- Current
- Browse
- Collections
-
For contributors
- For Authors
- Instructions to authors
- Article processing charge
- e-submission
- For Reviewers
- Instructions for reviewers
- How to become a reviewer
- Best reviewers
- For Readers
- Readership
- Subscription
- Permission guidelines
- About
- Editorial policy
Articles
- Page Path
- HOME > Diabetes Metab J > Volume 35(1); 2011 > Article
-
Original ArticleAutoimmune Hypoglycemia in a Patient with Characterization of Insulin Receptor Autoantibodies
- Suk Chon1,2, Moon Chan Choi1, Yun Jung Lee1, You Cheol Hwang1,2, In-Kyung Jeong1,2, Seungjoon Oh1,2, Kyu Jeung Ahn1,2, Ho Yeon Chung1,2, Jeong-Taek Woo1,2, Sung-Woon Kim1,2, Jin-Woo Kim1,2, Young Seol Kim1,2
-
Diabetes & Metabolism Journal 2011;35(1):80-85.
DOI: https://doi.org/10.4093/dmj.2011.35.1.80
Published online: February 28, 2011
1Department of Endocrinology and Metabolism, Kyung Hee University School of Medicine, Seoul, Korea.
2Research Institute of Endocrinology, Kyung Hee University School of Medicine, Seoul, Korea.
- Corresponding author: Seungjoon Oh. Department of Endocrinology and Metabolism, Kyung Hee Medical Center, 1 Heogi-dong, Dongdaemun-gu, Seoul 130-702, Korea. orqwic@chol.com
- *Suk Chon and Moon Chan Choi jointly contributed to this paper as first authors.
• Received: August 10, 2010 • Accepted: November 24, 2010
Copyright © 2011 Korean Diabetes Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Background
- Type B insulin resistance syndrome is a manifestation of autoantibodies to the insulin receptor that results in severe hyperglycemia and acanthosis nigricans. However, the mechanisms by which these autoantibodies induce hypoglycemia are largely unknown. In this paper, we report the case of patient with type B insulin resistance syndrome who presented with frequent severe fasting hypoglycemia and acanthosis nigricans.
-
Methods
- To evaluate the mechanism of hypoglycemia, we measured the inhibition of insulin binding to erythrocytes and IM9 lymphocytes in a sample of the patient's dialyzed serum before and after immunosuppressive therapy.
-
Results
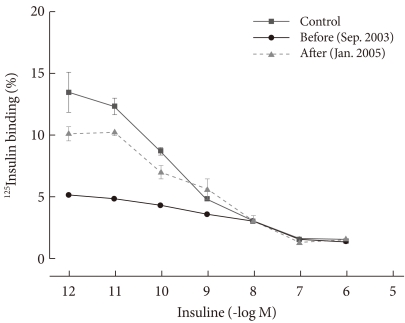
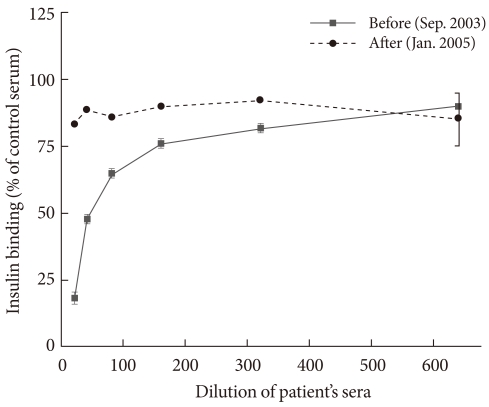
- In the patient's pre-treatment serum IgG, the binding of 125I-insulin to erythrocytes was markedly inhibited in a dose-dependent manner until the cold insulin level reached 10-9 mol/L. We also observed dose-dependent inhibition of insulin binding to IM9 lymphocytes, which reached approximately 82% inhibition and persisted even when diluted 1:20. After treatment with glucocorticoids, insulin-erythrocyte binding activity returned to between 70% and 80% of normal, while the inhibition of insulin-lymphocyte binding was reduced by 17%.
-
Conclusion
- We treated a patient with type B insulin resistance syndrome showing recurrent fasting hypoglycemia with steroids and azathioprine. We characterized the patient's insulin receptor antibodies by measuring the inhibition of insulin binding.
- Autoimmune hypoglycemia is a very rare disease caused by autoantibodies to the insulin receptor or to insulin itself [1]. Insulin antibody-mediated hypoglycemia is more common in autoimmune hypoglycemia [2]. Type B insulin resistance syndrome is a rare disorder characterized by severe hyperglycemia and acanthosis nigricans in which autoantibodies to the insulin receptor are present in serum [3]. On review of the literature, there are few cases of spontaneous fasting hypoglycemia reported, which is difficult to distinguish from other causes of hypoglycemia such as insulinoma [4,5]. Insulin receptor antibodies may cause hyperglycemia and/or hypoglycemia, and have been studied in vitro [3,6]. However, the rarity of insulin receptor antibody-mediated hypoglycemia has prevented extensive research into its mechanism.
- Recently, we experienced a case of male patient with frequent, severe fasting hypoglycemia and acanthosis nigricans. He had no significant medical history and no history of autoimmune disease. Laboratory evaluation revealed the presence of insulin receptor antibodies in his serum. We treated him with glucocorticoids and azathioprine. In order to evaluate the mechanism of insulin receptor antibody-induced hypoglycemia, we analyzed the behavior of antibodies in his serum.
INTRODUCTION
- Case history
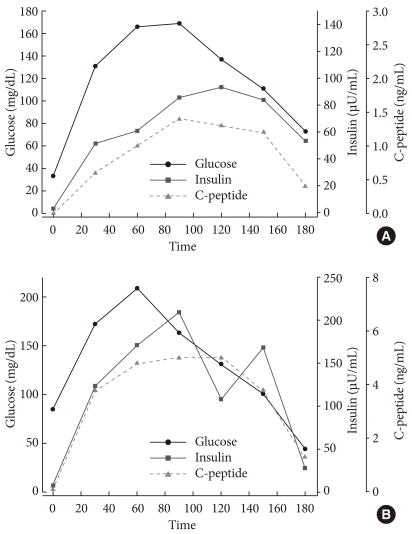
- A 35-year-old man presented with severe, episodic fasting hypoglycemia for the past several months as evidenced by sweating, anxiety, and episodes of unconsciousness. He had gained 12 kg over the past 6 months. His medical history was unremarkable. Physical exam revealed extensive acanthosis nigricans on his posterior neck, axillary, and inguinal areas (Fig. 1). We confirmed the diagnosis of fasting hypoglycemia with an attempted 72-hour fasting test (Fig. 2). At 4 hour after fasting, he complained of hypoglycemic symptoms and his blood glucose level was 44 mg/dL, plasma insulin level was 19.8 µU/mL, plasma proinsulin level was 14.11 pmol/L, and C-peptide was undetectable. The test was terminated after 9 hours due to severe hypoglycemia: his blood glucose level was 38 mg/dL. Despite worsening hypoglycemia, his insulin level slowly decreased and his C-peptide level remained undetectable. We performed computed tomography to exclude the possibility of insulinoma and found no evidence of a pancreatic mass. Percutaneous transhepatic portal and splenic venous sampling did not show abnormally elevated insulin or C-peptide levels. The patient had a normal adrenal response to a rapid ACTH stimulation test and normal thyroid function tests. We performed a 75 g oral glucose tolerance test to evaluate his insulin secretory capacity. Glucose excursion was normal, but insulin and C-peptide secretion increased in a delayed pattern and remained consistently elevated despite a normal glucose level (Fig. 3A).
- We analyzed the patient's serum for autoantibodies to evaluate for associated autoimmune diseases. Serologic exam was unremarkable: tests were negative for rheumatoid factor, antinuclear antibodies, anti-ds DNA antibodies, and anti-thyroid antibodies. Serum immunoglobulin levels (G, A, M, and E) were also within normal limits. Although the level of insulin antibodies was 6.7% (reference range, 0-7%), the insulin receptor antibody was positive by radioreceptor assay.
- We obtained written informed consent from the patient and the study protocol was approved by the Institutional Review Board of Kyung Hee University.
- Methods
- We dialyzed the patient's serum through a membrane that excluded molecules less than 50,000 MW. The complements in serum were heat-inactivated at 56℃ for 30 minutes and then run the dialyzed serum through a protein A affinity column (Hi-Trap affinity column). After washing with 10 mL PBS, the bound IgG was eluted with 3 mL of 100 mM sodium citrate (pH 3.5). We dialyzed the samples again and determined immunoglobulin concentrations.
- Insulin binding was determined as previously reported [7,8] on freshly isolated erythrocytes drawn under fasting conditions and purified on cellulose columns. Results are expressed as the percent specific binding for an erythrocyte suspension containing 4×106 RBC/µL.
- To determine the insulin-erythrocyte binding activity, we performed binding studies using a radioreceptor assay.
- We determined the extent of erythrocyte binding to 125I-labeled insulin by incubating a 400-µL cell suspension (1.75×106 cells in buffer G), 20 pg of 125I-labeled insulin in 25 µL of buffer, and various amounts of unlabeled insulin (0 to 0.5×105 ng) in a total volume of 0.5 mL. After incubation at 15℃ for 3 hours, we placed 200 µL aliquots of the suspension into prechilled microfuge tubes containing 200 µL buffer G and 200 µL dibutyl phthalate and centrifuged them for 10 minutes in a Beckman Microfuge B (Beckman Instruments Inc., Fullerton, CA, USA). We determined the radioactivity of the cells by gamma counter.
- We also investigated the insulin receptor binding activity of human lymphocytes, which carry insulin receptors that reflect insulin sensitivity. We pre-incubated 7.5×106 IM9 cells with serial dilutions of patient serum or control serum at 37℃ for 30 minutes in 800 µL assay buffer (100 mM HEPES, 120 mM NaCl, 1.2 mM MgSO4, 2.4 mM KCl, 1 mM glucose, 1 mM EDTA, 1% bovine serum albumin, pH 7.8). Cells were washed with phosphate-buffered saline and incubated with 125I-insulin in a final volume of 500 µL assay buffer at 15℃. At the end of the 90-minute incubation period, we centrifuged cells and separated cell-associated radioactivity from free 125I-insulin by adding 200 µL dibutylphthalate [3].
METHODS
Preparation of the serum IgG fraction
Insulin binding of erythrocytes
Binding studies
Inhibition of insulin binding of human IM9 lymphocytes
- Clinical course
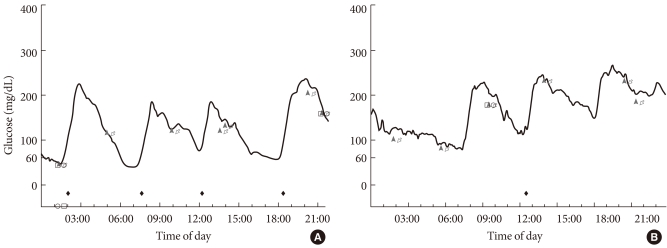
- Following the laboratory investigation, we diagnosed the patient with autoimmune hypoglycemia caused by insulin receptor antibodies and treated him with two courses of plasmapheresis. The patient's symptoms did not improve (Fig. 4A), so we added immunosuppressive agents. We first treated the patient with prednisolone 80 mg/day, which we eventually tapered to 20 mg/day 11 months after admission. The patient experienced no hypoglycemia attack during prednisolone treatment (Fig. 4B), although he suffered from mild recurrent hypoglycemia and skin inflammation at doses less than 20 mg/day. As a steroid-sparing agent, we added the azathioprine 100 mg/day to a physiologic prednisolone dose of 7.5 mg/day. The patient experienced no hypoglycemia during the 6 months of azathioprine treatment, and his skin inflammation and acanthosis nigricans improved.
- We performed a 75 g glucose tolerance test 16 months after admission to measure glucose, insulin, and C-peptide levels (Fig. 3B). Compared to the initial test, the serum glucose level had increased to over 200 mg/dL; both insulin and C-peptide levels had also increased. We also found that the increment of insulin level during the glucose excursion was faster than that of initial test. Currently, our patient is maintained on azathioprine 100 mg/day, and has not experienced any episodes of hypoglycemia.
- Analysis of insulin binding of erythrocytes
- We compared the insulin receptor binding activity of our patient's pre-treatment serum, post-treatment serum, and normal human serum by adding cold insulin (10-12 to 10-6 mol/L) to normal human erythrocytes. In the case of the patient's pretreatment serum, insulin receptor binding activity was inhibited in a dose-dependent manner until the cold insulin level reached 10-9 mol/L. This result specifically suggests that the patient's serum contained insulin receptor antibodies. After treatment, binding activity recovered to 70% to 80% of normal (Fig. 5).
- Analysis of insulin binding of IM9 lymphocytes
- The ability of the patient's serum to inhibit the binding of 125I-insulin to IM9 lymphocytes is shown in Fig. 6. We measured insulin receptor binding activity by diluting IgG purified from normal human serum, the patient's pre-treatment serum, and the patient's post-treatment serum to 1:20, 1:40, 1:160, 1:320, and 1:640 each in IM9 cell lines. The insulin binding activity of the patient's pre-treatment IgG was reduced in a dose-dependent manner compared to normal IgG. Most dramatically, the 1:20 dilution was 82% inhibited compared to normal IgG. Notably, this inhibitory effect was reduced to 17% after treatment (Fig. 6).
RESULTS
- Insulin resistance syndrome can be classified into type A, in which insulin receptors are absent, and type B, in which insulin receptor autoantibodies are present in serum [1]. First reported by Kahn et al. [9] in 1976, type B insulin resistance syndrome occurs most often in adult women who show other symptoms of autoimmune disease. It can be diagnosed by detection of insulin receptor antibodies [10,11].
- Clinical symptoms can include hyperglycemia, hypoglycemia, hyperinsulinemia, severe insulin resistance, and acanthosis nigricans [1,9,12,13]. While hyperglycemia is a more common symptom, hypoglycemia can occasionally cause serious problems [5,14]. In this paper, we describe a patient with recurrent symptomatic fasting hypoglycemia. This phenomenon appears to be caused by the binding of autoantibodies to insulin receptors, which inhibits the degradation of insulin and results in hyperinsulinemia followed by subsequent hypoglycemia [5]. In some cases, hyperglycemia and hypoglycemia may occur alternately in one patient [15], which suggests there are at least two subtypes of insulin receptor antibodies [14,16].
- The IgG insulin receptor antibody binds the insulin receptor and can have two different effects. Its function can be either inhibitory (by inhibiting insulin binding) or stimulatory (with an insulin-like action), both resulting in hypoglycemia [5,14,15,17]. These different interactions may be explained by quantitative differences in antibody titers. At low titers, the autoantibody appears to act as a partial agonist and result in hypoglycemia, while at high titers it appears to down-regulate the receptor's response to insulin and result in hyperglycemia [14,18]. In our patient, we measured insulin receptor antibodies by quantifying the inhibition of insulin binding to both erythrocytes and IM9 lymphocytes. However, this method is unable to determine the type of activation caused by autoantibody binding. Therefore, further study is needed to elucidate the mechanism of post-receptor signaling.
- In our patient, we observed significant inhibition of insulin binding to erythrocytes and IM9 lymphocytes in a dose-dependent manner, which did not improve after plasmapheresis. Clinically, the patient's symptoms of hypoglycemia and glucose tolerance improved after treatment with prednisolone and azathioprine. We found that insulin binding to erythrocytes gradually normalized to 70% to 80% of normal after immunosuppressive treatment. Furthermore, we found that the patient's dialyzed post-treatment serum inhibited 125I-binding to IM9 lymphocytes by only 17%.
- Yamasaki et al. [19] studied a patient with systemic lupus erythematosus and type B insulin resistance who showed the rapid disappearance of insulin receptor autoantibodies from circulation according to the treatment. They determined the biological and clinical relevance of the patient's insulin receptor antibodies by analyzing the inhibition of insulin binding to IM9 lymphocytes, the uptake of 2-deoxyglucose in CHO cells, and by phosphotyrosine immunoblotting of the insulin receptor. After immunosuppressive treatment, they found attenuation of the insulin binding inhibition present in the patient's serum in parallel with the normalization of the patient's insulin sensitivity. However, in this report the stimulatory activities that promote 2-deoxyglucose uptake and insulin receptor phosphorylation were discordant with the occurrence of fasting hypoglycemia. Thus, this study implicated other pathogenic mechanisms in the development of fasting hypoglycemia, in addition to the insulin-like action of insulin receptor antibodies.
- Our study proved that insulin binding activity was improved after treatment. If our study was further investigated about the post-receptor signaling after autoantibodies were bound to receptors, the mechanism of fasting hypoglycemia was expected to be clearly established.
- Immunosuppressants can be used to treat type B insulin resistance. However, the treatment results have generally been unsatisfactory. In our case, the patient's symptoms did not improve after plasmapheresis, leading us to use a combination of steroids and azathioprine, which resulted in clinical improvement. Arioglu et al. [20] reviewed the long-term clinical course of type B insulin resistance syndrome in 24 patients who were followed for up to 28 years. Although they found that the most effective short-term therapy was high-dose steroids, it remains unclear whether patients presenting with hypoglycemia would benefit from long-term steroid treatment. They also reported that immunomodulation therapy may not influence either the onset of remission or the long-term course of the disease. Nevertheless, immunosuppressive therapy may be considered in patients presenting with severe symptoms who do not spontaneously remit.
- Recently, in 2010, Malek et al. [21] reported a novel approach to reduce the load of insulin receptor antibodies. They treated 7 patients with type B insulin resistance syndrome with a new therapeutic protocol consisting of rituximab and cyclophosphamide combined with pulsed corticosteroids. All 7 patients achieved remission, defined as improved hyperglycemia, discontinuation of insulin therapy, and resolution of hyperandrogenism. This new therapeutic approach is promising in the treatment of both type B insulin resistance as well as other autoantibody receptor diseases.
DISCUSSION
- 1. Cruz PD Jr, Hud JA Jr. Excess insulin binding to insulin-like growth factor receptors: proposed mechanism for acanthosis nigricans. J Invest Dermatol 1992;98(6 Suppl):82S-85S. ArticlePubMed
- 2. Hirata Y, Uchigata Y. Insulin autoimmune syndrome in Japan. Diabetes Res Clin Pract 1994;24(Suppl):S153-S157. ArticlePubMed
- 3. Flier JS, Kahn CR, Roth J, Bar RS. Antibodies that impair insulin receptor binding in an unusual diabetic syndrome with severe insulin resistance. Science 1975;190:63-65. ArticlePubMed
- 4. Braund WJ, Naylor BA, Williamson DH, Buley ID, Clark A, Chapel HM, Turner RC. Autoimmunity to insulin receptor and hypoglycaemia in patient with Hodgkin's disease. Lancet 1987;1:237-240. ArticlePubMed
- 5. Taylor SI, Grunberger G, Marcus-Samuels B, Underhill LH, Dons RF, Ryan J, Roddam RF, Rupe CE, Gorden P. Hypoglycemia associated with antibodies to the insulin receptor. N Engl J Med 1982;307:1422-1426. ArticlePubMed
- 6. Rodriguez O, Collier E, Arakaki R, Gorden P. Characterization of purified autoantibodies to the insulin receptor from six patients with type B insulin resistance. Metabolism 1992;41:325-331. ArticlePubMed
- 7. Dozio N, Micossi P, Galimberti G, Sartori S, Pozza G, Dosio F, Savi A, Gerundini PG, Fazio F, Chiumello G, et al. In vivo demonstration of insulin-receptor defect with 123I-labeled insulin and scintigraphic scanning in severe insulin resistance. Diabetes Care 1992;15:651-656. ArticlePubMedPDF
- 8. Gambhir KK, Archer JA, Carter L. Insulin radioreceptor assay for human erythrocytes. Clin Chem 1977;23:1590-1595. ArticlePubMedPDF
- 9. Kahn CR, Flier JS, Bar RS, Archer JA, Gorden P, Martin MM, Roth J. The syndromes of insulin resistance and acanthosis nigricans. Insulin-receptor disorders in man. N Engl J Med 1976;294:739-745. ArticlePubMed
- 10. Flier JS, Eastman RC, Minaker KL, Matteson D, Rowe JW. Acanthosis nigricans in obese women with hyperandrogenism. Characterization of an insulin-resistant state distinct from the type A and B syndromes. Diabetes 1985;34:101-107. Article
- 11. Taylor SI, Dons RF, Hernandez E, Roth J, Gorden P. Insulin resistance associated with androgen excess in women with autoantibodies to the insulin receptor. Ann Intern Med 1982;97:851-855. ArticlePubMed
- 12. Accili D, Barbetti F, Cama A, Kadowaki H, Kadowaki T, Imano E, Levy-Toledano R, Taylor SI. Mutations in the insulin receptor gene in patients with genetic syndromes of insulin resistance and acanthosis nigricans. J Invest Dermatol 1992;98(6 Suppl):77S-81S. ArticlePubMed
- 13. Cama A, de la Luz Sierra M, Ottini L, Kadowaki T, Gorden P, Imperato-McGinley J, Taylor SI. A mutation in the tyrosine kinase domain of the insulin receptor associated with insulin resistance in an obese woman. J Clin Endocrinol Metab 1991;73:894-901. ArticlePubMed
- 14. De Pirro R, Roth RA, Rossetti L, Goldfine ID. Characterization of the serum from a patient with insulin resistance and hypoglycemia. Evidence for multiple populations of insulin receptor antibodies with different receptor binding and insulin-mimicking activities. Diabetes 1984;33:301-304. ArticlePubMed
- 15. Dons RF, Havlik R, Taylor SI, Baird KL, Chernick SS, Gorden P. Clinical disorders associated with autoantibodies to the insulin receptor. Simulation by passive transfer of immunoglobulins to rats. J Clin Invest 1983;72:1072-1080. ArticlePubMedPMC
- 16. Tsushima T, Omori Y, Murakami H, Hirata Y, Shizume K. Demonstration of heterogeneity of autoantibodies to insulin receptors in type B insulin resistance by isoelectric focusing. Diabetes 1989;38:1090-1096. ArticlePubMed
- 17. Pedersen O, Hjollund E, Beck-Nielsen H, Kromann H. Diabetes mellitus caused by insulin-receptor blockade and impaired sensitivity to insulin. N Engl J Med 1981;304:1085-1088. ArticlePubMed
- 18. Di Paolo S, Giorgino R. Insulin resistance and hypoglycemia in a patient with systemic lupus erythematosus: description of antiinsulin receptor antibodies that enhance insulin binding and inhibit insulin action. J Clin Endocrinol Metab 1991;73:650-657. ArticlePubMed
- 19. Yamasaki H, Yamaguchi Y, Fujita N, Kato C, Kuwahara H, Yamauchi MD, Yamakawa K, Abe T, Ozaki M, Sera Y, Uotani S, Kawasaki E, Takino H, Eguchi K. Anti-insulin receptor autoantibodies in a patient with type B insulin resistance and fasting hypoglycemia. Acta Diabetol 2000;37:189-196. ArticlePubMedPDF
- 20. Arioglu E, Andewelt A, Diabo C, Bell M, Taylor SI, Gorden P. Clinical course of the syndrome of autoantibodies to the insulin receptor (type B insulin resistance): a 28-year perspective. Medicine (Baltimore) 2002;81:87-100. PubMed
- 21. Malek R, Chong AY, Lupsa BC, Lungu AO, Cochran EK, Soos MA, Semple RK, Balow JE, Gorden P. Treatment of type B insulin resistance: a novel approach to reduce insulin receptor autoantibodies. J Clin Endocrinol Metab 2010;95:3641-3647. ArticlePubMedPMC
REFERENCES
Fig. 1Thickened, hyperpigmented skin lesions (acanthosis nigricans) were observed on the posterior neck, axillae and groin.
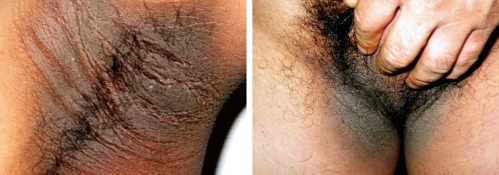
Fig. 2Initial 24-hour glucose profile using a continuous glucose monitoring system during a 72-hour fasting test.
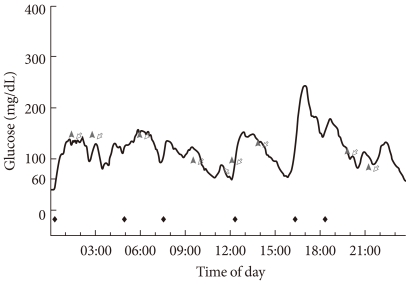
Fig. 3Pre- and post-treatment serum levels of insulin and C-peptide after 75 g oral glucose tolerance test. (A) On admission. (B) Sixteen-month follow-up.
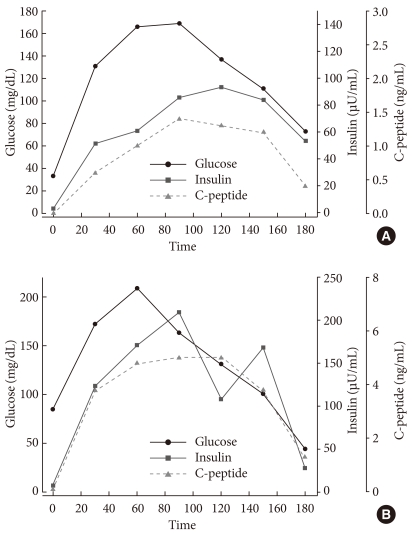

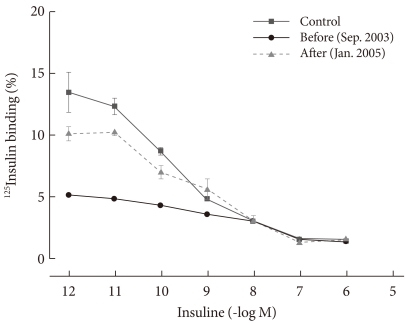
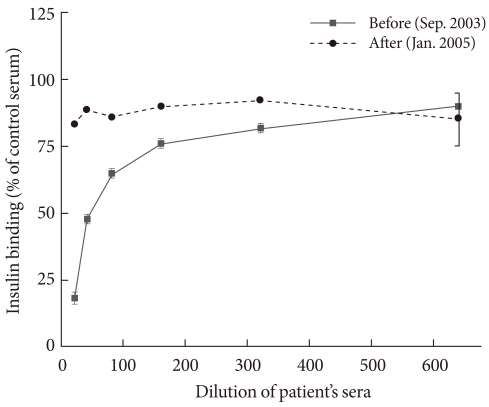
Figure & Data
References
Citations
Citations to this article as recorded by 
- Systematic Review—Type B Insulin Resistance With Isolated Hypoglycemia and Suppressed Insulin
Natasha Brown, Marianne S Elston
The Journal of Clinical Endocrinology & Metabolism.2024; 109(4): 936. CrossRef - Type B insulin resistance syndrome: a systematic review
Luizianne Mariano Martins, Virgínia Oliveira Fernandes, Manuela Montenegro Dias de Carvalho, Daniel Duarte Gadelha, Paulo Cruz de Queiroz, Renan Magalhães Montenegro
Archives of Endocrinology and Metabolism.2020;[Epub] CrossRef - Autoimmune hypoglycemia
Marina Y. Yukina, Diana A. Davtyan, Ekaterina A. Troshina, Nurana F. Nuralieva
Obesity and metabolism.2018; 15(3): 9. CrossRef - Unique pharmacology of a novel allosteric agonist/sensitizer insulin receptor monoclonal antibody
Simon A. Hinke, Anne M. Cieniewicz, Thomas Kirchner, Katharine D'Aquino, Rupesh Nanjunda, Jason Aligo, Robert Perkinson, Philip Cooper, Ken Boayke, Mark L. Chiu, Steve Jarantow, Eilyn R. Lacy, Yin Liang, Dana L. Johnson, Jean M. Whaley, Russell B. Lingham
Molecular Metabolism.2018; 10: 87. CrossRef - Combined Immunosuppressive Therapy Induces Remission in Patients With Severe Type B Insulin Resistance: A Prospective Cohort Study
Joanna Klubo-Gwiezdzinska, Maria Lange, Elaine Cochran, Robert K. Semple, Cornelia Gewert, Rebecca J. Brown, Phillip Gorden
Diabetes Care.2018; 41(11): 2353. CrossRef - Hypoinsulinemic Hypoglycemia Followed By The Onset Of Severe Insulin Resistance With Hyperglycemia And Circulating Anti-Insulin Receptor Antibodies In A Patient Suffering Systemic Lupus Erythematosus: A Case Report And Literature Review
Guillermo Martínez de Pinillos, Mariana Tomé, María M. Viloria, Joaquín Bobillo, María V. Cózar
AACE Clinical Case Reports.2017; 3(3): e284. CrossRef - The treatment of hyperinsulinemic hypoglycaemia in adults: an update
M. V. Davi′, A. Pia, V. Guarnotta, G. Pizza, A. Colao, A. Faggiano
Journal of Endocrinological Investigation.2017; 40(1): 9. CrossRef - Immunosuppressive Therapy in Treatment of Refractory Hypoglycemia in Type B Insulin Resistance: A Case Report
Lavanya Viswanathan, Imali Sirisena
Journal of the Endocrine Society.2017; 1(12): 1435. CrossRef - 反復する低血糖発作を契機に発見されたインスリン受容体異常症B型の1例(A case of type B insulin resistance presenting as recurrent hypoglycemia)
杉本 龍 (Ryu Sugimoto), 髙木 誠 (Makoto Takaki), 前原 潤一 (Junichi Maehara), 具嶋 泰弘 (Yasuhiro Gushima)
Nihon Kyukyu Igakukai Zasshi: Journal of Japanese Association for Acute Medicine.2017; 28(3): 100. CrossRef - Type B insulin resistance syndrome
Devina L. Willard, Mary Stevenson, Devin Steenkamp
Current Opinion in Endocrinology, Diabetes & Obesity.2016; 23(4): 318. CrossRef - Antibody-Mediated Insulin Resistance: When Insulin and Insulin Receptor Act as Autoantigens in Humans
Christelle Liminet, Julien Vouillarmet, Karim Chikh, Emmanuel Disse
Canadian Journal of Diabetes.2016; 40(5): 462. CrossRef - The insulin autoimmune syndrome (IAS) as a cause of hypoglycaemia: an update on the pathophysiology, biochemical investigations and diagnosis
Adel A.A. Ismail
Clinical Chemistry and Laboratory Medicine (CCLM).2016; 54(11): 1715. CrossRef - Type B insulin-resistance syndrome presenting as autoimmune hypoglycemia, associated with systemic lupus erythematosus and interstitial lung disease
Seon Mee Kang, Heung Yong Jin, Kyung Ae Lee, Ji Hyun Park, Hong Sun Baek, Tae Sun Park
The Korean Journal of Internal Medicine.2013; 28(1): 98. CrossRef - Treatment of recurrent hypoglycemia with plasmapheresis and steroid in nondiabetic patient
Mustafa Kulaksızoglu, Mustafa Sait Gonen, Levent Kebapcilar, Fatih Sahin, Fatih Demirci, Ali Topcu
Transfusion and Apheresis Science.2013; 48(1): 11. CrossRef - A Case of Persistent Hypoglycemia: When to Think Outside the Box
Yogeswari Venugopal, Shireene Vethakkan, Sargunan Sockalingam, Raja Jasmin, Karen Choong
Clinical Diabetes.2013; 31(3): 130. CrossRef - The effect of hyperglycemia and hypoglycemia on glucose transport and expression of glucose transporters in human lymphocytes B and T: An in vitro study
Bożenna Oleszczak, Leszek Szablewski, Monika Pliszka
Diabetes Research and Clinical Practice.2012; 96(2): 170. CrossRef - The effect of glucose concentrations in the medium on expression of insulin receptors in human lymphocytes B and T: anin vitrostudy
Bożenna Oleszczak, Leszek Szablewski, Monika Pliszka
Journal of Receptors and Signal Transduction.2012; 32(5): 263. CrossRef - Fulminant Type 1 diabetes in a pregnant woman as an initial manifestation of the insulin autoimmune syndrome
H. S. Kim, T.‐Y. Lee, E. Y. Kim, J. H. Choi, S. Y. Kim, Y.‐C. Hwang, J.‐H. Kang, K. J. Ahn, H. Y. Chung, I.‐K. Jeong
Diabetic Medicine.2012; 29(10): 1335. CrossRef - A Case of the Type B Insulin Resistance Syndrome with Chronic Hepatitis B
Hyun Seok Choi, Byoung Ho Choi, Seok Hoo Jeong, Shung Han Choi, Dong Su Shin, Sei hyun Kim, Young Sil Eom, Sihoon Lee, Yeun Sun Kim, Ie Byung Park, Ki Young Lee
Endocrinology and Metabolism.2011; 26(4): 360. CrossRef
 PubReader
PubReader Cite
Cite