The Effect of DPP-4 Inhibitors on Metabolic Parameters in Patients with Type 2 Diabetes
Article information
Abstract
Background
We evaluated the effects of two dipeptidyl peptidase-4 (DPP-4) inhibitors, sitagliptin and vildagliptin, on metabolic parameters in patients with type 2 diabetes mellitus.
Methods
A total of 170 type 2 diabetes patients treated with sitagliptin or vildagliptin for more than 24 weeks were selected. The patients were separated into two groups, sitagliptin (100 mg once daily, n=93) and vildagliptin (50 mg twice daily, n=77). We compared the effect of each DPP-4 inhibitor on metabolic parameters, including the fasting plasma glucose (FPG), postprandial glucose (PPG), glycated hemoglobin (HbA1c), and glycated albumin (GA) levels, and lipid parameters at baseline and after 24 weeks of treatment.
Results
The HbA1c, FPG, and GA levels were similar between the two groups at baseline, but the sitagliptin group displayed a higher PPG level (P=0.03). After 24 weeks of treatment, all of the glucose-related parameters were significantly decreased in both groups (P=0.001). The levels of total cholesterol and triglycerides were only reduced in the vildagliptin group (P=0.001), although the sitagliptin group received a larger quantity of statins than the vildagliptin group (P=0.002).The mean change in the glucose- and lipid-related parameters after 24 weeks of treatment were not significantly different between the two groups (P=not significant). Neither sitagliptin nor vildagliptin treatment was associated with a reduction in the high sensitive C-reactive protein level (P=0.714).
Conclusion
Vildagliptin and sitagliptin exert a similar effect on metabolic parameters, but vildagliptin exerts a more potent beneficial effect on lipid parameters.
INTRODUCTION
The increasing prevalence of diabetes mellitus is increasing the economic burden of controlling blood glucose levels and treating complications [1,2]. Diabetes mellitus patients also exhibit a more than 3-fold greater risk of cardiovascular disease (CVD) and mortality than nondiabetic subjects [3]. To prevent CVD, patients with diabetes mellitus require comprehensive treatment that includes the control of glucose, blood pressure and cholesterol levels. The UK Prospective Diabetes Study demonstrated that intensive glucose control of type 2 diabetes could prevent microvascular complications [4]. However, large follow-up clinical studies revealed that intensive treatment increases the risk of CVD and mortality due to hypoglycemia and weight gain [5,6,7]. Therefore, a variety of potential drugs have been developed to control the glucose levels and reduce severe hypoglycemia. Among these drugs, dipeptidyl peptidase-4 (DPP-4) inhibitors have been proven effective for glucose control without inducing hypoglycemia and are widely used as the primary therapeutic option. Sitagliptin is the first DDP-4 inhibitor that was commercially approved for use. Many clinical trials demonstrated that sitagliptin reduces the level of glycated hemoglobin (HbA1c) by 0.6% to 1.5% compared to placebo in subjects of various ages and ethnicities [8,9,10]. Vildagliptin, the second DPP-4 inhibitor developed, also effectively reduces the plasma glucose levels [11,12]. Although both sitagliptin and vildagliptin belong to the same class of DPP-4 inhibitors, these two drugs display many different properties, including structure, pharmacokinetics and mechanism of action to inhibit DPP-4 [13,14,15]. Sitagliptin is a 523.32 Da compound that contains a pyrimidine structure and displays a 12.4-hour half-life. It is primarily metabolized by cytochrome p450 3A4 and eliminated by renal excretion [13]. Alternatively, vildagliptin is a 303 Da compound that contains a cyanopyridine structure and displays a 2-hour half-life. Because of its low protein binding affinity (9%), vildagliptin is rapidly absorbed, reaching its peak plasma concentration within 1 hour, and then rapidly eliminated [14]. However, despite its short half-life, vildagliptin exerts a potent inhibitory effect for 24 hours by covalently binding to the DPP-4 receptor if administered at a dose of 50 mg twice daily [15,16]. Generally, the effect of both drugs on the plasma glucose level and the glucose indices is similar. Vildagliptin exerts a more potent beneficial effect on the levels of oxidative stress and inflammation markers [17,18]. However, few patients were examined for only a short duration, so the long-term effects of both drugs on metabolic parameters have not been well studied.
This study investigated the effects of two DPP-4 inhibitors, sitagliptin and vildagliptin, on metabolic parameters in patients with type 2 diabetes mellitus.
METHODS
This retrospective study reviewed patients who had been diagnosed with type 2 diabetes mellitus from January 2008 to December 2012 at Severance Hospital Diabetes Center. Patients who were receiving 100 mg of sitagliptin once daily or 50 mg of vildagliptin twice daily were selected and the dosage of each patient's previous medications was maintained. The exclusion criteria were as follows: 1) any change in prior medications just before (the past 12 weeks) or during the period of DPP-4 inhibitor treatment, including any alteration in dose, composition, or frequency; 2) chronic liver (Child-Pugh C) or kidney disease (stage ≥IV); or 3) any medications that could affect the plasma glucose levels, such as a steroid, thyroid hormone, or herbal drug. The enrolled patients were separated into the sitagliptin group or the vildagliptin group according the drug that they were receiving. The metabolic parameters, including the levels of fasting plasma glucose (FPG), postprandial 2-hour glucose (PPG), HbA1c, glycated albumin (GA), total cholesterol, high density lipoprotein cholesterol (HDL-C), low density lipoprotein cholesterol (LDL-C), triglyceride (TG), and creatinine, were measured at baseline and every 12 weeks during the 24-week study. The high sensitivity C-reactive protein (hsCRP) assay was also performed. The prevalence of hypertension, coronary artery occlusive disease (CAOD), peripheral artery occlusive disease (PAOD) and stroke and the medical history of statin administration were recorded using the medical records. The FPG levels were determined via the standard glucose oxidase method using a 747 automatic analyzer (Hitachi, Tokyo, Japan). The HbA1c levels were measured via high performance liquid chromatography. The serum GA level was determined via an enzymatic method using an albumin-specific proteinase, ketoamine oxidase, and albumin assay reagent (LUCICA GA-L; Asahi Kasei Pharma Co., Tokyo, Japan), as well as a Hitachi 7699 Pmodule autoanalyzer (Hitachi Instruments Service, Tokyo, Japan). The fasting and postprandial 2-hour insulin and C-peptide levels were measured via a radioimmunoassay method at baseline. To analyze insulin resistance and insulin secretion, homeostatic model assessment-insulin resistance (HOMA-IR) and the change in the C-peptide level were calculated as follows: HOMA-IR=fasting insulin (µU/mL)×FPG (mmol/L)/22.5, and ΔC-peptide=postprandial 2-hour C-peptide.fasting C-peptide. The body mass index (BMI) was also calculated according to the following equation: BMI=weight (kg)/height2 (m2). The mean change (Δ) in each metabolic parameter was calculated using following formula: level after 24 weeks of treatment.level at baseline.
Statistical analysis
All descriptive data were expressed as the means±standard deviation. Continuous variables of the sitagliptin group and the vildagliptin group were compared and analyzed using t-tests. Nominal variables were compared using the chi-square test. Analyses of more than three measured parameters were performed using repeated measures analysis of variance. P values of less than 0.05 were considered to be statistically significant. Pearson correlation coefficient (r) was used to assess the strength of the relationships between the clinical and laboratory variables. Variables displaying P<0.05 based on univariate analysis were subjected to multivariate analysis. SPSS version 17.0 (SPSS Inc., Chicago, IL, USA) was used for the analyses.
RESULTS
Baseline characteristics
A total of 170 patients suffering from type 2 diabetes mellitus who had received sitagliptin or vildagliptin for more than 24 weeks were selected. Ninety-three patients were taking sitagliptin, and 77 patients were taking vildagliptin. The baseline characteristics of both groups are presented in Table 1. The mean age of the subjects was 61.3±12.9 years in the sitagliptin group and 58.7±12.2 years in the vildagliptin group (P=0.186). The diabetes mellitus duration was over 6 years in both groups (P=0.642). There was no difference in the metabolic parameters of the FPG, HbA1c, GA, creatinine, estimated glomerular filtration rate, TG or total, and LDL-C or HDL-C level at baseline. However, the PPG level was significantly higher in the sitagliptin group than in the vildagliptin group (P=0.030). Although HOMA-IR was not different between the groups (P=0.480), the postprandial 2-hour C-peptide level and the change in the C-peptide level were significantly higher in the subjects taking vildagliptin than in those taking sitagliptin (P=0.030). There was no significant difference in the prevalence of hypertension, CAOD, PAOD, or stroke (P=not significant) between the groups. Statins were more frequently administered in the sitagliptin group than in the vildagliptin group (P=0.002).
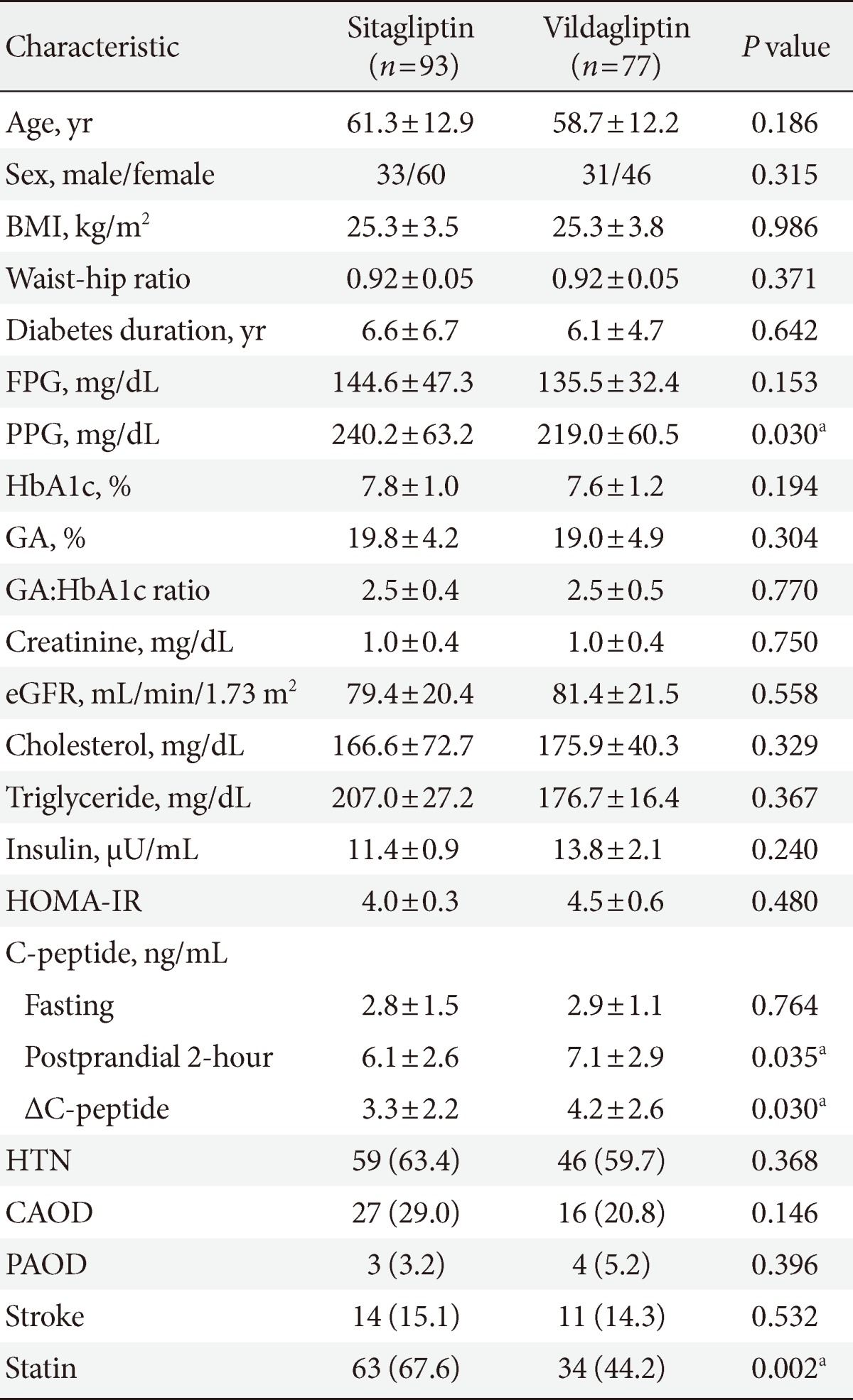
Baseline characteristics of the patients
Change in the metabolic parameters after 24 weeks of treatment
After 24 weeks of DPP-4 inhibitor treatment, all of the glucose parameters were significantly decreased compared to baseline in both groups (Table 2). The HbA1c and GA levels were significantly decreased compared to the premedication levels (Fig. 1A and B). The ratio of GA to HbA1c was significantly reduced from 2.5 to 2.3 (P=0.001). There were changes in both the FPG and PPG levels (Fig. 1C and D). However, there was no significant difference between the groups in the magnitude of the change in the glucose parameters (Table 2). The total cholesterol and TG levels were significantly decreased in the vildagliptin group (P=0.001) (Fig. 1E and F) regardless of statin use (Supplementary Table 1). The LDL-C level was also reduced, although this result was not statistically significant (P=0.077). There was no significant change in the lipid parameters in the sitagliptin group (Table 2). Although the mean changes in the lipid parameters were not significantly different between the two groups, vildagliptin displayed a trend to reduce the total cholesterol levels further than sitagliptin (P=0.071). The hsCRP level was 1.9±1.2 mg/L in the sitagliptin group and 1.5±1.4 mg/L in the vildagliptin group at baseline. There was no statistical significance difference in the hsCRP level after DPP-4 inhibitor treatment.

Drug effects on metabolic parameters after 24 weeks of treatment
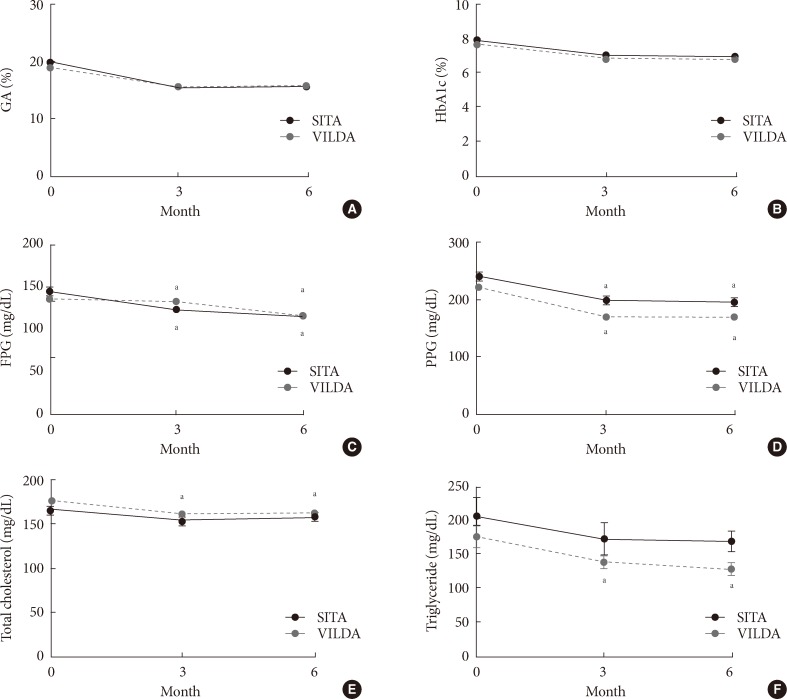
(A-F) Change in the metabolic parameters during dipeptidyl peptidase-4 (DPP-4) inhibitor treatment. Values are presented as mean±standard error. SITA, sitagliptin; VILDA, vildagliptin; GA, glycated albumin; HbA1c, glycated hemoglobin; FPG, fasting plasma glucose; PPG, postprandial glucose. aP<0.05, compared to baseline.
Proportion of subjects that reached the treatment target goal
A decrease in the HbA1c level of over 1% from baseline was achieved in 39.8% of the patients administered sitagliptin and 36.4% of the patients administered vildagliptin (P=0.746) (Fig. 2A). The proportion of patients exhibiting an HbA1c level of less than 7% was 73% in the sitagliptin group and 79.5% in the vildagliptin group (P=0.362) (Fig. 2B). There was no significant difference between the two groups in terms of glucose control. The proportion of patients who achieved a reduction in the GA level of over 3% from baseline was 63.6% in the sitagliptin group and 50.8% in the vildagliptin group (P=0.136) (Fig. 2C). The proportion of patients displaying a GA level of less than 14% was 37% in the sitagliptin group and 35% in the vildagliptin group (P=0.406) (Fig. 2D).
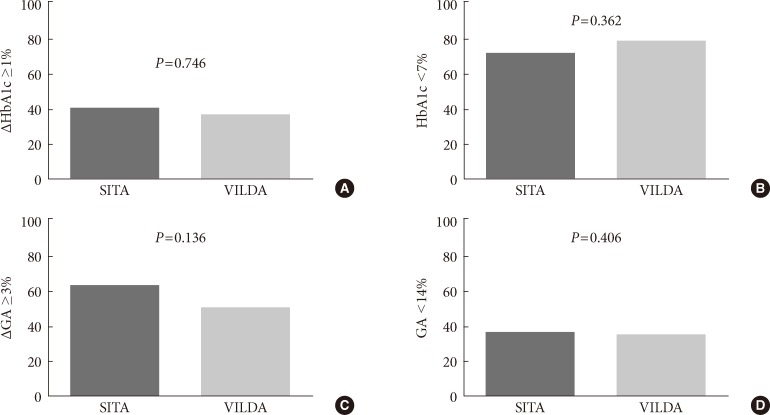
(A-D) Proportion of subjects that reached the target glucose range. Student t-test was performed. SITA, sitagliptin; VILDA, vildagliptin; HbA1c, glycated hemoglobin; ΔHbA1c ≥1, greater than 1% decrease in the HbA1c level from baseline; GA, glycated albumin; ΔGA ≥3, greater than 3% decrease in the GA level from baseline.
DISCUSSION
This study compared the effects of sitagliptin and vildagliptin on metabolic parameters. The efficacy of sitagliptin and vildagliptin were directly compared based on various glucose and lipid parameters over the course of 24 weeks of treatment. We found that vildagliptin exerts a similar effect on glucose control to that of sitagliptin, but vildagliptin exerts more potent beneficial effect on the lipid profiles. The metabolic parameters could be easily and consistently measured in most outpatient clinics. There were no significant differences in the changes in the glucose parameters. Additionally, a similar proportion of the enrolled patients attained the target glucose range after treatment with the DPP-4 inhibitor in both medication groups. Significant changes in the lipid parameters following sitagliptin treatment were not detected. However, with vildagliptin treatment, the total cholesterol and TG levels were significantly decreased compared to baseline, although the vildagliptin group received a lower amount of statin drug compared to the sitagliptin group.
There are many studies that investigated the clinical efficacy of DPP-4 inhibitors [19,20,21,22,23,24]. Many studies reported an improvement in the glucose status compared to placebo when administered as a supplement to the existing treatment or as a combination therapy with various drugs, including metformin, sulfonylurea, thiazolidinedione, or insulin, in patients suffering from type 2 diabetes mellitus with impaired glucose control. In addition, the clinical parameters that could affect glycemic control were evaluated [10,25,26]. In this study, the GA level was used to evaluate the change in glucose metabolism over the course of 2 to 3 weeks as an of index short-duration glucose control [27]. The GA level is currently widely used as an index of glycemic control during intensive diabetes treatment as a more rapid glycation index than HbA1c for glucose control and excursion [27,28,29]. In many studies, both drugs exerted a similar effect on glucose reduction compared to placebo, but some studies reported that vildagliptin may exert a more potent effect to reduce of oxidative stress and glucose fluctuations, which may play a role in its protection against vascular damage [17,30,31]. Recently, a prospective randomized control trial reported that sitagliptin and vildagliptin treatment resulted in a reduction in the carotid artery intra media thickness (IMT) by decreasing the oxidative stress and inflammation marker levels [18]. In that study, there was no significant change in the lipid parameters and no difference between the two groups in the reduction in the glucose parameters over the course of 12 weeks of treatment. However, vildagliptin induced a stronger reduction in the IMT than sitagliptin. Predictors of the IMT change were only found for glucose fluctuations, measured as the mean amplitude of glucose excursion and the LDL levels. In our study, there was no difference in the change in the glucose parameters, including the GA level and the GA to HbA1c ratio. However, there was a significant reduction in the lipid parameters in the vildagliptin group. Some studies reported this effect of DPP-4 inhibitor treatment on the lipid parameters [17,26,32,33] and found an association between DPP-4 inhibitor treatment and reduced total cholesterol levels. We investigated the change in lipid parameters during a 24-week DPP-4 inhibitor treatment period and compared the efficacy of the two drugs. Although there was no significant difference in the magnitude of the mean change between the two groups, vildagliptin treatment resulted in significantly reduced levels of total cholesterol and TG.
This study has some limitations. Because it was not a randomized clinical trial, there were biochemical differences between the two groups at baseline. We could not exclude the possibility of differences in drug compliance between the two medications. The number of enrolled patients was relatively small because there were few subjects who had not changed other oral hypoglycemic medications. Although we continuously followed up for up to 24 weeks, we did not detect a direct effect of either drug on the development of CVD. Therefore, long-term follow-up studies of diabetes using DPP-4 inhibitors are needed to obtain additional evidence of their benefits.
In conclusion, vildagliptin exerts a similar effect on metabolic profiles to that of sitagliptin, but vildagliptin exerts a more potent beneficial effect on lipid profiles.
ACKNOWLEDGMENTS
This study was financially supported by the "Kiturami" Faculty Research Assistance Program of Yonsei University College of Medicine (6-2012-0148).
Notes
No potential conflict of interest relevant to this article was reported.
References
Supplementary Material
Supplementary Table 1
Lipid profile changes according to statin treatment