
- Current
- Browse
- Collections
-
For contributors
- For Authors
- Instructions to authors
- Article processing charge
- e-submission
- For Reviewers
- Instructions for reviewers
- How to become a reviewer
- Best reviewers
- For Readers
- Readership
- Subscription
- Permission guidelines
- About
- Editorial policy
Articles
- Page Path
- HOME > Diabetes Metab J > Volume 48(2); 2024 > Article
-
Original ArticleOthers Comparative Effect of Glucose-Lowering Drugs for Type 2 Diabetes Mellitus on Stroke Prevention: A Systematic Review and Network Meta-Analysis
-
Ji Soo Kim1*
 , Gyeongsil Lee2*, Kyung-Il Park3, Seung-Won Oh4
, Gyeongsil Lee2*, Kyung-Il Park3, Seung-Won Oh4 -
Diabetes & Metabolism Journal 2024;48(2):312-320.
DOI: https://doi.org/10.4093/dmj.2022.0421
Published online: January 26, 2024
1International Healthcare Center, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seoul, Korea
2Esther Formula Medical Food R&D Center, Seoul, Korea
3Department of Neurology, Seoul National University Hospital Healthcare System Gangnam Center, Seoul, Korea
4Department of Family Medicine, Seoul National University Hospital Healthcare System Gangnam Center, Seoul National University College of Medicine, Seoul, Korea
-
Corresponding author: Seung-Won Oh Department of Family Medicine, Seoul National University Hospital Healthcare System Gangnam Center, Seoul National University College of Medicine, 152 Teheran-ro, Gangnam-gu, Seoul 06236, Korea E-mail: sw.oh@snu.ac.kr
- *Ji Soo Kim and Gyeongsil Lee contributed equally to this study as first authors.
Copyright © 2024 Korean Diabetes Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Background
- There is still a lack of research on which diabetic drugs are more effective in preventing stroke. Our network metaanalysis aimed to compare cerebrovascular benefits among glucose-lowering treatments.
-
Methods
- We searched MEDLINE, EMBASE, the Cochrane Central Register of Controlled Trials, and the ClinicalTrials.gov registry for clinical trials from inception through May 25, 2021. We included both prespecified cerebrovascular outcomes and cerebrovascular events reported as severe adverse events. Subgroup analyses were conducted by stroke subtype, publication type, age of patients, baseline glycosylated hemoglobin (HbA1c), duration of type 2 diabetes mellitus, and cardiovascular risks.
-
Results
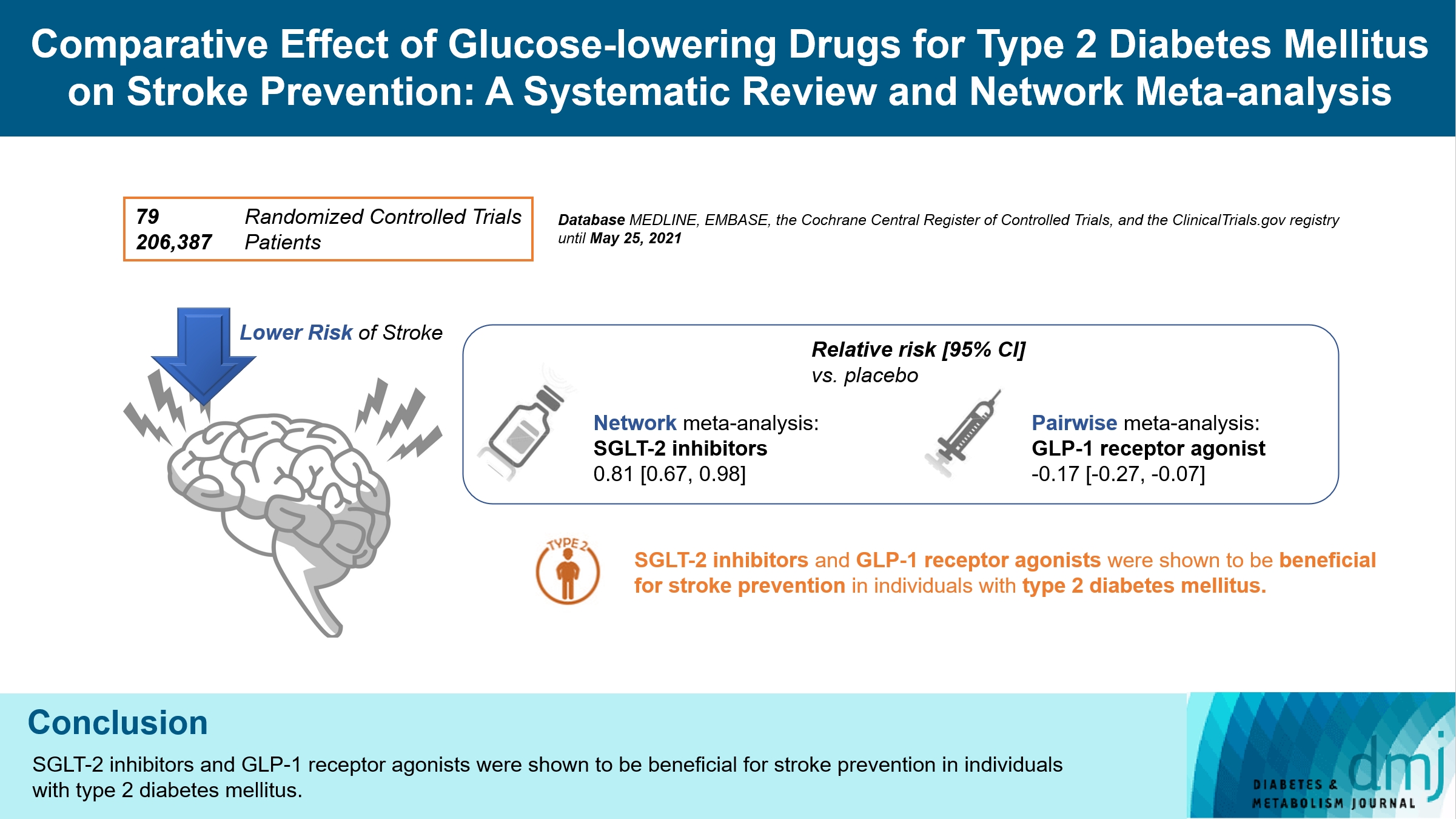
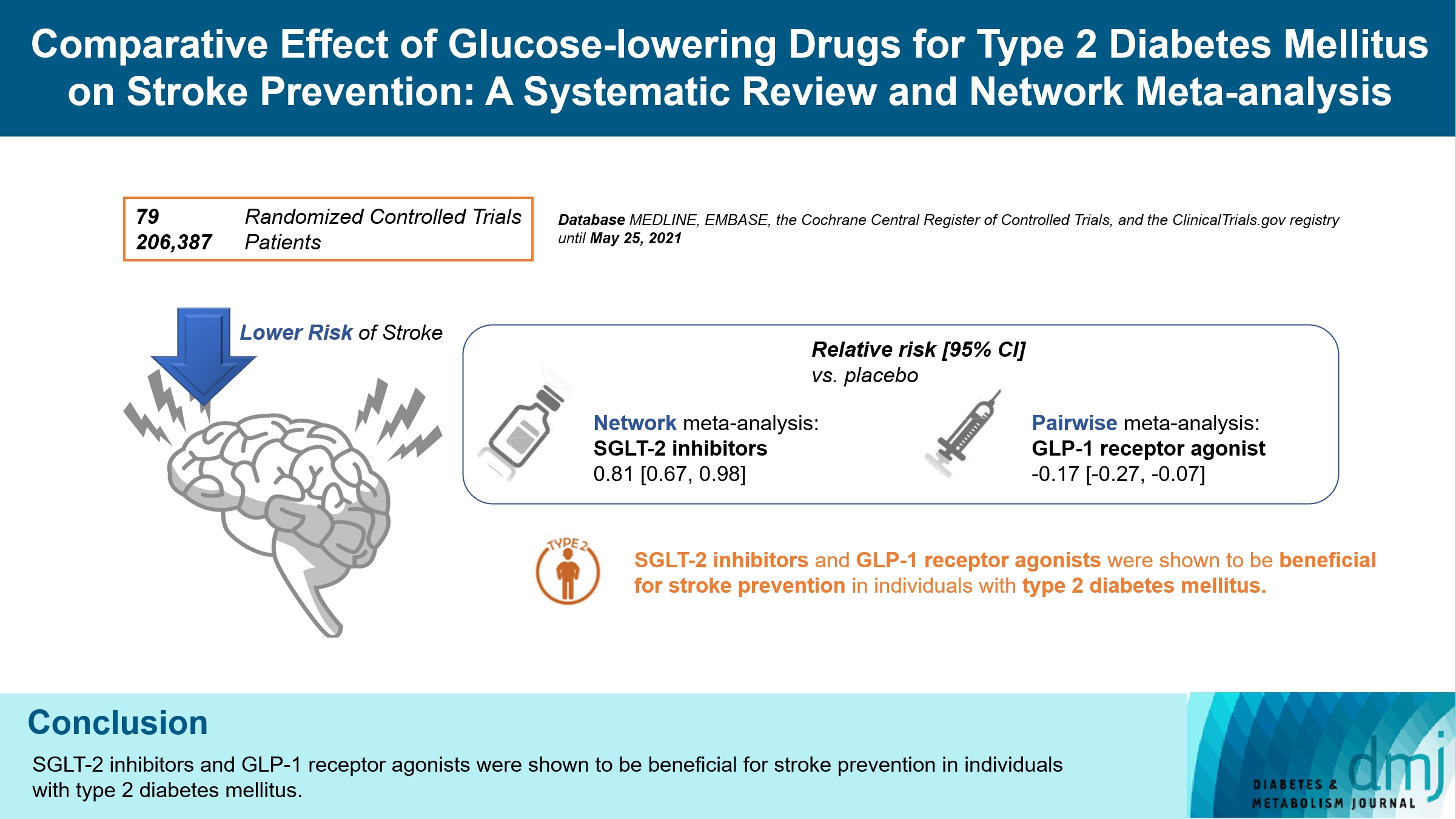
- Of 2,861 reports and 1,779 trials screened, 79 randomized controlled trials comprising 206,387 patients fulfilled the inclusion criteria. In the pairwise meta-analysis, the use of glucagon-like peptide-1 (GLP-1) agonist was associated with a lower risk of total stroke compared with placebo (relative risk [RR], –0.17; 95% confidence interval [CI], –0.27 to –0.07). In the network meta-analysis, only the use of sodium-glucose cotransporter-2 (SGLT-2) inhibitor was associated with a reduction of total stroke, compared with placebo (RR, 0.81; 95% CI, 0.67 to 0.98). In the subgroup analyses, the use of SGLT-2 inhibitor and GLP-1 agonist was associated with a lower risk of stroke in those with high HbA1c (≥8.0) and low-risk of cardiovascular disease, respectively.
-
Conclusion
- SGLT-2 inhibitors and GLP-1 agonists were shown to be beneficial for stroke prevention in patients with type 2 diabetes mellitus.
- • This study compared stroke events across anti-diabetic medications.
- • A total of 79 randomized controlled trials were included.
- • Pairwise meta-analysis linked GLP-1 receptor agonists to reduced total stroke risk.
- • Network meta-analysis showed only SGLT-2 inhibitors correlated with lower stroke risk.
- • SGLT-2 inhibitors and GLP-1 receptor agonists may benefit stroke prevention in T2DM.
Highlights
- Diabetes and hyperglycemia are established risk factors of stroke [1]. There is evidence concerning the pathogenetic mechanisms and clinical conditions that may underlie the propensity for cerebrovascular diseases in diabetic patients [2,3]. Metformin is the preferred initial pharmacologic agent for treating type 2 diabetes mellitus (T2DM), and other glucose-lowering agents can be considered according to comorbidities or patient-centered treatment factors [4,5]. However, the optimal glucose-lowering treatment for preventing stroke is unclear.
- Several large-scale studies have shown the superiority of newer antidiabetic medications for preventing poor cardiovascular outcomes and related mortality [6]. However, analyses about the effects of antidiabetic medications on stroke have shown inconsistent results [7,8]. Pioglitazone did not reduce stroke compared with placebo, but it had a significant effect in preventing stroke recurrence in the PROspective pioglitAzone Clinical Trial In macroVascular Events (PROactive) [9]. Sodium-glucose cotransporter-2 (SGLT-2) inhibitor use was associated with reduced cardiovascular events and mortality compared to placebo in the Empagliflozin Cardiovascular Outcome Event Trial in Type 2 diabetes Mellitus Patients (EMPA-REG OUTCOME), CANagliflozin cardioVascular Assessment Study (CANVAS), and Dapagliflozin Effect on Cardiovascular Events– Thrombolysis in Myocardial Infarction 58 (DECLARE-TIMI58) trials. However, its effects on stroke were neutral or non-significant [10-13]. Semaglutide, in the Trial to Evaluate Cardiovascular and Other Long-term Outcomes With Semaglutide in Subjects With Type 2 Diabetes (SUSTAIN-6), showed a significant reduction of nonfatal stroke compared to placebo. However, the trial was a noninferiority study and was not powered to show the superiority of specific stroke endpoints [13]. Furthermore, studies of other glucagon-like peptide-1 (GLP-1) analogs did not show significant reductions in stroke events [14-17]. In this study, we aimed to compare stroke events among glucose-lowering treatments, by conducting a network meta-analysis.
INTRODUCTION
- Search strategy and selection criteria
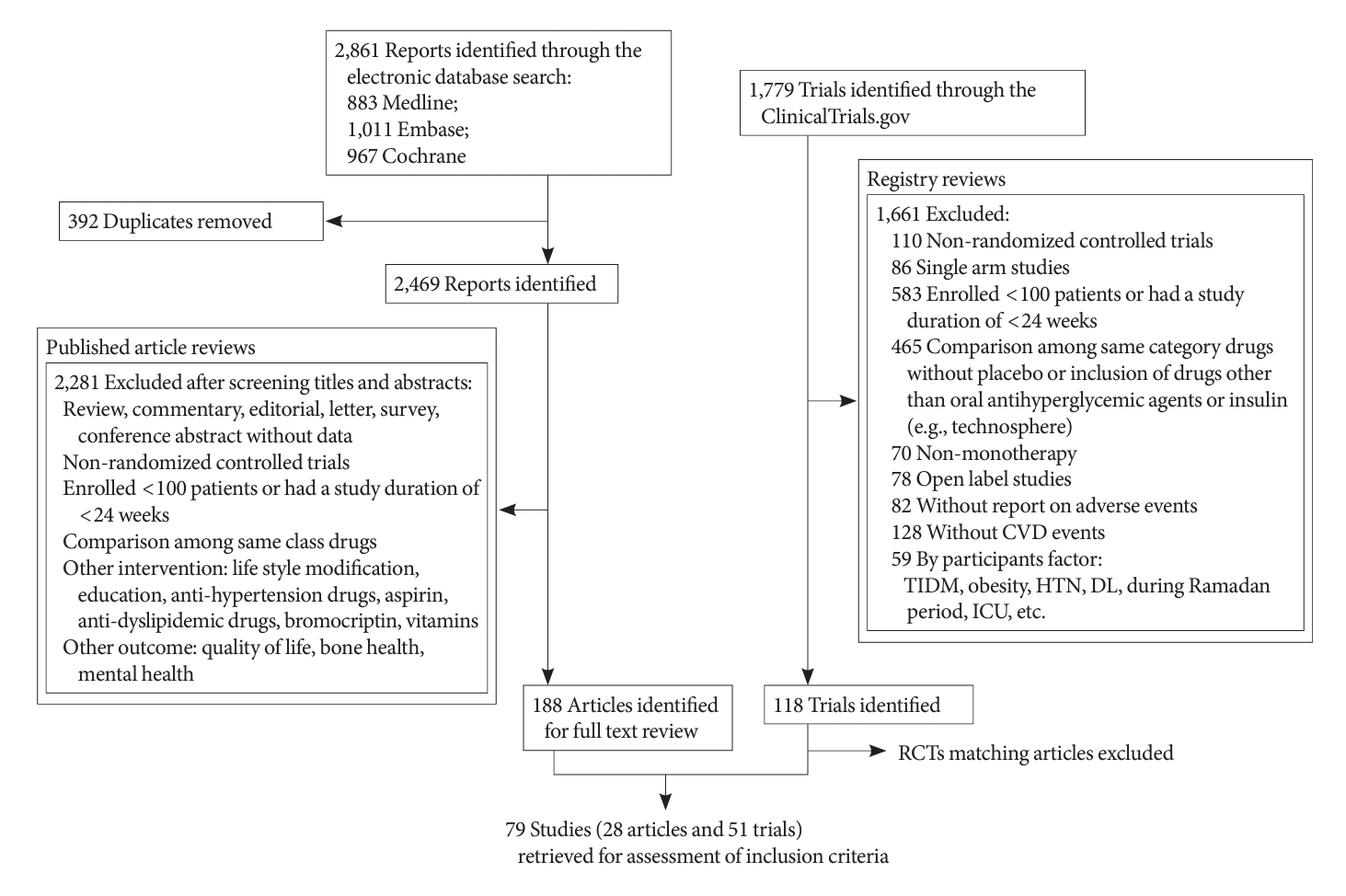
- The systematic review (PROSPERO: CRD42018082633) protocol was drafted based on the Preferred Reporting Items for Systematic reviews and Meta-Analyses Extension for Network Meta-Analysis (PRISMA-NMA) [18]. MEDLINE, EMBASE, and the Cochrane Central Register of Controlled Trials were searched for articles published from inception through May 25, 2021 (Fig. 1 and Supplementary Tables 1, 2). The glucose-lowering drugs targeted in our comparison were metformin, sulfonylureas, thiazolidinedione, dipeptidyl peptidase 4 (DPP-4) inhibitors, SGLT-2 inhibitors, alpha-glucosidase inhibitors, meglitinide, GLP-1 agonist, and insulin. When searching the ClinicalTrials.gov registry, we did not use the outcome keywords. As a result, we reviewed all registered clinical trials including unpublished reports on antidiabetic drugs that met our comparison criteria. We included not only prespecified outcomes, but also cerebrovascular events reported as severe adverse events (SAEs). Additionally, publications were retrieved from the bibliographies of relevant manuscripts if they were considered pertinent. All citations were eligible for inclusion regardless of publication year or language.
- After removing duplicate citations, two authors (J.S.K. and G.L.) independently screened the titles and abstracts to identify potentially relevant citations. Full texts were then reviewed to establish whether all prespecified inclusion criteria were met: participants were adults with T2DM; group allocation was based on antidiabetic drug use; the study reported at least two groups; comparison was among monotherapy treatment pertaining to different drug category; participants were followed up for at least 24 weeks; more than 100 participants were randomized; and the number of fatal or nonfatal strokes, including hemorrhagic stroke, ischemic stroke, or transient ischemic attack (TIA) was reported. Disagreements regarding study inclusion or exclusion were resolved by discussion with another author (S.W.O.).
- Data extraction and risk of bias assessment
- One author (J.S.K.) used a standardized form to extract data from each included study, and a second author (G.L.) verified data accuracy and completeness (Supplementary Table 2). The following were recorded: data sources (published articles and ClinicalTrials.gov registries); lead author and year of publication; study design and phase; duration of study; antidiabetic drug use at enrollment; participant age, percentage of male or female participants, ethnicity, and baseline glycosylated hemoglobin (HbA1c) level; duration of T2DM; duration of follow-up; prespecified outcomes or SAE measured; number of randomized participants allocated with each antidiabetic agent; and number of participants who experienced each outcome or SAEs.
- We did not impose limitations on background medication. If there was no change in the use of a background medication, we did not include the particular background medication in the analyses. When trials switched from one drug to another or added a drug, we determined the group based on which treatment was administered for a longer duration. Separate drug dosages were not evaluated in the analyses. When results of one trial were published separately due to an extended study duration, we used the results from the extended duration. We prioritized published data when both published and unpublished data were available.
- Cerebrovascular outcome or events consisted of ischemic stroke (ischemia, ischemic stroke, vertebrobasilar insufficiency, cerebrovascular insufficiency, and lacunar infarction) or TIA (including reversible ischemic neurologic deficit), hemorrhagic stroke (hemorrhage and cerebral hematoma), and unspecified stroke (cerebrovascular accident, cerebrovascular disorder, hemiplegia, and hemiparesis). We excluded cerebrovascular outcomes or events that could not be identified as ischemic stroke, TIA, hemorrhagic stroke, or unspecified stroke. Parts of a study duration that were not chosen for data extraction were also excluded. The Cochrane Collaboration tool for assessing the risk of bias was used to examine the quality of eligible randomized controlled trials (RCTs) [19]. Both the manuscript and protocol were reviewed for relevant information on quality (Supplementary Table 3 and Supplementary Fig. 1). The risk of bias was assessed by one author (J.S.K.) and cross-checked by a second author (S.W.O.).
- Data synthesis and analysis
- We undertook pairwise meta-analyses for within-study comparisons between one antidiabetic drug and placebo or other antidiabetic drugs using Mantel-Haenszel fixed-effects models [20]. Results were reported as relative risks (RRs) and corresponding 95% confidence intervals (CIs) [21]. Heterogeneity was measured with the I2 statistic. Then, a network meta-analysis was constructed to combine the direct and indirect evidence. After generating network geometry, overall and local loop inconsistency tests were performed. Network forest plots, interval plot, and league table of effect size by treatment were used to display effect sizes. Treatments were ranked in order according to the superiority of their treatment effect based on the surface under the cumulative ranking curves (SUCRA) percentages. Lastly, we evaluated publication bias in the network meta-analysis using a network funnel plot.
- Subgroup analyses were conducted, stratified by stroke subtypes (ischemic stroke, hemorrhagic stroke, unspecified stroke, and TIA) and publication type (published by peer-reviewed journal or unpublished [Clinicaltrials.gov database-only]) (Supplementary Figs. 2-7). Subgroup analyses were also conducted according to age (<65 and ≥65 years), baseline HbA1c (<8.0 and ≥8.0), duration of type 2 diabetes mellitus (<10 and ≥10 years), and presence of low or high cardiovascular disease risk (history of renal impairment, heart failure, or old age) (Supplementary Figs. 8-15). All statistical analyses were performed using Stata version 16.1 (StataCorp LP, College Station, TX, USA).
METHODS
- Fig. 1 shows the flow diagram of this study according to the PRISMA-NMA statement. The literature search identified 2,861 reports and 1,779 trials. After screening the titles and abstracts, 3,869 studies were excluded, because they did not meet the predetermined selection criteria. The full texts of 188 studies and 118 trials were reviewed. Finally, 79 RCTs were included in the final analysis. Supplementary Table 2 summarizes the characteristics of the included trials.
- The RCTs focused on metformin, sulfonylureas, thiazolidinedione, DPP-4 inhibitors, SGLT-2 inhibitors, alpha-glucosidase inhibitors, GLP-1 agonists, and insulin. RCTs on insulin were excluded from the final analysis because no studies met the inclusion criteria. The mean patient age was 49 to 74 years. Baseline HbA1c levels were 6.8% to 9.5%, and the duration from diabetes diagnosis ranged from naïve to a mean of 18 years. Participants were diverse in terms of ethnicity (Caucasian, Asian, and multi-ethnicity). The results of the risk of bias assessment are presented in Supplementary Table 3 and Supplementary Fig. 1. Overall, 43 (54.4%) out of 79 RCTs provided details on randomization and allocation concealment procedures.
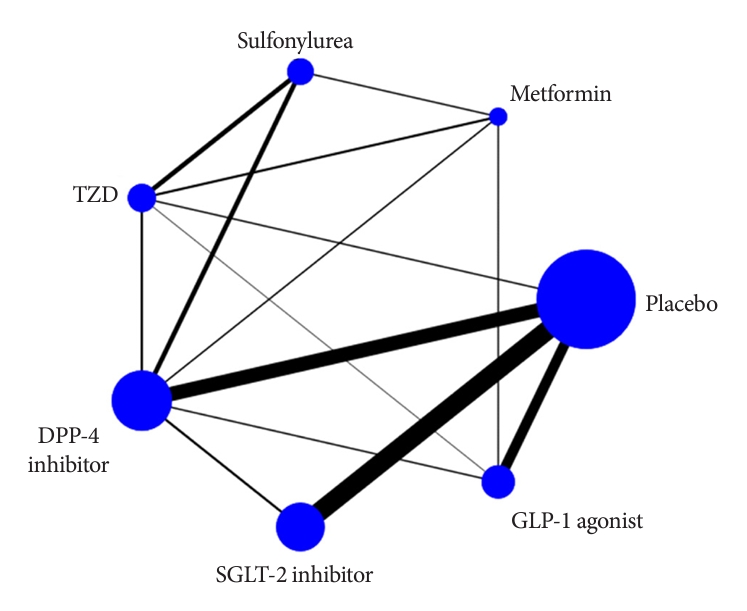
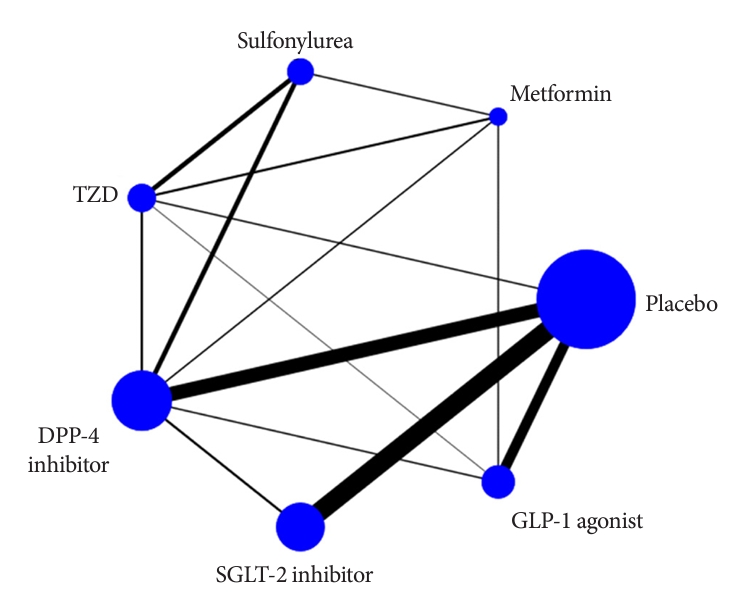
- The final analysis included data from 79 RCTs reporting 4,625 (2.2%) total strokes in 206,387 patients. In the network plot of eligible comparisons (test of consistency; P=0.953), the most frequent studies compared placebo versus SGLT-2 inhibitor and placebo versus DPP-4 inhibitor (Fig. 2). An inconsistency test was performed to compare direct and indirect treatment in mixed treatment (Supplementary Table 4). A traditional pairwise and network meta-analyses for total stroke (Table 1) and corresponding network forest plot and interval plot (Supplementary Figs. 16 and 17, respectively) were used. In the pairwise meta-analysis, GLP-1 agonist use was associated with a lower risk of total stroke compared with placebo, based on data from 58,399 patients in 13 studies (855 events/38,921 subjects with placebo vs. 724 events/29,478 subjects with GLP-1 agonist; RR, –0.17; 95% CI, –0.27 to –0.07). In the network meta-analysis, only SGLT-2 inhibitor use was associated with a reduction in total stroke, compared with placebo (RR, 0.81; 95% CI, 0.67 to 0.98). There were no significant differences between the other antidiabetic drugs and placebo. Regarding the ranking of the most superior treatment, SGLT-2 inhibitor showed the leading effect (SUCRA 76.4%), followed by GLP-1 agonist (SUCRA 71.7%). The probability of SGLT-2 inhibitor being the best was 31.0%, and its probability to be at least the second best was 29.2% (Supplementary Fig. 18). Through the comparison-adjusted funnel plot, we confirmed these data were relatively symmetric, indicating rare small-study effects in the network (Supplementary Fig. 19).
- The results of the subgroup analyses stratified by stroke subtype (ischemic stroke [44 trials], hemorrhagic stroke [20 trials], unspecified stroke [37 trials], and TIA [26 trials]), and publication type (published [44 trials] and unpublished [35 trials] studies) are shown in Supplementary Figs. 2-7. There were no significant differences between antidiabetic drugs and placebo in these analyses. The results of the subgroup analyses stratified by age, baseline HbA1c, duration of diabetes, and cardiovascular risk status are shown in Supplementary Figs. 8-15. The subgroup analysis of subjects with baseline HbA1c ≥8.0% (51 trials) was in line with the full analysis, in which SGLT-2 inhibitor was associated with a lower risk than placebo (RR, 0.78; 95% CI, 0.62 to 0.97) (Supplementary Fig. 11). In the subgroup analysis of low cardiovascular disease risk (40 trials), GLP-1 agonist was associated with a lower risk of total stroke compared to placebo (RR, 0.82; 95% CI, 0.73 to 0.93) (Supplementary Fig. 14).
RESULTS
- In this network meta-analysis, we identified 79 RCTs that reported cerebrovascular outcomes for antidiabetic drugs. Our study showed that SGLT-2 inhibitors and GLP-1 agonists, among glucose-lowering treatments, had benefits for total stroke compared to placebo, in patients with T2DM.
- In a previous network meta-analysis comparing cardiovascular outcomes among new antidiabetic drug classes, SGLT-2 inhibitors did not reduce nonfatal stroke [5]. In a meta-analysis of five RCTs which directly compared SGLT-2 inhibitors to placebo, there was no significant effect on total stroke; a pooled analysis of three trials showed that SGLT-2 inhibitors were associated with a substantial reduction in hemorrhagic stroke alone [22]. However, in the present study, the network metaanalysis showed that SGLT-2 inhibitors had a significant preventive effect on total stroke, while the traditional pairwise meta-analysis of 24 RCTs comparing the effect of SGLT-2 inhibitors and placebo was not significant. Our study included more recent RCTs on SGLT-2 inhibitors, such as the Sotagliflozin on Cardiovascular and Renal Events in Patients with Type 2 Diabetes and Moderate Renal Impairment Who Are at Cardiovascular Risk (SCORED) and Sotagliflozin on Cardiovascular Events in Patients with Type 2 Diabetes Post Worsening Heart Failure (SOLOIST-WHF) trials, which may have contributed to this mixed result. In the SCORED trial, which enrolled 10,584 diabetic patients with chronic kidney disease, sotagliflozin showed a stroke-protective effect [23]. On the other hand, in the SOLOIST-WHF trial consisting of 1,222 diabetic patients with recent worsening health failure, there was a greater number of stroke events in the sotagliflozin group than in the placebo group [24]. Sotagliflozin is a SGLT-1 and SGLT-2 co-inhibitor, so the additive effects might affect cardiovascular outcome [25]. In the network meta-analysis after exclusion of studies on sotagliflozin, the association for SGLT-2 inhibitors remained statistically significant (Supplementary Table 5). Nevertheless, SGLT-1 versus SGLT-2 selectivity might have had an impact on the results of stroke prevention, and this effect may have contributed to the discrepancy between pairwise meta-analysis and network meta-analysis.
- GLP-1 agonist use was associated with a lower risk of total stroke based on the pairwise meta-analysis in our study. This coincides with results from previous meta-analyses in which GLP-1 agonists were associated with a 15% lower risk of nonfatal stroke and a 16% lower risk of total stroke [26,27]. Our study also comprised newer trials such as the Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results (LEADER) and SUSTAIN-6 trials, which focused on liraglutide and semaglutide, respectively [13,14]. These studies reported the superiority of GLP-1 agonists in terms of the cardiovascular composite outcome but not regarding stroke. In addition, the exploratory subanalysis of the Dulaglutide and cardiovascular outcomes in type 2 diabetes (REWIND) trial which investigated the effect of dulaglutide on stroke were included in our study. In this trial, weekly dulaglutide reduced ischemic stroke (hazard ratio [HR], 0.75; 95% CI, 0.59 to 0.94; P=0.012), nonfatal stroke (HR, 0.76; 95% CI, 0.61 to 0.95; P=0.017), and disabling stroke (HR, 0.74; 95% CI, 0.56 to 0.99; P=0.042) [28].
- The difference among glucose-lowering medications regarding the effect on stroke may be attributed to various drug mechanisms in terms of glucose variability [13] and hemodynamics. Diabetic patients are known to suffer from episodes of asymptomatic and symptomatic hypoglycemia, and one of the most common causes is intensive glycemic control [29]. Severe hypoglycemia can lead to brain injury via neuroinflammatory pathways and has been shown to increase stroke risk even in prediabetic patients [30]. Drugs with greater glucose variability may mechanistically increase the risk of stroke. Studies have shown that long-term glucose variability in T2DM is correlated with an increased risk of macrovascular complications; the Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial substantiates this effect [31,32]. A meta-analysis by Lee et al. [33] showed the correlation between SGLT-2 inhibitors and GLP-1 agonists, and glucose variability. Both SGLT-2 inhibitors and GLP-1 agonists were significantly associated with a reduction in the mean amplitude of glucose excursion and mean blood glucose levels and an increase in the percentage of time with euglycemic levels [33]. DPP-4 inhibitors also reduced glucose variability compared to other antidiabetic agents. However, comparison groups mostly included sulfonylureas [34]. In addition, the effects on neuroinflammation or endothelial dysfunction associated with atherosclerosis may also cause differences between drugs [8].
- Subgroup analyses showed the SGLT-2 inhibitors use was associated with a reduced risk of total stroke in patients with HbA1c ≥8.0% [35,36]. In a trial consisting of diabetic and hypertensive patients with a mean HbA1c of 8.59, empagliflozin, compared to placebo, showed a lower number of cerebrovascular events [37]. SGLT-2 inhibitors are known to have a pleiotropic effect on hemodynamics. Possible mechanisms by which SGLT-2 inhibitors exert their cardiorenal benefits include reductions in insulin resistance, inflammation, oxidative stress [38], and the risk of albuminuria [39,40]. The high HbA1c group is more vulnerable in these respects, and for this reason, SGLT-2 inhibitor may have shown a more protective effect in this group [21]. Further investigation is warranted to explore the impact of SGLT-2 inhibitors on stroke in patients with relatively high HbA1c.
- Our study also showed GLP-1 agonists were associated with a lower risk of total stroke in patients without cardiovascular disease risk such as renal impairment, heart failure, or old age. Compared to previous meta-analyses [25,26] our meta-analysis included more recent studies on semaglutide (Peptide Innovation for Early Diabetes Treatment [PIONEER] 1 and PIONEER 5) [41,42]. In the PIONEER 5 trial, in which patients had moderate renal impairment, there were two cerebrovascular events in the semaglutide group and none in the placebo group. However, the PIONEER 1 trial, which did not consist of a high cardiovascular disease risk population, showed no cerebrovascular events in the semaglutide group and three in the placebo group. Collectively, these results may have influenced the association observed in the low-risk subgroup. GLP-1 agonists have a positive effect on the reduction of weight, blood pressure, and serum lipids; in a meta-analysis that included longer duration studies, GLP-1 agonists showed neuroprotective effects [43]. However, in high-risk patients with advanced complications, these positive effects may not be sufficiently exhibited. Additionally, the issue of the differing effects of GLP-1 agonists on stroke based on the type of GLP-1 agonist (intravenous exenatide, oral semaglutide, etc.), partly owing to different half-lives, has been noted [5,44]. Therefore, future studies comparing stroke outcomes based on risk stratification and among drugs pertaining to the same class are necessary.
- Several limitations should be considered when interpreting our results. First, the study included both prespecified cerebrovascular outcomes and cerebrovascular events reported as SAEs. This aspect added value in terms of the comprehensiveness of our study. However, it may have also contributed to study heterogeneity. Although there was no inconsistency in our study, the difference between SGLT-2 inhibitor and placebo became non-significant in the subgroup analysis of published trials only. Second, our study only included monotherapy without differentiating background and/or add-on therapy. Therefore, it is difficult to apply the results of this study when two or more drugs are used in combination.
- In conclusion, the present meta-analysis demonstrates the benefits of SGLT-2 inhibitors and GLP-1 agonists for stroke prevention. Further studies with outcomes for different stroke subtypes, in varying clinical conditions, would provide more evidence to compare the effects of antidiabetic drugs on cerebrovascular outcomes.
DISCUSSION
SUPPLEMENTARY MATERIALS
Supplementary Table 1.
Supplementary Table 2.
Supplementary Table 4.
Supplementary Table 5.
Supplementary Fig. 1.
Supplementary Fig. 2.
Supplementary Fig. 3.
Supplementary Fig. 4.
Supplementary Fig. 5.
Supplementary Fig. 6.
Supplementary Fig. 7.
Supplementary Fig. 8.
Supplementary Fig. 9.
Supplementary Fig. 10.
Supplementary Fig. 11.
Supplementary Fig. 12.
Supplementary Fig. 13.
Supplementary Fig. 14.
Supplementary Fig. 15.
Supplementary Fig. 16.
Supplementary Fig. 17.
Supplementary Fig. 18.
Supplementary Fig. 19.
-
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article, including the Esther Formula Medical Food R&D Center, was reported.
-
AUTHOR CONTRIBUTIONS
Conception or design: S.W.O.
Acquisition, analysis, or interpretation of data: J.S.K., G.L.
Drafting the work or revising: J.S.K., S.W.O.
Final approval of the manuscript: J.S.K., G.L., K.I.P., S.W.O.
-
FUNDING
The study was supported by the Seoul National University Hospital Research Fund grant no. 23-2017-0010.
NOTES
-
Acknowledgements
- None
| Placebo | Metformin | Sulfonylurea | TZD | DPP-4 inhibitor | SGLT-2 inhibitor | GLP-1 agonist | |
|---|---|---|---|---|---|---|---|
| Placebo | - | - | 2 Studies | 19 Studies | 24 Studies | 13 Studies | |
| I2 =0.0% | I2 =0.0% | I2 =64.3% | I2 =0.00% | ||||
| –0.22 (–0.51 to 0.07) | –0.04 (–0.17 to 0.08) | –0.22 (–0.50 to 0.06) | –0.17 (–0.27 to –0.07)a | ||||
| Metformin | 1.01 (0.55 to 1.85) | 2 Studies | 3 Studies | 2 Studies | - | 2 Studies | |
| I2 =19.0% | I2 =0.0% | I2 =0.0% | I2 =0.0% | ||||
| 0.14 (–0.44 to 0.72) | –0.23 (–0.88 to 0.41) | –1.23 (–3.49 to 1.04) | –0.40 (–2.33 to 1.52) | ||||
| Sulfonylurea | 1.05 (0.70 to 1.60) | 1.04 (0.61 to 1.78) | 6 Studies | 6 Studies | - | - | |
| I2 =0.0% | I2 =0.0% | ||||||
| –0.02 (–0.53 to 0.49) | –0.15 (–0.41 to 0.11) | ||||||
| TZD | 0.86 (0.57 to 1.30) | 0.85 (0.48 to 1.52) | 0.82 (0.53 to 1.26) | 3 Studies | - | 1 Study | |
| I2 =0.0% | –0.42 (–4.34 to 3.51) | ||||||
| 0.27 (–1.65 to 2.20) | |||||||
| DPP-4 inhibitor | 0.93 (0.74 to 1.16) | 0.92 (0.50 to 1.66) | 0.88 (0.60 to 1.30) | 1.08 (0.70 to 1.65) | 3 Studies | 2 Studies | |
| I2 =0.0% | I2 =0.0% | ||||||
| –1.03 (–2.85 to 0.79) | –1.25 (–3.73 to 1.24) | ||||||
| SGLT-2 inhibitor | 0.81 (0.67 to 0.98)a | 0.80 (0.42 to 1.51) | 0.77 (0.48 to 1.21) | 0.94 (0.60 to 1.48) | 0.87 (0.65 to 1.16) | - | |
| GLP-1 agonist | 0.83 (0.68 to 1.02) | 0.82 (0.44 to 1.54) | 0.79 (0.50 to 1.25) | 0.97 (0.61 to 1.52) | 0.90 (0.67 to 1.20) | 1.03 (0.78 to 1.35) |
Traditional pairwise (upper right side) and network (lower left side) meta-analytic results are depicted for total stroke. Outcome of meta-analysis is expressed as effect size with 95% confidence intervals in the case of pairwise meta-analysis and 95% credible intervals in the case of network meta-analysis. For the pairwise meta-analysis, effect size of less than 0 indicate that the drug located in the column is safer. For the network meta-analysis, relative risks of less than 1 indicate that the drug located in the row is safer.
TZD, thiazolidinedione; DPP-4, dipeptidyl peptidase-4; SGLT-2, sodium-glucose cotransporter-2; GLP-1, glucagon-like peptide-1.
a It results indicate statistical significance. The total number of traditional pairwise studies was 83 trials due to two three arms studies and one four arms study.
- 1. Shi H, Ge Y, Wang H, Zhang Y, Teng W, Tian L. Fasting blood glucose and risk of stroke: a dose-response meta-analysis. Clin Nutr 2021;40:3296-304.ArticlePubMed
- 2. Forstermann U, Xia N, Li H. Roles of vascular oxidative stress and nitric oxide in the pathogenesis of atherosclerosis. Circ Res 2017;120:713-35.ArticlePubMed
- 3. Park SK, Jung JY, Kim MH, Oh CM, Ha E, Shin SS, et al. The association between changes in proteinuria and the risk of cerebral infarction in the Korean population. Diabetes Res Clin Pract 2022;192:110090.ArticlePubMed
- 4. American Diabetes Association Professional Practice Committee. 9. Pharmacologic approaches to glycemic treatment: standards of medical care in diabetes-2022. Diabetes Care 2022;45(Suppl 1):S125-43.ArticlePubMedPDF
- 5. Fei Y, Tsoi MF, Cheung BM. Cardiovascular outcomes in trials of new antidiabetic drug classes: a network meta-analysis. Cardiovasc Diabetol 2019;18:112.ArticlePubMedPMCPDF
- 6. Lee G, Oh SW, Hwang SS, Yoon JW, Kang S, Joh HK, et al. Comparative effectiveness of oral antidiabetic drugs in preventing cardiovascular mortality and morbidity: a network meta-analysis. PLoS One 2017;12:e0177646.ArticlePubMedPMC
- 7. Bloomgarden Z, Chilton R. Diabetes and stroke: an important complication. J Diabetes 2021;13:184-90.ArticlePubMedPDF
- 8. Ahn CH, Lim S. Effects of thiazolidinedione and new antidiabetic agents on stroke. J Stroke 2019;21:139-50.ArticlePubMedPMCPDF
- 9. Wilcox R, Bousser MG, Betteridge DJ, Schernthaner G, Pirags V, Kupfer S, et al. Effects of pioglitazone in patients with type 2 diabetes with or without previous stroke: results from PROactive (PROspective pioglitAzone Clinical Trial In macroVascular Events 04). Stroke 2007;38:865-73.ArticlePubMed
- 10. Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, Hantel S, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med 2015;373:2117-28.ArticlePubMed
- 11. Neal B, Perkovic V, Mahaffey KW, de Zeeuw D, Fulcher G, Erondu N, et al. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med 2017;377:644-57.ArticlePubMed
- 12. Wiviott SD, Raz I, Bonaca MP, Mosenzon O, Kato ET, Cahn A, et al. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med 2019;380:347-57.ArticlePubMed
- 13. Marso SP, Bain SC, Consoli A, Eliaschewitz FG, Jodar E, Leiter LA, et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med 2016;375:1834-44.ArticlePubMed
- 14. Marso SP, Daniels GH, Brown-Frandsen K, Kristensen P, Mann JF, Nauck MA, et al. Liraglutide and cardiovascular outcomes in type 2 diabetes. N Engl J Med 2016;375:311-22.ArticlePubMedPMC
- 15. Pfeffer MA, Claggett B, Diaz R, Dickstein K, Gerstein HC, Kober LV, et al. Lixisenatide in patients with type 2 diabetes and acute coronary syndrome. N Engl J Med 2015;373:2247-57.ArticlePubMed
- 16. Holman RR, Bethel MA, Mentz RJ, Thompson VP, Lokhnygina Y, Buse JB, et al. Effects of once-weekly exenatide on cardiovascular outcomes in type 2 diabetes. N Engl J Med 2017;377:1228-39.PubMedPMC
- 17. Hernandez AF, Green JB, Janmohamed S, D’Agostino RB Sr, Granger CB, Jones NP, et al. Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes): a double-blind, randomised placebo-controlled trial. Lancet 2018;392:1519-29.PubMed
- 18. Cornell JE. The PRISMA extension for network meta-analysis: bringing clarity and guidance to the reporting of systematic reviews incorporating network meta-analyses. Ann Intern Med 2015;162:797-8.ArticlePubMed
- 19. Higgins JP, Altman DG, Gotzsche PC, Juni P, Moher D, Oxman AD, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011;343:d5928.ArticlePubMedPMC
- 20. Palmer TM, Sterne JAC. Meta-analysis in Stata: an updated collection from the Stata Journal. College Station: Stata Press; 1998. Chapter 1, Metan: a command for meta-analysis in Stata. p. 3-28.
- 21. Sinning C, Makarova N, Volzke H, Schnabel RB, Ojeda F, Dorr M, et al. Association of glycated hemoglobin A1c levels with cardiovascular outcomes in the general population: results from the BiomarCaRE (Biomarker for Cardiovascular Risk Assessment in Europe) consortium. Cardiovasc Diabetol 2021;20:223.ArticlePubMedPMCPDF
- 22. Tsai WH, Chuang SM, Liu SC, Lee CC, Chien MN, Leung CH, et al. Effects of SGLT2 inhibitors on stroke and its subtypes in patients with type 2 diabetes: a systematic review and meta-analysis. Sci Rep 2021;11:15364.ArticlePubMedPMCPDF
- 23. Bhatt DL, Szarek M, Pitt B, Cannon CP, Leiter LA, McGuire DK, et al. Sotagliflozin in patients with diabetes and chronic kidney disease. N Engl J Med 2021;384:129-39.PubMed
- 24. Bhatt DL, Szarek M, Steg PG, Cannon CP, Leiter LA, McGuire DK, et al. Sotagliflozin in patients with diabetes and recent worsening heart failure. N Engl J Med 2021;384:117-28.ArticlePubMed
- 25. Cefalo CM, Cinti F, Moffa S, Impronta F, Sorice GP, Mezza T, et al. Sotagliflozin, the first dual SGLT inhibitor: current outlook and perspectives. Cardiovasc Diabetol 2019;18:20.ArticlePubMedPMCPDF
- 26. Bellastella G, Maiorino MI, Longo M, Scappaticcio L, Chiodini P, Esposito K, et al. Glucagon-like peptide-1 receptor agonists and prevention of stroke systematic review of cardiovascular outcome trials with meta-analysis. Stroke 2020;51:666-9.ArticlePubMed
- 27. Malhotra K, Katsanos AH, Lambadiari V, Goyal N, Palaiodimou L, Kosmidou M, et al. GLP-1 receptor agonists in diabetes for stroke prevention: a systematic review and meta-analysis. J Neurol 2020;267:2117-22.ArticlePubMedPDF
- 28. Gerstein HC, Hart R, Colhoun HM, Diaz R, Lakshmanan M, Botros FT, et al. The effect of dulaglutide on stroke: an exploratory analysis of the REWIND trial. Lancet Diabetes Endocrinol 2020;8:106-14.ArticlePubMed
- 29. Kalra S, Mukherjee JJ, Venkataraman S, Bantwal G, Shaikh S, Saboo B, et al. Hypoglycemia: the neglected complication. Indian J Endocrinol Metab 2013;17:819-34.ArticlePubMedPMC
- 30. Mijajlovic MD, Aleksic VM, Sternic NM, Mirkovic MM, Bornstein NM. Role of prediabetes in stroke. Neuropsychiatr Dis Treat 2017;13:259-67.ArticlePubMedPMCPDF
- 31. Ren X, Wang Z, Guo C. Long-term glycemic variability and risk of stroke in patients with diabetes: a meta-analysis. Diabetol Metab Syndr 2022;14:6.ArticlePubMedPMCPDF
- 32. Sun B, Luo Z, Zhou J. Comprehensive elaboration of glycemic variability in diabetic macrovascular and microvascular complications. Cardiovasc Diabetol 2021;20:9.ArticlePubMedPMCPDF
- 33. Lee H, Park SE, Kim EY. Glycemic variability impacted by SGLT2 inhibitors and GLP 1 agonists in patients with diabetes mellitus: a systematic review and meta-analysis. J Clin Med 2021;10:4078.ArticlePubMedPMC
- 34. Lee S, Lee H, Kim Y, Kim E. Effect of DPP-IV inhibitors on glycemic variability in patients with T2DM: a systematic review and meta-analysis. Sci Rep 2019;9:13296.ArticlePubMedPMCPDF
- 35. Kim K, Choi SH, Jang HC, Park YS, Oh TJ. Glucose profiles assessed by intermittently scanned continuous glucose monitoring system during the perioperative period of metabolic surgery. Diabetes Metab J 2022;46:713-21.ArticlePubMedPMCPDF
- 36. Seino H, Onishi Y, Naito Y, Komatsu M. Lixisenatide improves glycemic outcomes of Japanese patients with type 2 diabetes: a meta-analysis. Diabetol Metab Syndr 2016;8:36.ArticlePubMedPMC
- 37. Ferdinand KC, Izzo JL, Lee J, Meng L, George J, Salsali A, et al. Antihyperglycemic and blood pressure effects of empagliflozin in black patients with type 2 diabetes mellitus and hypertension. Circulation 2019;139:2098-109.ArticlePubMed
- 38. Ryder REJ, Abdul-Ghani MA, DeFronzo RA. Diabetes medications with cardiovascular protection: the likelihood of benefit from combination therapy increases further following new evidence during 2020. Br J Diabetes 2020;20:84-8.ArticlePDF
- 39. Bae JH, Park EG, Kim S, Kim SG, Hahn S, Kim NH. Comparative renal effects of dipeptidyl peptidase-4 inhibitors and sodium-glucose cotransporter 2 inhibitors on individual outcomes in patients with type 2 diabetes: a systematic review and network meta-analysis. Endocrinol Metab (Seoul) 2021;36:388-400.ArticlePubMedPMCPDF
- 40. Barkas F, Elisaf M, Tsimihodimos V, Milionis H. Dipeptidyl peptidase-4 inhibitors and protection against stroke: a systematic review and meta-analysis. Diabetes Metab 2017;43:1-8.ArticlePubMed
- 41. Aroda VR, Rosenstock J, Terauchi Y, Altuntas Y, Lalic NM, Morales Villegas EC, et al. PIONEER 1: randomized clinical trial of the efficacy and safety of oral semaglutide monotherapy in comparison with placebo in patients with type 2 diabetes. Diabetes Care 2019;42:1724-32.PubMed
- 42. Mosenzon O, Blicher TM, Rosenlund S, Eriksson JW, Heller S, Hels OH, et al. Efficacy and safety of oral semaglutide in patients with type 2 diabetes and moderate renal impairment (PIONEER 5): a placebo-controlled, randomised, phase 3a trial. Lancet Diabetes Endocrinol 2019;7:515-27.PubMed
- 43. Barkas F, Elisaf M, Milionis H. Protection against stroke with glucagon-like peptide 1 receptor agonists: a systematic review and meta-analysis. Eur J Neurol 2019;26:559-65.ArticlePubMedPDF
- 44. Sheahan KH, Wahlberg EA, Gilbert MP. An overview of GLP1 agonists and recent cardiovascular outcomes trials. Postgrad Med J 2020;96:156-61.ArticlePubMedPMCPDF
REFERENCES
Figure & Data
References
Citations
- SGLT2 Inhibitors and GLP-1 Agonists: A Beacon of Hope for Stroke Prevention in Diabetes
Jae-Han Jeon
Diabetes & Metabolism Journal.2024; 48(2): 213. CrossRef - Reply to comment on: Association of glucose-lowering drugs with incident stroke and transient ischaemic attacks in primary care patients with type 2 diabetes: disease analyser database
Wolfgang Rathmann, Karel Kostev
Acta Diabetologica.2024;[Epub] CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite- Figure
-

- Related articles
-
- Effectiveness of Resistance Exercise on Inflammatory Biomarkers in Patients with Type 2 Diabetes Mellitus: A Systematic Review with Meta-Analysis
- Effect of the Glucagon-Like Peptide-1 Receptor Agonists on Autonomic Function in Subjects with Diabetes: A Systematic Review and Meta-Analysis
- Effect of Different Types of Diagnostic Criteria for Gestational Diabetes Mellitus on Adverse Neonatal Outcomes: A Systematic Review, Meta-Analysis, and Meta-Regression
- Impact of COVID-19 Lockdown on the Metabolic Control Parameters in Patients with Diabetes Mellitus: A Systematic Review and Meta-Analysis



