
- Current
- Browse
- Collections
-
For contributors
- For Authors
- Instructions to authors
- Article processing charge
- e-submission
- For Reviewers
- Instructions for reviewers
- How to become a reviewer
- Best reviewers
- For Readers
- Readership
- Subscription
- Permission guidelines
- About
- Editorial policy
Articles
- Page Path
- HOME > Diabetes Metab J > Volume 36(1); 2012 > Article
-
Original ArticlePrevalence of Dyslipidemia among Korean Adults: Korea National Health and Nutrition Survey 1998-2005
- Myung Ha Lee1, Hyeon Chang Kim1,2, Song Vogue Ahn3, Nam Wook Hur1, Dong Phil Choi1, Chang Gyu Park4, Il Suh1
-
Diabetes & Metabolism Journal 2012;36(1):43-55.
DOI: https://doi.org/10.4093/dmj.2012.36.1.43
Published online: February 17, 2012
1Department of Preventive Medicine, Yonsei University College of Medicine, Seoul, Korea.
2Severance Institute for Vascular and Metabolic Research, Yonsei University College of Medicine, Seoul, Korea.
3Department of Preventive Medicine, Yonsei University Wonju College of Medicine, Wonju, Korea.
4Department of Cardiology, Cardiovascular Center, Korea University Guro Hospital, Seoul, Korea.
- Corresponding author: Hyeon Chang Kim. Department of Preventive Medicine, Yonsei University College of Medicine, 50 Yonsei-ro, Seodaemun-gu, Seoul 120-752, Korea. hckim@yuhs.ac
Copyright © 2012 Korean Diabetes Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Background
- Dyslipidemia is a disorder of lipid metabolism, including elevated total cholesterol, elevated triglyceride, elevated low density lipoprotein cholesterol (LDL-C), and decreased high density lipoprotein cholesterol (HDL-C). The objective of this study was to investigate recent changes in the prevalence of dyslipidemia and also the rates of awareness, treatment, and control of dyslipidemia among Korean adults.
-
Methods
- Dyslipidemia is defined according to the National Cholesterol Education Program-Adult Treatment Panel III as total cholesterol ≥240 mg/dL, LDL-C ≥160 mg/dL, HDL-C <40 mg/dL, and triglyceride ≥200 mg/dL. The prevalence of dyslipidemia was estimated for adults aged ≥20 years using the Korea National Health and Nutrition Survey (KNHANES) in 1998 (n=6,923), 2001 (n=4,882), and 2005 (n=5,323). Rates of awareness, treatment and control of dyslipidemia were calculated for adults aged ≥30 years using the KNHANES in 2005 (n=4,654).
-
Results
- The prevalence of dyslipidemia (aged ≥20 years) increased from 32.4% in 1998 to 42.6% in 2001 and 44.1% in 2005. Compared with the KNHANES in 1998, the prevalence of dyslipidemia was 47% (95% confidence interval [CI], 35% to 59%) higher in 2001 and 61% (95% CI, 49% to 75%) higher in 2005. In 2005, only 9.5% of people with dyslipidemia were aware of the disease, 5.2% used lipid-lowering medication, and 33.2% of patients with treatment reached treatment goals.
-
Conclusion
- The prevalence of dyslipidemia in Korea gradually increased between 1998 and 2005. These findings suggest that more intense efforts for the prevention and treatment of dyslipidemia may lead to further improvement in the management of dyslipidemia.
- Dyslipidemia means abnormal amount of lipids in the blood and its clinically important types include elevated total cholesterol, elevated triglycerides, elevated low density lipoprotein cholesterol (LDL-C), and decreased high density lipoprotein cholesterol (HDL-C) levels. Many previous studies have reported that dyslipidemia increases the risk of cardiovascular diseases [1-3]. Due to its asymptomatic nature and slow progression, it is difficult for individuals to notice or manage it. According to the 30-year follow-up study, a 10 mg/dL increase in total cholesterol was associated with 5% increase of total mortality and 9% increase of cardiovascular mortality [4]. Coronary heart disease and cerebrovascular disease caused twelve million deaths per year worldwide [5]. In South Korea, cerebrovascular disease, cardiovascular disease, and other circulatory diseases account for 20% of the total deaths and great disease burden as well [6,7]. However, there has not yet been a representative study that shows the prevalence of dyslipidemia in Korea. Thus we estimated the prevalence of dyslipidemia and its components among Korean adults based on the 1998, 2001, and 2005 Korean National Health and Nutrition Examination Survey (KNHANES) datasets. This study also investigated the rates of awareness, treatment, and control of dyslipidemia among Korean adults.
INTRODUCTION
- This study is based on the data obtained from the KNHANES, which is a nationwide survey examining the general health and nutrition status of the Korean people [8]. It consisted of four distinct surveys: the health interview survey, the health behavior survey, the health examination survey, and the nutrition survey. The KNHANES was conducted in 1998 (KNHANES I), 2001 (KNHANES II), and 2005 (KNHANES III). A stratified, multistage probability sampling design was used in KNHANES, and 42,780 individuals from 600 districts were chosen in consideration of location and residence-type in order to establish full representativeness of the whole nation. All 600 sampling districts were subject to the health interview and behavior surveys, and 200 districts of them (one third random sample) were subject to the health examination and nutrition surveys.
- The diagnosis of dyslipidemia was based on the presence of one or more of the following criteria, according to the criteria of the National Cholesterol Education Program Adult Treatment Panel III [9]. In the KNHANES I (year 1998) and II (year 2001), individuals were not asked about their blood lipid levels and management in the health interview survey because dyslipidemia was assumed to be very low in Korea. Thus dyslipidemia was defined solely based on the blood test results in the health examination in 1998 and 2001. But in 2005, dyslipidemia was determined with fasting blood tests as well as health interview survey data. Blood samples were collected in the morning after fasting for at least 8 hours and analyzed in the certified central laboratory on the same day. Serum total cholesterol, triglycerides, and HDL-C were measured by automated enzymatic techniques. LDL-C was calculated using the Friedewald's formula [10] in individuals with triglycerides <400 mg/dL. Therefore the definitions of dyslipidemia are as follows: In 1998 and 2001, total cholesterol levels over 240 mg/dL in the blood test results were defined as hypercholesterolemia, HDL-C levels under 40 mg/dL were defined as hypo-HDL-cholesterolemia, and triglyceride levels over 200 mg/dL were defined as hypertriglycemia. LDL-C levels over 160 mg/dL were defined as hyper-LDL-cholesterolemia. In 2005, hypo-HDL-cholesterolemia and hypertriglycemia were defined in the same way as they were in 1998 and 2001. Hypercholesterolemia was defined as the following three cases: 1) a total cholesterol level over 240 mg/dL from a blood test taken after fasting, or 2) the use of lipid-lowering drugs, or 3) when the subject has been diagnosed with dyslipidemia by a physician. Hyper-LDL-cholesterolemia was defined as: 1) an LDL-C level over 160 mg/dL, or 2) the use of lipid-lowering drugs, or 3) when the subject has been diagnosed with dyslipidemia by a physician (Table 1). The reason being, that despite the discrepancies in the definition of dyslipidemia by year, it is optimal for the definition to be accurate for each year. In the case of this study, the analysis was done excluding any measurements that were missing total cholesterol, HDL-C, or triglycerides. We analyzed subjects over 20 years old who participated in the health examination survey.
- The awareness rate of dyslipidemia, physician diagnosis rate, treatment rate, and control rate were defined using the health interview survey and the health examination survey results from KNHANES III (2005) only. The awareness rate is defined as the number of individuals whose response to the health interview survey indicated that they have had dyslipidemia in the past divided by the number of people with dyslipidemia, and the physician diagnosis rate is defined as the number of cases where individuals replied that they had been diagnosed by a physician out of those who are dyslipidemic. The treatment rate is defined based on individuals who had been diagnosed with dyslipidemia and had been taking lipid-lowering drugs, and the control rate is defined as individuals who had been diagnosed with dyslipidemia and had LDL-C levels under 160 mg/dL, HDL-C levels over 40 mg/dL, and triglyceride levels under 150 mg/dL.
- Statistical analysis
- For prevalence calculations, we used the stratification variables and sampling weights designated by the Korean Centers for Disease Control and Prevention, which were based on the sample design of each survey year. Prevalence of dyslipidemia was estimated in subjects over 20 and 30, and ages were classified into 10-year increments. The standardized prevalence and the numbers of cases of dyslipidemia were calculated by sex- and age-specific 2005 Korean population. In the table, the coefficients of variation over 30% were expressed as separate notations, and caution is required when interpreting corresponding values. For the purpose of comparison, the prevalence, diagnosis, and treatment rates in 1998 and 2001 were also adjusted to the age structure of the 2005 Korean population. Statistical analyses were performed using SAS version 9.2 (SAS Institute, Cary, NC, USA) and a P value of less than 0.05 was considered to be statistically significant. All statistical values generated in this research used the stratification variables used for sampling as well as weights, using the SAS survey procedure.
METHODS
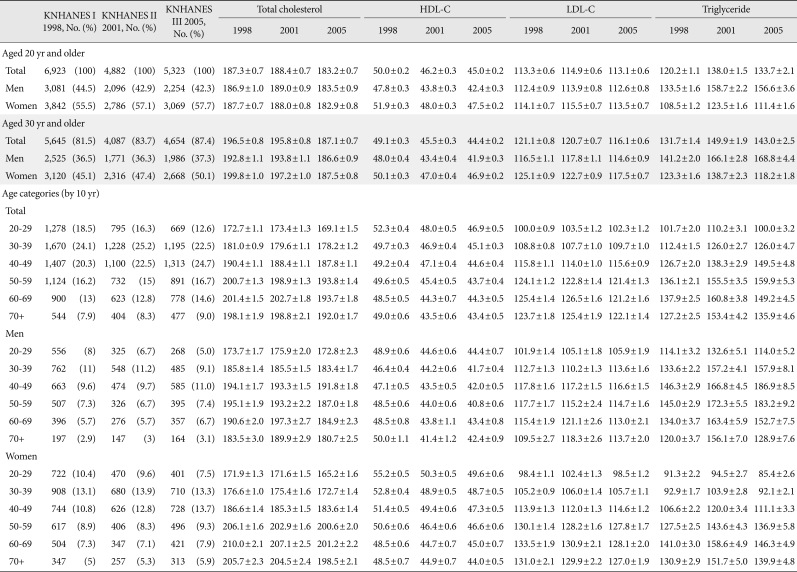
- The total numbers of subjects in this study were as follows: 6,923 in KNHANES I (1998), 4,882 in KNHANES II (2001), and 5,323 in KNHANES III (2005). The mean ages of the participants were 43.2, 45.8, and 43.4 years per survey year, respectively. The mean ages of male participants were 42.6, 46.0, and 42.6 years, respectively, and the mean ages of female participants were 43.7, 45.6, and 44.3 years.
- Lipoprotein distribution
- The mean values of total cholesterol, HDL-C, LDL-C, and triglycerides were presented for each survey year by gender according to age groups of 20+, 30+, and so on in 10-year increments (Table 2).
- Total cholesterol shows an increasing trend with age. Prior to age 50, the mean total cholesterol value in males is greater than in females. HDL-C decreases as age increases, but when examined by gender, is higher in females prior to age 50, although it is similar in males and females older than 50. LDL-C in males did not deviate far from the gender mean value, whereas as females age increases, the mean values showed an increasing trend. The mean triglyceride level in males was the highest between the ages of 40 to 59, and highest in females between the ages of 50 to 69. When considering only KNHANES III (2005), the average total cholesterol and LDL-C levels were 2 to 3 mg/dL lower in females than in males, and triglyceride levels were approximately 50 mg/dL lower in females. HDL-C was approximately 5 mg/dL higher in females than in males.
- Prevalence of dyslipidemia
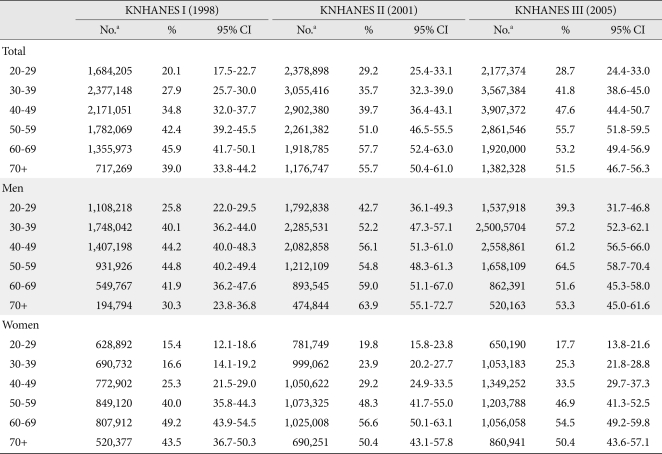
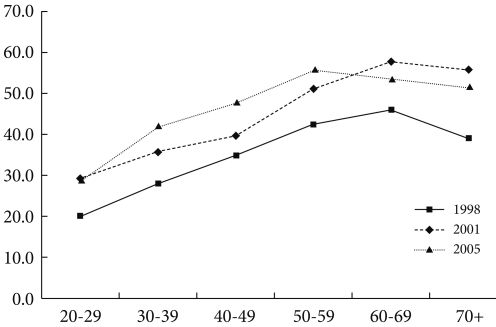
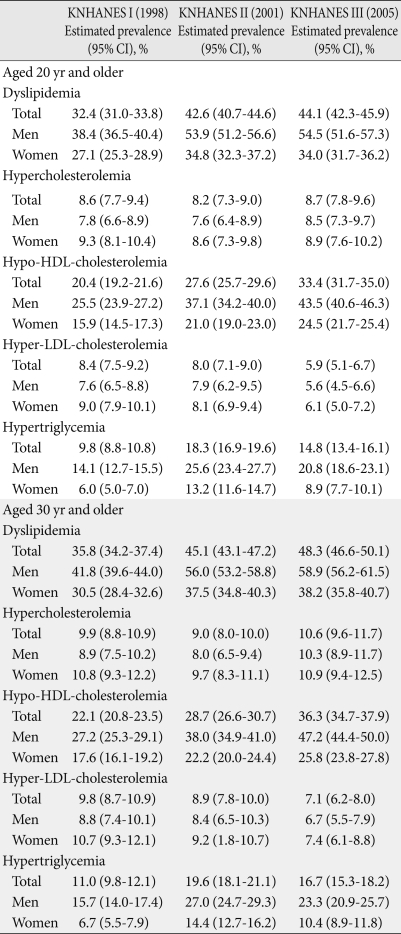
- The prevalence of dyslipidemia in adults over age 20 was 32.4% in 1998 (males, 38.4%; females, 27.1%), and increased greatly to 42.6% in 2011 (males, 53.9%; females, 34.8%). The prevalence was 44.1% in 2005 (males, 54.5%; females, 34.0%), which was a slight increase over the 2001 survey. The age-standardized prevalence in individuals older than 30 in 1998 was 35.8%, and 45.1% in 2001, which was a 9.3% increase within three years. In 2005, the age-standardized prevalence was 48.3%, which was 3.2% higher than in 2001. The prevalence of dyslipidemia was higher in males than in females (Table 3). A rapid increase in the prevalence of dyslipidemia in adults was observed in all age (Fig. 1).
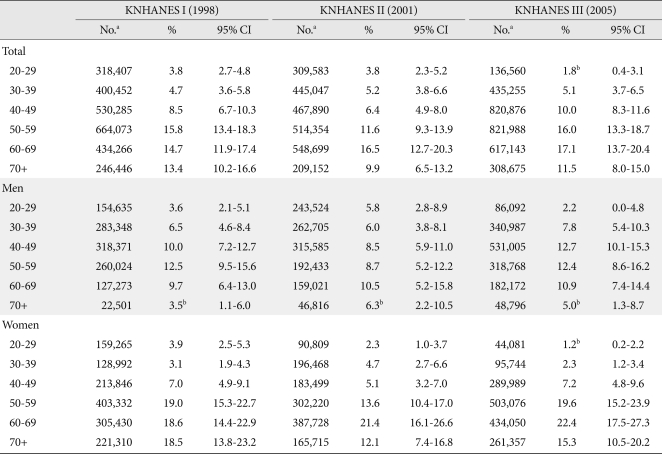
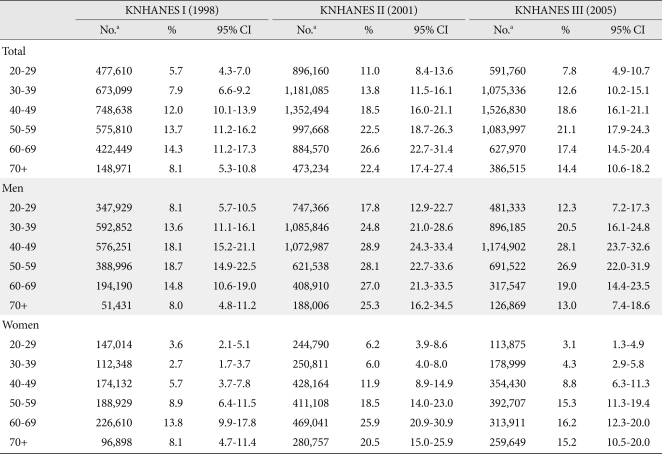
- The prevalence of hypercholesterolemia in adults over 20 years of age was 8.6%, 8.2%, and 8.7%, respectively, by survey year. The prevalence slightly decreased from 1998 to 2001 and then increased again. The prevalence of hypo-HDL-cholesterolemia gradually increased (20.4% in 1998, 27.6% in 2001, and 33.4% in 2005), but the prevalence in males was higher than in females in all surveys. The prevalence of hyper-LDL-cholesterolemia was 8.4% in 1998, 8.0% in 2001, and 5.9% in 2005. The prevalence of hyper-LDL-cholesterolemia was decreased from 1998 to 2005. This pattern was similar for both males and females. The prevalence of hypertriglycemia was 9.8%, 18.3%, and 14.8%, respectively; the prevalence increased from 1998 to 2001 and then began to decrease. In males, the prevalence of hypertriglycemia was 14.1%, 25.6%, and 20.8%, respectively, while those in females were 6.0%, 13.2%, and 8.9%. The results show that the prevalence was higher in males than in females (Table 3).
- The prevalence of dyslipidemia and the number of cases estimated by 2005 population are presented in the Appendix 1 to 5. When the results from the 2005 survey were examined, the prevalence of dyslipidemia in participants in their 20s was 28.7% and surged to 41.8% in participants in their 30s. Between the ages of 50 and 70+, more than half of those surveyed were reported to have dyslipidemia. As age increased for both males and females, an increasing trend in dyslipidemia was seen. The prevalence of dyslipidemia in males between the ages of 20 and 50 was nearly double the prevalence in females, although the prevalence was higher in females in the 60 to 70 age groups. In the age 70+ group, the prevalence in the male group was slightly higher than in female. The prevalence of hypercholesterolemia and hyper-LDL-cholesterolemia was higher in males until age 40 and higher in females after age 50. However, hypo-HDL-cholesterolemia and hypertriglycemia prevalence peaked in the 40 to 50 age range, after which a slight decreasing trend could be seen. In nearly all age groups, the prevalence of hypo-HDL cholesterolemia and hypertriglycemia was slightly higher in males (except females in their 60s). Among the components of dyslipidemia, the prevalence of hypo-HDL cholesterolemia was the highest, followed by hypertriglycemia, and the prevalence of hyper-LDL cholesterolemia was the lowest, around 7 percent.
- Age-standardized prevalence was 36.1% in 1998, 46.2% in 2001, and 48.4% in 2005. Compared with the prevalence from 1998, the prevalence in 2001 had increased by 1.47-fold (95% confidence interval [CI], 1.35 to 1.59), and in 2005 it had increased by 1.61-fold (95% CI, 1.49 to 1.75). Overtime, the prevalence of dyslipidemia tended to increase in both males and females, but the prevalence rate in males increased more quickly (Table 4).
- In the 2005 survey, awareness, physician diagnosis, treatment rate, and control rate in individuals over age 30 diagnosed with dyslipidemia were examined. The awareness rate, physician diagnosis rate, and treatment rate were slightly higher in females (Table 5). The control rate of dyslipidemia, when examined according to the presence of accompanying risk factors, was 56.3% in the 0 to 1 risk factors group, and 13.1% in the group with two or more risk factors (data not shown).
RESULTS
- In this study, the lipoprotein distribution and prevalence of dyslipidemia were estimated based on data from KNHANES conducted in 1998, 2001, and 2005. The yearly changes in the trends of prevalence were also analyzed. The prevalence of dyslipidemia in participants over age 20 was 32.4% in 1998, 42.6% in 2001, and 44.1% in 2005. The results also showed that the prevalence was higher in males than in females. The prevalence of dyslipidemia in males was 38.4%, 53.9%, and 54.5%, respectively, and 27.1%, 34.8%, and 34.0% in females, respectively.
- Dyslipidemia is the most manageable risk factor of atherosclerotic cardiovascular disease. The relationship between increased cholesterol and mortality rate due to coronary heart disease has been reported in numerous epidemiological studies [11,12]. A previous study reported that both total cholesterol and LDL-C increase total mortality rates [13]. According to a meta-analysis of several epidemiological studies, when HDL-C increased by 1.0 mg/dL, the occurrence of coronary heart disease decreased by 2% to 3% [14].
- In the KNHANES data analysis, hypo-HDL-cholesterolemia had the highest prevalence rate, followed by hypertriglycemia. The high HDL-C and triglyceride levels are thought to be caused by Korea's carbohydrate-centered diet [15] and are also correlated with a recent rapidly increased prevalence of obesity and type 2 diabetes. In particular, high triglyceride levels in diabetic patients are very common. In populations with high triglyceride levels, the incidence of cardiovascular disease is over two times higher compared to that in populations with normal levels [16]. In the KNHANES, the prevalence of hypertriglycemia in the normal glucose group was 6.7% and the prevalence of hypo-HDL-cholesterolemia was 30.7%, whereas in the impaired fasting glucose group, they were 14.9% and 42.4%, respectively, and in the diabetes group, they were 20.1% and 46.8% (P<0.0001).
- Based on the type of dyslipidemia, the risk of coronary artery disease differs between genders. LDL-C is the most indicative predicting factor in males, while HDL-C is the most indicative factor in females, while triglycerides are the second most indicative in both sexes [17,18]. The mean cholesterol concentration in females was lower than that in males in our analysis. However, there were more females with hypercholesterolemia with cholesterol concentrations over 240 mg/dL. One possible reason is that pre-menopausal females have lower lipid levels than males due to hormonal effects, but after menopause lipid levels rapidly increase and become similar or higher than that of males [19,20]. In the KNHANES III survey (2005), the prevalence of dyslipidemia increased with age. After the prevalence of dyslipidemia in males peaks in their 50s and in women in their 60s, it decreases slightly, and we observed that the onset of dyslipidemia occurs 10 years later in women than in men. Our analysis showed that more than half of the individuals aged 50+ had dyslipidemia. Yet, the awareness rate of dyslipidemia and the treatment rates are still low, and treatment is limited to hyper-LDL-cholesterolemia [21,22]. In this study, the prevalence of dyslipidemia continuously increases, especially first appearing in younger males in 20s and 30s. In order to prevent cardiovascular disease, it is necessary to educate, screen, and aggressively treat dyslipidemia in younger age subjects.
- The mortality rate of cardiovascular disease in Korea is still lower than that in the USA. When the actual distribution of lipoproteins by age and gender were compared with the United States, the mean total cholesterol levels of Korean above age 20 were lower. The LDL-C levels of Korean were also lower. However, triglyceride levels in Korean participants were higher than that of participants from the United States. HDL-C levels were lower in Koreans than in Americans. Especially, HDL-C and triglyceride levels in Korean females were much worse than in females from the United States [23]. In the USA, between 1960 and 2002, total cholesterol and LDL-C levels had continuously decreased due to ongoing efforts, and cardiovascular disease had decreased. However, triglyceride levels increased as a result of continuously increase in prevalence of diabetes and obesity [24]. Since Koreans have significantly higher triglyceride levels than Americans, proper management is urgent. In the USA, the prevalence of hypercholesterolemia (≥260 mg/dL) was 34.2% in males and 41.6% in females [23]. In recent years, total cholesterol decreased in the USA but still higher than in Koreans.
- In Japan, total cholesterol levels have increased by 5 mg/dL in the last 10 years. The total cholesterol levels in Japanese were 10 to 20 mg/dL higher than in Koreans in all age groups. However, LDL-C levels were similar, HDL-C was 14 mg/dL higher and triglyceride levels were 20 mg/dL lower in Japanese than in Koreans [25]. Since the definitions of hypercholesterolemia, hypertriglycemia, and dyslipidemia are not identical, care is needed when interpreting these results.
- Although it is based on a national representative survey, this study also has several limitations. First, this is a cross-sectional analysis and cannot investigate the factors affecting prevalence and management of dyslipidemia. Second, dyslipidemia was defined based on blood tests in 1998 and 2001, but was defined through an integration of blood tests, physician diagnosis and treatment in 2005. Differences in the definitions of dyslipidemia might affect the prevalence estimation and make direct comparisons difficult. Third, the health interview and the health behavior surveys were not consistent over time, and the treatment and control rates were estimated only in the 2005 survey.
- In conclusion, by analyzing datasets from the KNHANES conducted in 1998, 2001, and 2005, we observed an increase in the prevalence of dyslipidemia in Korea. In 2005, the prevalence approached nearly 50% of the adult population over age 30. The primary forms of dyslipidemia were hypo-HDL-cholesterolemia and hypertriglycemia. These findings suggest that more intense efforts are required to prevent from and control dyslipidemia in Korean adults.
DISCUSSION
-
Acknowledgements
- This study was supported by grants from the Korea Centers for Disease Control and Prevention (2006) and the Korea Healthcare Technology R&D Project of the Ministry of Health and Welfare, Republic of Korea (A102065).
ACKNOWLEDGMENTS
- 1. Castelli WP. The triglyceride issue: a view from Framingham. Am Heart J 1986;112:432-437. ArticlePubMed
- 2. Jee SH, Suh I, Kim IS, Appel LJ. Smoking and atherosclerotic cardiovascular disease in men with low levels of serum cholesterol: the Korea Medical Insurance Corporation Study. JAMA 1999;282:2149-2155. ArticlePubMed
- 3. Toth PP. Subclinical atherosclerosis: what it is, what it means and what we can do about it. Int J Clin Pract 2008;62:1246-1254. ArticlePubMedPMC
- 4. Anderson KM, Castelli WP, Levy D. Cholesterol and mortality. 30 years of follow-up from the Framingham study. JAMA 1987;257:2176-2180. ArticlePubMed
- 5. World Health Statistics 2009. World Health Organization cited 2010 Sep 30. Available from: http://www.who.int/whosis/whostat/2009/en/index.html.
- 6. Korea National Statistical Office. Annual report on the cause of death statistics, 2006. 2007. Daejeon: Korea National Statistical Office.
- 7. Lim SJ, Kim HJ, Nam CM, Chang HS, Jang YH, Kim S, Kang HY. Socioeconomic costs of stroke in Korea: estimated from the Korea national health insurance claims database. J Prev Med Public Health 2009;42:251-260. ArticlePubMed
- 8. Korea Health Industry Development Institute. Ministry of Health and Welfare. The Third Korea National Health and Nutrition Examination Survey (KNHANES III), 2005. 2006. Seoul: Ministry of Health and Welfare.
- 9. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001;285:2486-2497. ArticlePubMed
- 10. Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem 1972;18:499-502. ArticlePubMedPDF
- 11. Castelli WP. Cholesterol and lipids in the risk of coronary artery disease: the Framingham Heart Study. Can J Cardiol 1988;4(Suppl A):5A-10A. PubMed
- 12. Stamler J, Wentworth D, Neaton JD. Is relationship between serum cholesterol and risk of premature death from coronary heart disease continuous and graded? Findings in 356,222 primary screenees of the Multiple Risk Factor Intervention Trial (MRFIT). JAMA 1986;256:2823-2828. ArticlePubMed
- 13. Haim M, Benderly M, Brunner D, Behar S, Graff E, Reicher-Reiss H, Goldbourt U. Elevated serum triglyceride levels and long-term mortality in patients with coronary heart disease: the Bezafibrate Infarction Prevention (BIP) Registry. Circulation 1999;100:475-482. ArticlePubMed
- 14. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Summary of the second report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel II). JAMA 1993;269:3015-3023. ArticlePubMed
- 15. Song Y, Joung H. A traditional Korean dietary pattern and metabolic syndrome abnormalities. Nutr Metab Cardiovasc Dis Epub 2011 Jan 5. DOI: http://dx.doi.org/10.1016/j.numecd.2010.09.002.Article
- 16. Turner RC, Millns H, Neil HA, Stratton IM, Manley SE, Matthews DR, Holman RR. Risk factors for coronary artery disease in non-insulin dependent diabetes mellitus: United Kingdom Prospective Diabetes Study (UKPDS: 23). BMJ 1998;316:823-828. ArticlePubMedPMC
- 17. O'Brien T, Nguyen TT. Lipids and lipoproteins in women. Mayo Clin Proc 1997;72:235-244. ArticlePubMed
- 18. Barrett-Connor E, Bush TL. Estrogen replacement and coronary heart disease. Cardiovasc Clin 1989;19:159-172. PubMed
- 19. Jensen J, Nilas L, Christiansen C. Influence of menopause on serum lipids and lipoproteins. Maturitas 1990;12:321-331. ArticlePubMed
- 20. de Aloysio D, Gambacciani M, Meschia M, Pansini F, Bacchi Modena A, Bolis PF, Massobrio M, Maiocchi G, Peruzzi E. The Icarus Study Group. The effect of menopause on blood lipid and lipoprotein levels. Atherosclerosis 1999;147:147-153. ArticlePubMed
- 21. Korea Health Industry Development Institute. Ministry of Health and Welfare. Report on National Health and Nutrition Examination Survey, 1998. 1999. Seoul: Ministry of Health and Welfare.
- 22. Korea Health Industry Development Institute. Ministry of Health and Welfare. Report on National Health and Nutrition Examination Survey, 2001. 2002. Seoul: Ministry of Health and Welfare.
- 23. Ford ES, Mokdad AH, Giles WH, Mensah GA. Serum total cholesterol concentrations and awareness, treatment, and control of hypercholesterolemia among US adults: findings from the National Health and Nutrition Examination Survey, 1999 to 2000. Circulation 2003;107:2185-2189. ArticlePubMed
- 24. Carroll MD, Lacher DA, Sorlie PD, Cleeman JI, Gordon DJ, Wolz M, Grundy SM, Johnson CL. Trends in serum lipids and lipoproteins of adults, 1960-2002. JAMA 2005;294:1773-1781. ArticlePubMed
- 25. Arai H, Yamamoto A, Matsuzawa Y, Saito Y, Yamada N, Oikawa S, Mabuchi H, Teramoto T, Sasaki J, Nakaya N, Itakura H, Ishikawa Y, Ouchi Y, Horibe H, Kita T. Serum lipid survey and its recent trend in the general Japanese population in 2000. J Atheroscler Thromb 2005;12:98-106. ArticlePubMed
REFERENCES
Appendix
Prevalence of dyslipidemia in the KNHANES during 1998-2005 by age category
Prevalence of hypercholesterolemia in the KNHANES during 1998-2005 by age category
Prevalence of hypo-HDL-cholesterolemia in the KNHANES during 1998-2005 by age category

Prevalence of hyper-LDL cholesterolemia in the KNHANES during 1998-2005 by age category

Prevalence of hypertriglycemia in the KNHANES during 1998-2005 by age category

Values are presented as mean±standard deviation.
KNHANES, Korea National Health and Nutrition Examination Survey; HDL-C, high density lipoprotein cholesterol; LDL-C, low density lipoprotein cholesterol.
aMean values generated in this research used the stratification variables used for sampling as well as weights.


KNHANES, Korea National Health and Nutrition Examination Survey. aProportion of patients with awareness of the disease of all patients with dyslipidemia, bProportion of patients with previous diagnosis of all patients with dyslipidemia, cProportion of patients using lipid-lowering medication of all patients with dyslipidemia, dProportion of patients who achieved the treatment goal of all patients with dyslipidemia using lipid-lowering medication, eProportion of patients who achieved the treatment goal of all patients with hyper-LDL-cholesterolemia using lipid-lowering medication.
Figure & Data
References
Citations
- Association between weekend catch-up sleep and dyslipidemia among Korean workers
Ye Seul Jang, Yu Shin Park, Kyungduk Hurh, Eun-Cheol Park, Sung-In Jang
Scientific Reports.2023;[Epub] CrossRef - Effects of ambient particulate exposure on blood lipid levels in hypertension inpatients
Yanfang Gao, Chenwei Li, Lei Huang, Kun Huang, Miao Guo, Xingye Zhou, Xiaokang Zhang
Frontiers in Public Health.2023;[Epub] CrossRef - Association between ambient air pollutants and lipid profile: A systematic review and meta-analysis
Chun Wang, Xing-chen Meng, Chao Huang, Jia Wang, Ying-hao Liao, Yang Huang, Ran Liu
Ecotoxicology and Environmental Safety.2023; 262: 115140. CrossRef - Lipoproteins, Cholesterol, and Atherosclerotic Cardiovascular Disease in East Asians and Europeans
Takahito Doi, Anne Langsted, Børge G. Nordestgaard
Journal of Atherosclerosis and Thrombosis.2023; 30(11): 1525. CrossRef - Associations between the Genetic Heritability of Dyslipidemia and Dietary Patterns in Korean Adults Based on Sex Differences
Sei Kim, Hye Kyung Jeon, Gyeonghee Lee, Youbin Kim, Hae Young Yoo
Nutrients.2023; 15(20): 4385. CrossRef - Periodontitis is a factor associated with dyslipidemia
Isaac Suzart Gomes‐Filho, Michelle Teixeira Oliveira, Simone Seixas da Cruz, Eneida de Moraes Marcílio Cerqueira, Soraya Castro Trindade, Graciete Oliveira Vieira, Paulo Henrique Couto Souza, Luis Fernando Fernandes Adan, Alexandre Marcelo Hintz, Johelle
Oral Diseases.2022; 28(3): 813. CrossRef - Association of PM2.5 With blood lipids and dyslipidaemia in a rural population of north-western china
Kairong Wang, Yi Zhao, Qingan Wang, Yajuan Zhang, Yuhong Zhang
Frontiers in Environmental Science.2022;[Epub] CrossRef - The association between ambient air pollution and blood lipids: A longitudinal study in Shijiazhuang, China
Kaihua Zhang, Haoyuan Wang, Weiliang He, Gongbo Chen, Peng Lu, Rongbin Xu, Pei Yu, Tingting Ye, Suying Guo, Shanshan Li, Yinyu Xie, Zhihua Hao, Hebo Wang, Yuming Guo
Science of The Total Environment.2021; 752: 141648. CrossRef - The association between periodontitis and dyslipidemia according to smoking and harmful alcohol use in a representative sample of Korean adults
Su-Jin Han, Yeo Jin Yi, Kwang-Hak Bae
Clinical Oral Investigations.2020; 24(2): 937. CrossRef - Factors Associated with Awareness, Treatment, and Control Rate of Hypertension among Korean Young Adults Aged 30–49 Years
Yong Woo Jeon, Hyeon Chang Kim
Korean Circulation Journal.2020; 50(12): 1077. CrossRef - Efficacy and Safety of Omega-3 Fatty Acids in Patients Treated with Statins for Residual Hypertriglyceridemia: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial
Ji Eun Jun, In-Kyung Jeong, Jae Myung Yu, Sung Rae Kim, In Kye Lee, Kyung-Ah Han, Sung Hee Choi, Soo-Kyung Kim, Hyeong Kyu Park, Ji-Oh Mok, Yong-ho Lee, Hyuk-Sang Kwon, So Hun Kim, Ho-Cheol Kang, Sang Ah Lee, Chang Beom Lee, Kyung Mook Choi, Sung-Ho Her,
Diabetes & Metabolism Journal.2020; 44(1): 78. CrossRef - Prevalencia de hipertrigliceridemia en adultos y factores cardiometabólicos asociados. Estudio SIMETAP-HTG
Antonio Ruiz-García, Ezequiel Arranz-Martínez, Beatriz López-Uriarte, Montserrat Rivera-Teijido, David Palacios-Martínez, Gema M. Dávila-Blázquez, Antonio Rosillo-González, José Antonio González-Posada Delgado, José Enrique Mariño-Suárez, Enrique Revilla-
Clínica e Investigación en Arteriosclerosis.2020; 32(6): 242. CrossRef - Long-term effects of ambient air pollutants to blood lipids and dyslipidemias in a Chinese rural population
Shuyuan Mao, Gongbo Chen, Feifei Liu, Na Li, Chongjian Wang, Yisi Liu, Suyang Liu, Yuanan Lu, Hao Xiang, Yuming Guo, Shanshan Li
Environmental Pollution.2020; 256: 113403. CrossRef - Prevalence of hypertriglyceridemia in adults and related cardiometabolic factors. SIMETAP-HTG study
Antonio Ruiz-García, Ezequiel Arranz-Martínez, Beatriz López-Uriarte, Montserrat Rivera-Teijido, David Palacios-Martínez, Gema M. Dávila-Blázquez, Antonio Rosillo-González, José Antonio González-Posada Delgado, José Enrique Mariño-Suárez, Enrique Revilla-
Clínica e Investigación en Arteriosclerosis (English Edition).2020; 32(6): 242. CrossRef - Long-term effects of various types of 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitors on changes in glomerular filtration rate in Korea
Seo Yeon Baik, Hyunah Kim, So Jung Yang, Tong Min Kim, Seung-Hwan Lee, Jae Hyoung Cho, Hyunyong Lee, Hyeon Woo Yim, Kun-Ho Yoon, Hun-Sung Kim
Frontiers of Medicine.2019; 13(6): 713. CrossRef - The association between low frequency of having breakfast and dyslipidemia in South Korean men and women
Doo Woong Lee, Dong-Woo Choi, Yeong Jun Ju, Sang Ah Lee, Eun-Cheol Park
European Journal of Clinical Nutrition.2019; 73(6): 896. CrossRef - Association between Brachial-Ankle Pulse Wave Velocity and Microalbuminuria and to Predict the Risk for the Development of Microalbuminuria Using Brachial-Ankle Pulse Wave Velocity Measurement in Type 2 Diabetes Mellitus Patients
Byong-Kyu Kim, Dilaram Acharya, Deuk-Young Nah, Moo-Yong Rhee, Seok-Ju Yoo, Kwan Lee
Healthcare.2019; 7(4): 111. CrossRef - A genome-wide search for gene-by-obesity interaction loci of dyslipidemia in Koreans shows diverse genetic risk alleles
Moonil Kang, Joohon Sung
Journal of Lipid Research.2019; 60(12): 2090. CrossRef - Oily Fish Consumption and the Risk of Dyslipidemia in Korean Adults: A Prospective Cohort Study Based on the Health Examinees Gem (HEXA-G) Study
Seong-Ah Kim, Jong-koo Lee, Daehee Kang, Sangah Shin
Nutrients.2019; 11(10): 2506. CrossRef - Dyslipidemia: Genetics, lipoprotein lipase and HindIII polymorphism
Marcos Palacio Rojas, Carem Prieto, Valmore Bermúdez, Carlos Garicano, Trina Núñez Nava, María Sofía Martínez, Juan Salazar, Edward Rojas, Arturo Pérez, Paulo Marca Vicuña, Natalia González Martínez, Santiago Maldonado Parra, Kyle Hoedebecke, Rosanna D’Ad
F1000Research.2018; 6: 2073. CrossRef - Prevalence of dyslipidemia and achievement of low-density lipoprotein cholesterol targets in Chinese adults: A nationally representative survey of 163,641 adults
Mei Zhang, Qian Deng, Linhong Wang, Zhengjing Huang, Maigeng Zhou, Yichong Li, Zhenping Zhao, Yawei Zhang, Limin Wang
International Journal of Cardiology.2018; 260: 196. CrossRef - Change in ALT levels after administration of HMG‐CoA reductase inhibitors to subjects with pretreatment levels three times the upper normal limit in clinical practice
Hyunah Kim, Hyeseon Lee, Tong Min Kim, So Jung Yang, Seo Yeon Baik, Seung‐Hwan Lee, Jae‐Hyoung Cho, Hyunyong Lee, Hyeon Woo Yim, In Young Choi, Kun‐Ho Yoon, Hun‐Sung Kim
Cardiovascular Therapeutics.2018;[Epub] CrossRef - Evaluating the prevalence, awareness, and control of hypertension, diabetes, and dyslipidemia in Korea using the NHIS-NSC database
Sunjoo Boo, Young Joo Yoon, Hyunjin Oh
Medicine.2018; 97(51): e13713. CrossRef - Prevalence of Metabolic Syndrome and Associations with Lipid Profiles in Iranian Men: A Population-Based Screening Program
Abolfazl Mohammadbeigi, Hamid Farahani, Esmail Moshiri, Mahbobeh Sajadi, Robabeh Ahmadli, Sima Afrashteh, Salman Khazaei, Hossein Ansari
The World Journal of Men's Health.2018; 36(1): 50. CrossRef - Association of change in waist circumference and dyslipidaemia risk: The rural Chinese cohort study
Junmei Zhou, Yongcheng Ren, Chongjian Wang, Linlin Li, Lu Zhang, Bingyuan Wang, Yang Zhao, Chengyi Han, Hongyan Zhang, Xiangyu Yang, Xinping Luo, Chao Pang, Lei Yin, Tianping Feng, Jingzhi Zhao, Dongsheng Hu, Ming Zhang
Diabetes/Metabolism Research and Reviews.2018;[Epub] CrossRef - Association between triglyceride/high-density lipoprotein ratio and hearing impairment in a Korean population
Da Jung Jung, Jun Young Do, Kyu Hyang Cho, A. Young Kim, Seok Hui Kang
Postgraduate Medicine.2017; 129(8): 943. CrossRef - Association of Body Mass Index with Dyslipidemia among the Government Staff of Kermanshah, Iran: A Cross-Sectional Study
Ebrahim Shakiba, Nahid Khademi, Malihe Khoramdad, Yousef Alimohamadi, Neda Izadi
Iranian Red Crescent Medical Journal.2017;[Epub] CrossRef - The differences in the incidence of diabetes mellitus and prediabetes according to the type of HMG-CoA reductase inhibitors prescribed in Korean patients
Tong Min Kim, Hyunah Kim, Yoo Jin Jeong, Sun Jung Baik, So Jung Yang, Seung-Hwan Lee, Jae-Hyoung Cho, Hyunyong Lee, Hyeon Woo Yim, In Young Choi, Kun-Ho Yoon, Hun-Sung Kim
Pharmacoepidemiology and Drug Safety.2017; 26(10): 1156. CrossRef - Analysis and comparison of the cost-effectiveness of statins according to the baseline low-density lipoprotein cholesterol level in Korea
Y. J. Jeong, H. Kim, S. J. Baik, T. M. Kim, S. J. Yang, S.-H. Lee, J.-H. Cho, H. Lee, H. W. Yim, I. Y. Choi, K.-H. Yoon, H.-S. Kim
Journal of Clinical Pharmacy and Therapeutics.2017; 42(3): 292. CrossRef - Changes over time in the prevalence and treatment of cardiovascular risk factors, and contributions to time trends in coronary mortality over 25 years in the Lille urban area (northern France)
Guillaume Clement, Jonathan Giovannelli, Dominique Cottel, Michele Montaye, Alina Ciuchete, Jean Dallongeville, Philippe Amouyel, Luc Dauchet
Archives of Cardiovascular Diseases.2017; 110(12): 689. CrossRef - Early Postpartum Lipid Profile in Women with and Without Gestational Diabetes Mellitus: Results of a Prospective Cohort Study
Sedigheh Nouhjah, Hajieh Shahbazian, Shayesteh Jahanfar, Nahid Shahbazian, Alireza Jahanshahi, Bahman Cheraghian, Leila Hardanipasand, Mitra Moradi
Iranian Red Crescent Medical Journal.2017;[Epub] CrossRef - Dyslipidemia: Genetics, lipoprotein lipase and HindIII polymorphism
Marcos Palacio Rojas, Carem Prieto, Valmore Bermúdez, Carlos Garicano, Trina Núñez Nava, María Sofía Martínez, Juan Salazar, Edward Rojas, Arturo Pérez, Paulo Marca Vicuña, Natalia González Martínez, Santiago Maldonado Parra, Kyle Hoedebecke, Rosanna D’Ad
F1000Research.2017; 6: 2073. CrossRef - Self‐perceived health versus actual cardiovascular disease risks
Young Ko, Sunjoo Boo
Japan Journal of Nursing Science.2016; 13(1): 65. CrossRef - Hypertriglyceridemia and Cardiovascular Diseases: Revisited
Seung Hwan Han, Stephen J Nicholls, Ichiro Sakuma, Dong Zhao, Kwang Kon Koh
Korean Circulation Journal.2016; 46(2): 135. CrossRef - One-Year Experience Managing a Cancer Survivorship Clinic Using a Shared-Care Model for Gastric Cancer Survivors in Korea
Ji Eun Lee, Dong Wook Shin, Hyejin Lee, Ki Young Son, Warrick Junsuk Kim, Yun-Suhk Suh, Seong-Ho Kong, Hyuk Joon Lee, Belong Cho, Han-Kwang Yang
Journal of Korean Medical Science.2016; 31(6): 859. CrossRef - Relationship Between Dyslipidemia and Albuminuria in Hypertensive Adults
Sung-Ho Lee, Do Hoon Kim, Yang-Hyun Kim, Yong Kyun Roh, Sang Yhun Ju, Hyo-Yun Nam, Ga-Eun Nam, Jun-Seok Choi, Jong-Eun Lee, Jung-Eun Sang, Kyungdo Han, Yong-Gyu Park
Medicine.2016; 95(16): e3224. CrossRef - Epidemiology of dyslipidemia in Korea
Hyeon Chang Kim
Journal of the Korean Medical Association.2016; 59(5): 352. CrossRef - Effects of Age, Sex, and Menopausal Status on Blood Cholesterol Profile in the Korean Population
Ji Hye Park, Myung Ha Lee, Jee-Seon Shim, Dong Phil Choi, Bo Mi Song, Seung Won Lee, Hansol Choi, Hyeon Chang Kim
Korean Circulation Journal.2015; 45(2): 141. CrossRef - Related factors of medication adherence in patients with dyslipidemia: The 2010-2012 Korean National Health and Nutrition Examination Survey
Eun Jung Cho, Kyoung Ja Moon
Korean Journal of Health Education and Promotion.2015; 32(2): 65. CrossRef - Dyslipidemia Prevalence in Iranian Adult Men: The Impact of Population-Based Screening on the Detection of Undiagnosed Patients
Abolfazl Mohammadbeigi, Esamil Moshiri, Narges Mohammadsalehi, Hossein Ansari, Ali Ahmadi
The World Journal of Men's Health.2015; 33(3): 167. CrossRef - Nicotinic acid and derivatives as multifunctional pharmacophores for medical applications
Nujarin Sinthupoom, Veda Prachayasittikul, Supaluk Prachayasittikul, Somsak Ruchirawat, Virapong Prachayasittikul
European Food Research and Technology.2015; 240(1): 1. CrossRef - Relationship between dyslipidemia and albuminuria in prediabetic adults: The Korea National Health and Nutrition Examination Survey 2011–2012
Ga Eun Nam, Kyungdo Han, Do Hoon Kim, Yong Gyu Park, Yeo Joon Yoon, Young Eun Kim, Sangsu Lee, Sungho Lee, Yong Kyun Roh
Endocrine.2015; 48(2): 557. CrossRef - Trends in lipid profiles among South Korean adults: 2005, 2008 and 2010 Korea National Health and Nutrition Examination Survey
Ga Eun Nam, Kyungdo Han, Yong Gyu Park, Youn Seon Choi, Seon Mee Kim, Sang-Yhun Ju, Byung-Joon Ko, Yang Hyun Kim, Eun Hye Kim, Kyung Hwan Cho, Do Hoon Kim
Journal of Public Health.2015; 37(2): 286. CrossRef - Subclinical Hypothyroidism Might Worsen the Effects of Aging on Serum Lipid Profiles: A Population-Based Case-Control Study
Meng Zhao, Tao Yang, Li Chen, Xulei Tang, Qingbo Guan, Bingchang Zhang, Xu Zhang, Haiqing Zhang, Chenggang Wang, Jin Xu, Xinguo Hou, Qiu Li, Chunxiao Yu, Yuanfei Zhao, Li Fang, Zhongshang Yuan, Fuzhong Xue, Guang Ning, Ling Gao, Chao Xu, Jiajun Zhao
Thyroid.2015; 25(5): 485. CrossRef - Serum lipid profiles and glycemic control in adolescents and young adults with type 1 diabetes mellitus
Shin-Hee Kim, In-Ah Jung, Yeon Jin Jeon, Won Kyoung Cho, Kyoung Soon Cho, So Hyun Park, Min Ho Jung, Byoung Kyu Suh
Annals of Pediatric Endocrinology & Metabolism.2014; 19(4): 191. CrossRef - Dyslipidemia in Children and Adolescents: When and How to Diagnose and Treat?
Jung Min Yoon
Pediatric Gastroenterology, Hepatology & Nutrition.2014; 17(2): 85. CrossRef - Sarcopenia and sarcopenic obesity and their association with dyslipidemia in Korean elderly men: the 2008–2010 Korea National Health and Nutrition Examination Survey
S. J. Baek, G. E. Nam, K. D. Han, S. W. Choi, S. W. Jung, A. R. Bok, Y. H. Kim, K. S. Lee, B. D. Han, D. H. Kim
Journal of Endocrinological Investigation.2014; 37(3): 247. CrossRef - Association between Blood Lipid Levels and Personality Traits in Young Korean Women
Seung-Ju Roh, Han-Na Kim, Unjin Shim, Bo-Hye Kim, Su-Jin Kim, Hye Won Chung, Hyejin Lee, Yeon-Ah Sung, Hyung-Lae Kim, Christina Bursill
PLoS ONE.2014; 9(9): e108406. CrossRef - Serum Cholesterol Concentration and Prevalence, Awareness, Treatment, and Control of High Low‐Density Lipoprotein Cholesterol in the Korea National Health and Nutrition Examination Surveys 2008–2010: Beyond the Tip of the Iceberg
Yong‐ho Lee, Sang‐Guk Lee, Myung Ha Lee, Jeong‐Ho Kim, Byung‐Wan Lee, Eun Seok Kang, Hyun Chul Lee, Bong Soo Cha
Journal of the American Heart Association.2014;[Epub] CrossRef - Prevalence of plasma lipid abnormalities and its association with glucose metabolism in Spain: The di@bet.es study
Sergio Martinez-Hervas, Rafael Carmena, Juan F. Ascaso, Jose T. Real, Luis Masana, Miguel Catalá, Joan Vendrell, José Antonio Vázquez, Sergio Valdés, Inés Urrutia, Federico Soriguer, Manuel Serrano-Rios, Gemma Rojo-Martínez, Gemma Pascual-Manich, Emilio O
Clínica e Investigación en Arteriosclerosis.2014; 26(3): 107. CrossRef - The current state of dyslipidemia in Korean children and adolescents and its management in clinical practice
Jung Sub Lim
Annals of Pediatric Endocrinology & Metabolism.2013; 18(1): 1. CrossRef - Prevalence and Management of Dyslipidemia in Korea: Korea National Health and Nutrition Examination Survey during 1998 to 2010
Eun Roh, Seung-Hyun Ko, Hyuk-Sang Kwon, Nan Hee Kim, Jae Hyeon Kim, Chul Sik Kim, Kee-Ho Song, Jong Chul Won, Dae Jung Kim, Sung Hee Choi, Soo Lim, Bong-Yun Cha
Diabetes & Metabolism Journal.2013; 37(6): 433. CrossRef - Socioeconomic status and dyslipidemia in Korean adults: The 2008–2010 Korea National Health and Nutrition Examination Survey
Ga Eun Nam, Kyung Hwan Cho, Yong Gyu Park, Kyung Do Han, Youn Seon Choi, Seon Mee Kim, Kyung Shik Lee, Byung Joon Ko, Yang Hyun Kim, Byoung Duck Han, Do Hoon Kim
Preventive Medicine.2013; 57(4): 304. CrossRef - The association between periodontitis and dyslipidemia based on the fourth Korea National Health and Nutrition Examination Survey
Jun‐Beom Lee, Hee‐Yong Yi, Kwang‐Hak Bae
Journal of Clinical Periodontology.2013; 40(5): 437. CrossRef - Trends in Cardiovascular Health Metrics among Korean Adults
Hae-Joon Lee, Beomseok Suh, Tae-Gon Yoo, Haewon Lee, Dong Wook Shin
Korean Journal of Family Medicine.2013; 34(6): 403. CrossRef - Increasing achievement of the target goals for glycemic, blood pressure and lipid control for adults with diagnosed diabetes in Korea
Sung Hoon Yu, Jun Goo Kang, Yoo‐Cheol Hwang, Kyu Jeung Ahn, Hyung Joon Yoo, Hong Yup Ahn, Sung Woo Park, Cheol‐Young Park
Journal of Diabetes Investigation.2013; 4(5): 460. CrossRef - Low bone mineral density is associated with dyslipidemia in South Korean men: The 2008–2010 Korean National Health and Nutrition Examination Survey
Yang-Hyun Kim, Ga-Eun Nam, Kyung-Hwan Cho, Youn Seon Choi, Seon-Mee Kim, Byung-Duck Han, Kyung Do Han, Kyung-Shik Lee, Chang-Hae Park, Do-Hoon Kim
Endocrine Journal.2013; 60(10): 1179. CrossRef - Response: Prevalence of Dyslipidemia among Korean Adults: Korea National Health and Nutrition Survey 1998-2005 (Diabetes Metab J 2012;36:43-55)
Hyeon Chang Kim
Diabetes & Metabolism Journal.2012; 36(2): 165. CrossRef - Beyond the Shadow: Getting Past the Veil of Nonadherence in the Management of Atherosclerotic Risk Factors
Ross D. Feldman, Tavis S. Campbell
Canadian Journal of Cardiology.2012; 28(5): 531. CrossRef - Letter: Prevalence of Dyslipidemia among Korean Adults: Korea National Health and Nutrition Survey 1998-2005 (Diabetes Metab J 2012;36:43-55)
Bo Kyung Koo
Diabetes & Metabolism Journal.2012; 36(2): 163. CrossRef
 PubReader
PubReader Cite
Cite



