Probiotics are live microorganisms that can confer beneficial effects to the host [5]. Numerous studies have suggested that probiotic supplementation might help in modulating the composition as well as the activity of resident microbiota, thus counteracting obesity [7]. Many studies have suggested possible roles of probiotics in the treatment and prevention of obesity, such as increasing microbial diversity, inhibition of pathogenic bacterial growth, stimulation of short-chain fatty acid production, and appetite regulation [8]. Among the reported probiotics, most of the species with anti-obesity effects belong to the Lactobacillus and Bifidobacterium genera [9].
Lactobacillus is a genus of Gram-positive anaerobes normally present in the human gut, and several species, including L. acidophilus, L. curvatus, L. gasseri, L. rhamnosus, L. casei, L. amyhlovorus, L. sakei, and L. plantarum, have been suggested as alternative strategies to combat obesity [10,11]. Beyond the effects on body weight and fat mass, it has been reported that 2.4×109 colony forming units (CFUs) of L. species supplementation also showed additional weight loss effects when combined with bariatric surgery [12]. Among them, L. plantarum has received great attention as it is generally recognized as being safe for use in foods and has been employed widely for a long time [13].
The anti-obesity effects of probiotics are strictly strain-specific [7], and researchers continue to seek probiotic strains with stronger therapeutic activity [14]. We have isolated a novel L. plantarum strain (LMT1-48) from Korean fermented foods and newborn feces, and we reported its potent anti-obesity activities and underlying molecular mechanisms in vitro and in a high fat diet-induced mouse model of obesity [15,16]. Here, we investigated the efficacy and safety of LMT1-48 in human subjects with obesity.
METHODS
Study participants
One hundred seven healthy adult volunteers were screened for eligibility, with overweight defined as a body mass index (BMI) range of ≥25 to <30 kg/m2. Among them, 100 were included in this study after excluding seven according to our exclusion criteria: comorbidities of chronic disease (e.g., diabetes mellitus and cardiovascular diseases); consumption of products containing antibiotics or probiotics; use of medications that could affect body weight (e.g., anorexiants, antidepressants, beta-blockers, diuretics, hormonal contraceptives, and steroids); participation in a diet control program; and fluctuation of body weight over 10% within 3 months. All participants received an explanation of the procedures and possible risks associated with the study and provided written informed consent.
Study design
This was a double-blind, placebo-controlled, single-center, randomized controlled trial (RCT). It was conducted according to the Korean Good Clinical Practice guidelines and the Declaration of Helsinki 2013 (7th revision). Participants were randomly assigned to either LMT1-48 or placebo treatment groups in a 1:1 ratio using a dynamic allocation method with stratification by sex. Subjects were provided with individual screening codes for blinding. The experimental protocol was approved by the Institutional Review Board of Seoul National University Bundang Hospital (B-1805-469-004) and registered at www.clinicaltrials.gov (NCT03759743).
Intervention/procedures
The investigational products (LMT1-48) were given to the participants in the same packages provided by the probiotic manufacturer (Medytox Inc., Seoul, Korea). LMT1-48 capsules contained 10% of LMT1-48 and 90% of maltodextrin, and the placebo capsules contained 100% of maltodextrin. On the randomization visit, LMT1-48 or placebo capsules were distributed to the subjects, and they were asked to ingest two of them once daily for 12 weeks. Each LMT1-48 capsule contained 1×1010 CFU of LMT1-48. Compliance to the protocol was monitored strictly by counting leftover capsules on every visit.
From the start until the end of the study, participants were instructed to maintain a healthy lifestyle by adhering to published rules [17]. The daily calorie intake was calculated using CAN-Pro 5.0 software (KNS, Seoul, Korea) and the dietary intake information from 3 days—2 on weekdays and 1 at weekends—within a week before the visit.
Vital signs, anthropometric measurements, body fat, and abdominal adiposity were checked at weeks 0 (baseline), 6, and 12 (Supplementary Fig. 1). Dual-energy X-ray absorptiometry (Horizon W, Hologic Inc., Bedford, MA, USA) was used to measure whole body composition. Abdominal computed tomography scans (Somatom Sensation 16, Siemens, Munich, Germany) were used to measure the abdominal visceral fat area (VFA) and subcutaneous fat area (SFA). The abdominal total fat area (TFA) was calculated as the sum of the VFA and SFA.
Biochemical parameters, such as fasting levels of glucose (using a 747 Clinical Chemistry Analyzer, Hitachi, Tokyo, Japan), aspartate transaminase (AST) and alanine transaminase (ALT) (nicotinamide adenine dinucleotide hydrogen-ultraviolet [NADH-UV] method), alkaline phosphatase (AnaSpec, San Jose, CA, USA), creatinine (Jaffe’s kinetic method), blood urea nitrogen (Jaffe’s kinetic method), and lipid panel (747 Clinical Chemistry Analyzer), were measured at weeks 0 (baseline), 6, and 12.
Other biomarkers of obesity including the levels of gastric inhibitory polypeptide (GIP) and GLP-1 (ELISA, MilliporeSigma, Burlington, MA, USA), insulin (ECLIA, Linco, St. Charles, MO, USA), glucagon (Mercodia AB, Uppsala, Sweden), free fatty acids (747 Clinical Chemistry Analyzer), and high-sensitive C-reactive protein (CRP-Latex [II]X2, Denka Seiken Co., Tokyo, Japan) were measured from serum samples at baseline and after 12 weeks. Adiponectin (ELISA, Otsuka Pharmaceutical Co., Tokyo, Japan) and leptin (R&D Systems, Minneapolis, MN, USA) were measured from plasma samples.
Feces collection and gut microbiome analysis
Fecal samples were collected and frozen within 3 days of the visit date in a sterile stool collection kit provided by Macrogen (Seoul, South Korea). DNA from fecal samples was extracted using the DNeasy PowerSoil Kit (QIAGEN, Hilden, Germany) according to the manufacturer’s protocol, and the amount and quality were measured by PicoGreen (Promega, Madison, WI, USA) using VICTOR Nivo (PerkinElmer, Waltham, MA, USA). For 16S rDNA sequencing, fecal samples were prepared according to the Illumina 16S Metagenomic Sequencing Library Preparation protocols (Illumina, San Diego, CA, USA) as follows. The 16S rRNA genes were amplified from genomic DNA using 16S primers V3–V4. A subsequent limited‐cycle amplification step was performed to add multiplexing indices and Illumina sequencing adapters. The final products were normalized and pooled using PicoGreen. The sizes of libraries were verified using the TapeStation DNA screentape D1000 (Agilent Technologies, Santa Clara, CA, USA) and sequenced using the Illumina MiSeq platform.
Bioinformatics analysis
After sequencing was completed, MiSeq raw data were classified for each sample using the index sequence, and FASTQ files for each sample were generated. The adapter sequence was removed using the FASTP (v. 0.19.7) program [18], and error correction was performed on the region where the two reads overlapped. The paired-end data separated for each sample were assembled into a single sequence using FLASH (v. 1.2.11) [19]. The obtained sequence was clustered with more than 97% sequence similarity after removing low-quality sequences considered sequencing errors, ambiguous sequences, and chimera sequences, using CD HIT out, and an operational taxonomic unit (OTU) analysis program based on CD HIT EST [20]. This was used to form a species-level OTU. For the representative sequence of each OTU, BLAST+ (v. 2.9.0) [21] was performed on the reference DB (NCBI 16S Microbial), and taxonomic assignment was performed with the organism information of the subject with the highest similarity using QIIME (v. 1.9) [22,23]. To confirm the species diversity and homogeneity of the microbial community in the sample, the Shannon index was obtained, and alpha diversity information was confirmed via rarefaction curves and Chao1 values [23].
Statistical analysis
The sample size of 100 subjects ensured 90% power and a twosided type I error of 0.05 and an acceptable dropout rate of 15%. Efficacy analyses were performed on the full analysis set, defined as all randomized participants who received at least one dose of the study drug with follow-up body fat assessment as the primary outcome. The clinical variables and gut microbial features of continuous variables were analyzed with two-sample Student’s t-test or Wilcoxon’s rank-sum test. Safety endpoints included the rates of adverse and serious adverse events in those who received the study drug, and they were analyzed using chi-square or Fisher’s exact tests. The relationship between the clinical values and log-transformed microbiota counts after dietary supplementation was subjected to Spearman’s correlation analysis. P values for microbial data were adjusted using the Benjamini-Hochberg method for multiple comparisons.
Significance was defined as 2-sided P<0.05. All clinical and microbial statistical analyses were conducted using R software version 4.1.0 (R Development Core Team, Vienna, Austria) and RStudio version 1.4.1103 (RStudio, Boston, MA, USA).
RESULTS
Baseline characteristics
The 100 subjects were assigned randomly to LMT1-48 and placebo groups (Supplementary Fig. 2). One subject in the placebo declined study participation before receiving the trial product. During the study period, four subjects in the LMT1-48 group and 10 in the placebo group dropped out because of failed follow-up efficacy assessment, and finally 85 subjects (46 in the LMT1-48 group, and 39 in the placebo group) completed this RCT. Baseline characteristics of the subjects who received the study drug are summarized in Table 1. Middle-aged Korean subjects participated in this study with a BMI of 27.1±1.5 kg/m2 in the LMT1-48 group and 27.3±1.6 kg/m2 in the placebo group. There were no statistically significant differences between the two groups for all baseline parameters.
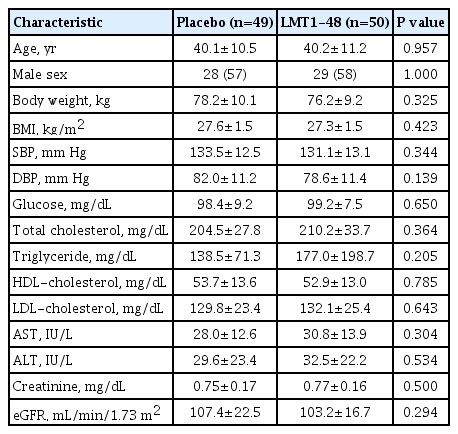
Baseline characteristics of the study participants
Effects of LMT1-48 ingestion on anthropometric and biochemical parameters
The changes in anthropometric parameters, including body weight, BMI, waist circumference, and other biochemical parameters, are shown in Table 2 and Fig. 1. The LMT1-48 group showed a significant weight loss from 76.6±9.4 kg at baseline to 75.7±9.2 kg at 12 weeks (P<0.05). BMI and waist circumference showed similar decreasing patterns in the LMI1-48 group.
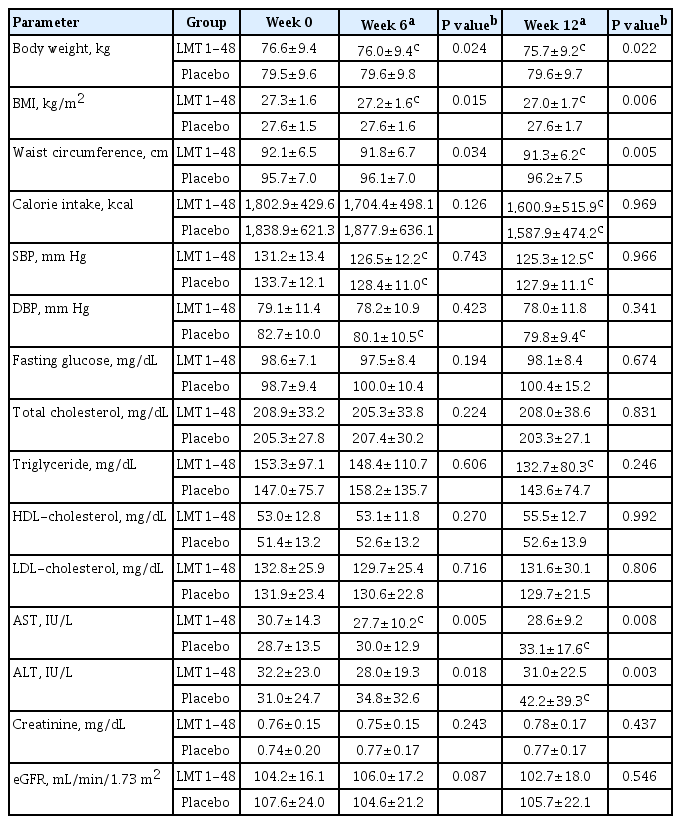
Effects of Lactobacillus plantarum strain LMT1-48 on anthropometric measures and blood biochemical profiles

Effects of LMT1-48 ingestion on body weight, body mass index (BMI), and abdominal adiposity. (A) Body weight, (B) BMI, (C) abdominal visceral fat area, and (D) abdominal subcutaneous fat area. Data are presented as the mean±standard error of the mean. LMT1-48, Lactobacillus plantarum LMT1-48. aP<0.05, bP<0.01.
The triglyceride (TG) levels decreased after 12 weeks ingestion of LMT1-48 (P<0.05), although there was no significant difference between the LMT1-48 and placebo groups. AST and ALT levels were significantly reduced in the LMT1-48 group compared with the placebo group (P<0.05). The levels of glucose and other lipid biomarkers, and renal function were not altered by LMT1-48 supplementation.
Effects of LMT1-48 ingestion on body fat
Changes in body weight, BMI, and abdominal fat area after 12 weeks ingestion of placebo or LMT1-48 are shown in Fig. 1. The abdominal VFA decreased significantly in the LMT1-48 group from 128.9±68.8 to 117±49.9 cm2 compared with the placebo group, where it increased from 149.8 ±60.9 to 151.9 ± 58.1 cm2 (P<0.05). LMT1-48 ingestion also significantly reduced the abdominal SFA from 236.4±53.7 to 229±53 cm2 compared with the placebo group, where it increased from 244.1±65.4 to 251.5±63.2 cm2 (P<0.05). The abdominal TFA exhibited a significant decrease by LMT1-48 supplementation from 365.3±78.4 to 346.0±72.8 cm2 compared with the placebo group, where it increased from 393.9±81.6 to 403.4±72.7 cm2 (P<0.05). In addition, decreases in VFA (-11.9 ± 48.5 cm2 vs. 2.1 ± 21.5 cm2), SFA (-7.4 ± 27.8 cm2 vs. 7.5 ± 31.7 cm2), and TFA (-19.3±48.5 cm2 vs. 9.6±43.7 cm2) in the LMT1-48 group was significantly greater than that in the placebo group (P<0.05, respectively). However, whole body fat mass did not change significantly in either group.
Effects of LMT1-48 ingestion on obesity-related cytokines and hormones
Changes in the levels of obesity-related biomarkers for the LMT1-48 group are shown in Table 3. The insulin level decreased in the LMT1-48 group, whereas it increased in the placebo group, with a significant between-group difference (P<0.05). The corresponding homeostasis model assessment of insulin resistance also showed a similar opposite trend in the two groups (P<0.05 for the between-group difference). Similarly, leptin levels decreased in the LMT1-48 group, whereas they tended to increase in the placebo group (P<0.05). Serum glucagon and plasma adiponectin levels increased in both groups, with no significant differences.
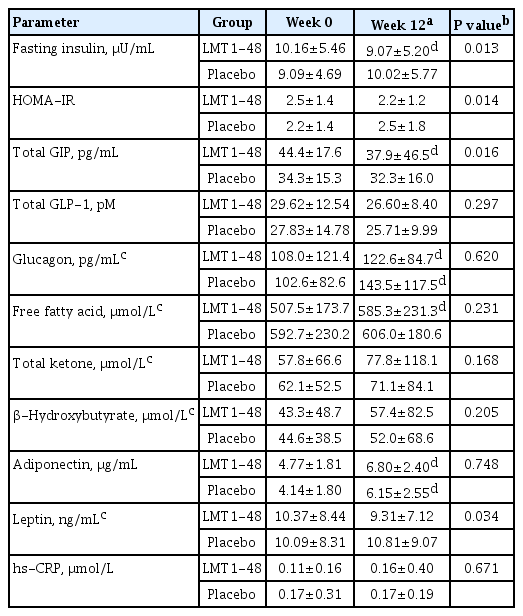
Effects of LMT1-48 on obesity-related biomarkers and hormones
Effects of LMT1-48 ingestion on gut microbiota
Gut microbial changes are shown in Fig. 2 and Supplementary Fig. 3. The Shannon index—microbiome α-diversity at the family level—increased significantly from 1.64 to 1.78 with LMT1-48 supplementation (P<0.05), indicating that it induced higher microbial richness and diversity. At the phylum level, administration of LMT1-48 for 12 weeks significantly increased the prevalence of Actinobacteria (by 0.23%) and Firmicutes (by 7.24%), but significantly decreased prevalence of the Bacteroidetes phylum (by 6.98%; P<0.05). The relative abundance ratio of Firmicutes to Bacteroidetes (F/B ratio) was 0.53 at baseline and increased to 0.80 after 12 weeks of ingestion of LMT1-48, with significant between-group difference (P<0.05). Other less prevalent phyla were not altered by LMT1-48 ingestion.

Changes of the logarithmic mean rarefied counts of gut microbiota (A) Lactobacillus and (B) Oscillibacter after 12-week supplementation with LMT1-48 or placebo, and (C) the heatmap of the Spearman correlation coefficients between microbes and obesity-related traits. LMT1-48, Lactobacillus plantarum LMT1-48; TG, triglyceride; ALT, alanine aminotransferase; AST, aspartate aminotransferase; HDL-C, high density lipoprotein cholesterol; BMI, body mass index; Bwt, body weight; VFA, visceral fat area; FM, fat mass; SFA, subcutaneous fat area; FFA, free fatty acid; TC, total cholesterol; LDL-C, low density lipoprotein cholesterol. aFalse discovery rate-adjusted P<0.05.
L. genus, which was negatively correlated with BMI (ρ=–0.15, P<0.05), body weight (ρ=–0.18, P<0.05), and body fat mass (ρ=–0.11, P<0.05), tended to increase after LMT1-48 supplementation, but not significantly because of high variation. Unfortunately, as too few L. plantarum counts were detected, this species was filtered out during the bioinformatics analysis. Instead, the abundance of L. sakei increased significantly in the LMT1-48 group compared with the placebo group (P<0.05). The abundance of L. sakei was negatively correlated with BMI (ρ=–0.16, P<0.05).
The Oscillibacter genus abundance was significantly increased after LMT1-48 administration for 12 weeks. This is reported to be associated with obesity [24] and was negatively correlated with the levels of TG (ρ=–0.27), ALT (ρ=–0.23), and high density lipoprotein (HDL) cholesterol (ρ 0.17; all P<0.05).
Both upper and lower levels of the taxonomic prevalence ranks of Oscillibacter genus, Oscillospiraceae family, and Oscillibacter ruminantium species were also significantly increased by LMT1-48 ingestion compared with placebo (P<0.05).
Safety assessment
No significant between-group differences were observed in terms of adverse event rates during 12-week study period; 12.0% (6/50 subjects, 10 events) in the LMT1-48 group and 4.1% (2/49 subjects, 4 events) in the placebo group (Supplementary Table 1). No serious adverse events were reported. In addition, there were no clinically significant abnormal measurements of vital signs in physical examinations in either group (data not shown).
DISCUSSION
In this RCT, 12-week dietary supplementation with LMT1-48 significantly reduced body weight, BMI, and waist circumference levels compared with the placebo group. The weight-reducing effect of LMT1-48 appeared first at week 6 and appeared to gradually decrease over time. In addition, abdominal VFA and SFA were also reduced significantly. Moreover, no serious adverse effects were observed in both groups during the test period. These findings indicate that LMT1-48 supplementation has a positive effect on reducing body weight and abdominal adiposity without safety concerns.
After LMT1-48 administration, body weight decreased to a modest yet significant extent. However, as abdominal obesity is more likely to be associated with other metabolic diseases [25], concurrent reductions in waist circumference and VFA in response to LMT1-48 ingestion could have clinical implications for improving the prognosis of persons with obesity.
LMT1-48 is a newly identified strain of L. plantarum that has shown anti-obesity effects in preclinical studies [15,16]. Administration of an LMT1-48 extract to 3T3-L1 adipocytes inhibited their differentiation and lipid accumulation by downregulating lipogenic genes including peroxisome proliferator-activated receptor gamma (PPARγ), CCAAT/enhancer binding protein (C/EBP), fatty acid synthase (FAS), and fatty acid binding protein 4 (FABP4) [16]. In an animal study with obese mice fed a high-fat diet, administration of LMT1-48 reduced body weight and fat volume [16]. Moreover, it decreased liver weight and liver TG levels along with downregulation of the lipogenic genes PPARγ, hormone-sensitive lipase (HSL), stearoyl-CoA desaturase-1 (SCD-1), and fatty acid translocase (FAT/CD36) in the liver.
Administration of such lactic acid-producing bacterial species has been reported to improve metabolic status, but the effects are relevant to specific strains, combinations, dosages, and the solvent used [10]. Administration of 5×1010 CFU L. reuteri NCIMB 30242 in a yogurt formulation to healthy hypercholesterolemic adults [26] and administration of 1×1010 CFU L. reuteri JBD301 have decreased body weights, similar to orlistat, an approved anti-obesity agent [27]. High leptin levels caused by leptin resistance and TG levels are important parameters linked to the severity of obesity [28,29]. In particular, TGs have been reported to inhibit the transport of leptin across the blood-brain barrier [29].
The gut microbiota is known collectively as a major causative factor for the progression of liver diseases, by changing bile acid homeostasis, the biology of amino acids and short-chain fatty acids, and energy expenditure [30]. Our finding of decreased liver enzyme levels by LMT1-48 supplementation implies that it might have a favorable effect on hepatic fat accumulation.
Both free fatty acids and adiponectin levels increased in the LMT1-48 group. Lipogenesis and free fatty acid levels have an inverse relationship in the rat liver [31]. Transient increases in the levels of free fatty acids that can be mobilized for oxidation have been shown after the administration of an SGLT2 inhibitor [32]. Therefore, the increased free fatty acid levels might be linked to a modulation of lipid metabolism, as observed in mouse models with changes in the expression of genes involved in lipogenesis and lipolysis following L. plantarum supplementation [16,33]. Adiponectin increases skeletal lipid uptake and oxidation [34] and is expected to aid in the elimination of free fatty acids safely without causing comorbid disease in the long term.
Among the serum biomarkers we tested, GIP levels were significantly decreased in the LMT1-48 group compared with the placebo group. Stimulation of adipogenesis and lipogenesis might act in GIP-induced obesity [35]. In healthy adults, inhibition of GIP by GIP(3–30)NH2 induced lipid metabolism by reducing adipocyte TG levels [36]. These findings support the idea that inhibition of GIP secretion might partially contribute to the LMT1-48-induced anti-obesogenic effects in human subjects with obesity. Furthermore, increased insulin secretion from pancreatic β-cells is a principal mechanism for GIP-induced obesity [37]. Taken together, the weight reduction effect of LMT1-48 might be mediated through the decreased levels of GIP and subsequent inhibition of insulin secretion. To our knowledge, our findings are the first to suggest that GIP might be involved in the anti-obesity effects of probiotics in humans. How LMT1-48 modulates GIP levels to alleviate obesity remains to be investigated.
Here we found that LMT1-48 supplementation significantly altered gut microbiota favorably. The decreased abundance of Actinobacteria species induced by LMT1-48 might be related to a decrease in body weight. In one study, Actinobacteria abundance was increased in obese compared with lean twin subjects [38]. As bacterial diversity in individuals with obesity is lower than in lean ones [39], the increased Shannon diversity index at the family level suggests a possible relationship between changes in the gut microbiome and the anti-obesity effect of LMT1-48.
The F/B ratio was increased by LMT1-48 supplementation. When probiotics are administered, the F/B ratio does not shift in a single direction, but rather returns to a normal balance [40]. In several experiments in mice involving LMT1-48, the F/B ratio was raised by administrating L. plantarum with the added advantage of anti-inflammatory effects [15,40]. The F/B ratio was over two in 747 Korean adults who were overweight or obese [41]. Given that the F/B ratio was 0.53 at baseline, it is reasonable to suppose that this increased ratio indicates recovery. So far, it is difficult to set a definite F/B ratio for controlling obesity because environmental factors have not been fully explored in earlier studies [42].
It is noteworthy that LMT1-48 supplementation significantly increased the abundance of O. ruminantium. This species was reported to decrease more in people with obesity than in lean subjects [43,44]. One study has shown an increase in the abundance of O. ruminantium by consuming foods fermented by L. plantarum [45]. Findings from other reports also propose the involvement of Oscillibacter-mediated mechanisms in weight loss. Butyric acid, a short-chain fatty acid that acts to increase energy expenditure and improve insulin sensitivity, is a major metabolic end product for O. ruminantium [46,47]. In addition, Oscillibacter exhibits dipeptidyl peptidase-4 (DPP-4) activity, an enzyme responsible for the degradation of incretins in the blood [48]. Although short-chain fatty acids were not analyzed in this RCT, it is possible that treatment with LMT1-48 induced weight loss in subjects with obesity by increasing the abundance of Oscillibacter species, followed by increased butyrate release and DPP-4-like enzyme activity.
During the 12 weeks of the study, there were no clinically serious adverse effects in either group of subjects. The compliance level in both groups was >95%, which supports the idea that LMT1-48, a lactic acid-producing bacterium isolated from Korean fermented foods and newborn feces, is safe.
In conclusion, this RCT has demonstrated the therapeutic potential of LMT1-48 in treating human obesity. In addition, our data regarding the gut microbiota are largely in agreement with other studies showing that the gut microbiota play key roles in human energy metabolism and the pathogenesis of obesity. They also support the idea that interventions to manipulate the gut microbiome with probiotics have a great therapeutic potential for alleviating obesity and obesity-related diseases.
SUPPLEMENTARY MATERIALS
Supplementary materials related to this article can be found online at https://doi.org/10.4093/dmj.2021.0370.
Summary of adverse events
Study design. This study was designed to include 2 weeks of initial screening and 12 weeks of ingestion. Dual-energy X-ray absorptiometry (DXA), abdominal computed tomography (CT) scan, fecal sample collection, blood collection, and anthropometrical measurement were performed as indicated. LMT1-48, Lactobacillus plantarum LMT1-48.
Flowchart showing the participants included in the study. In all, 107 subjects were screened for eligibility, and eight were excluded from randomization process. The remaining 99 subjects were randomized into LMT1-48 (50 subjects) and placebo (49 subjects) treatment groups. Four subjects from the LMT1-48 group and 10 from the placebo group dropped out because of missing efficacy and safety assessments. Finally, 46 subjects in the LMT1-48 group and 39 subjects in the placebo group were included in the analysis. LMT1-48, Lactobacillus plantarum LMT1-48.
Compositional profiling of (A) phyla and (B) genera with LMT1-48 or placebo supplementation during the study period. The genera profile shows the top 20. LMT1-48, Lactobacillus plantarum LMT1-48.
Notes
CONFLICTS OF INTEREST
Woo Shun Lee and Tai Hoon Kim are employees of Medytox (Suwon, South Korea).
AUTHOR CONTRIBUTIONS
Conception or design: M.S., H.J., W.S.L., T.H.K., S.L.
Acquisition, analysis, or interpretation of data: M.S., H.J., W.S.L., T.H.K., S.L.
Drafting the work or revising: M.S., H.J., W.S.L., T.H.K., S.L.
Final approval of the manuscript: M.S., H.J., W.S.L., T.H.K., S.L.
FUNDING
This research was funded by Medytox (Suwon, South Korea) through a subcontract with Seoul National University Bundang Hospital (Seongnam, South Korea).
Acknowledgements
None