- Current
- Browse
- Collections
-
For contributors
- For Authors
- Instructions to authors
- Article processing charge
- e-submission
- For Reviewers
- Instructions for reviewers
- How to become a reviewer
- Best reviewers
- For Readers
- Readership
- Subscription
- Permission guidelines
- About
- Editorial policy
Articles
- Page Path
- HOME > Diabetes Metab J > Volume 45(2); 2021 > Article
-
Original ArticleMetabolic Risk/Epidemiology Effect of Sarcopenia and Body Shape on Cardiovascular Disease According to Obesity Phenotypes
-
Hyun-Woong Cho1*
 , Wankyo Chung2,3*, Shinje Moon1, Ohk-Hyun Ryu1, Min Kyung Kim1, Jun Goo Kang1
, Wankyo Chung2,3*, Shinje Moon1, Ohk-Hyun Ryu1, Min Kyung Kim1, Jun Goo Kang1 -
Diabetes & Metabolism Journal 2021;45(2):209-218.
DOI: https://doi.org/10.4093/dmj.2019.0223
Published online: July 10, 2020
1Division of Endocrinology and Metabolism, Hallym University College of Medicine, Chuncheon, Korea
2Department of Public Health Science, Graduate School of Public Health, Seoul National University, Seoul, Korea
3Institute of Health and Environment, Seoul National University, Seoul, Korea
-
Corresponding author: Jun Goo Kang Division of Endocrinology and Metabolism, Hallym University College of Medicine,1 Hallimdaehak-gil, Chuncheon 24252, Korea. kjg0804@empas.com
-
Corresponding author: Min Kyung Kim Division of Endocrinology and Metabolism, Hallym University College of Medicine, 1 Hallimdaehak-gil, Chuncheon 24252, Korea. mkkim83@kdh.or.kr
- *Hyun-Woong Cho and Wankyo Chung contributed equally to this study as first authors.
Copyright © 2021 Korean Diabetes Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Background
- This study aimed to assess the effects of sarcopenia and A Body Shape Index (ABSI) on cardiovascular disease (CVD) risk according to obesity phenotypes.
-
Methods
- We used data from the National Health and Nutrition Examination Survey 1999 to 2012. A total of 25,270 adults were included and classified into the following groups: metabolically healthy normal weight (MHNW), metabolically healthy overweight/obese (MHO), metabolically unhealthy normal weight (MUNW), and metabolically unhealthy overweight/obese (MUO). Sarcopenia was defined as the appendicular skeletal mass index <7 kg/m2 in men and <5.5kg/m2 in women. A multivariate logistic regression analysis was performed to evaluate the odds ratio (OR) of sarcopenia and ABSI for CVD events according to the obesity phenotype.
-
Results
- The MHNW participants with sarcopenia had higher risk for CVD than those without sarcopenia (OR, 2.69; 95% confidence interval [CI], 1.56 to 4.64). In the analysis with MHNW participants without sarcopenia as a reference, the participants with sarcopenia showed a higher OR for CVD than those without sarcopenia in both MHO (OR in participants without sarcopenia, 3.31; 95% CI, 1.94 to 5.64) (OR in participants with sarcopenia, 8.59; 95% CI, 2.63 to 28.04) and MUO participants (OR in participants without sarcopenia, 5.11; 95% CI, 3.21 to 8.15) (OR in participants with sarcopenia, 8.12; 95% CI, 4.04 to 16.32). Participants within the second and third tertiles of ABSI had higher ORs for CVDs than the counterpart of obesity phenotypes within the first tertile.
-
Conclusion
- These results suggest that clinical approaches that consider muscle and body shape are required.
- Obesity remains a leading cause of type 2 diabetes mellitus (DM), cardiovascular diseases (CVDs), and stroke and has substantially increased the public health burden [1234]. To evaluate obesity accurately, direct fat mass measurement should be performed with computed tomography, magnetic resonance imaging, whole body dual-energy X-ray absorptiometry (DXA), or positron emission tomography-computed tomography [5]; however, direct measurements such as these are expensive and require modalities with limited availability in the clinical setting. Therefore, body mass index (BMI) has traditionally been used for the classification of obesity. However, one limitation of this method is that it cannot distinguish muscle from fat [6]. Recently, a number of studies found that low muscle mass; i.e., sarcopenia, was also associated with CVD [7]. Furthermore, epidemiologic studies suggested that a combination of sarcopenia and obesity has been associated with CVD and mortality [7].
- Although obesity is usually associated with cardio-metabolic risk factors, not all obese individuals develop metabolic dysfunction. For example, some have a metabolically healthy overweight/obese (MHO) phenotype. While a recent meta-analysis of 19 studies showed that individuals with MHO were at a high risk of CVD, nine of studies did not produce statistically significant results [8] and the exact mechanism regarding this phenomenon remains unclear. Therefore, the inability of BMI to distinguish between fat and muscle may be one of the reasons results regarding the risk of CVD in individuals with MHO are heterogeneous. However, there have been no studies to assess the associations between muscle mass and CVD according to obesity phenotype.
- Considering the limited availability of DXA in a clinical setting and the inability of BMI to estimate muscle mass, new obesity-related parameters that can distinguish between fat and muscle are needed. “A Body Shape Index” (ABSI) is a recently introduced parameter that reflects the body shape using waist circumference (WC), weight, and height [9]. Interestingly, ABSI was previously shown to have an inverse relationship with fat-free mass [10]; a modified ABSI also showed a positive association with the fat mass index as well as a negative association with the appendicular skeletal mass index (ASMI) [11]. Therefore, ABSI might supplement BMI by assessing muscle and fat mass.
- In the present study, we assessed the effects of sarcopenia as defined by whole body DXA and body shape on CVD risk according to obesity phenotypes in a representative population in the United States.
INTRODUCTION
- Study population
- We used data from the National Health and Nutrition Examination Survey (NHANES) collected between 1999 and 2012. This survey covers a representative sample from the United States and has been performed biannually by the National Center for Health Statistics since 1999 using questionnaire-based personal interviews, physical examinations, and laboratory tests. Among a population of 71,916, those 20 years of age or younger as well as those who lacked questionnaire-based data on CVD events; weight, height, and blood pressure (BP) measurements; and/or laboratory data including fasting glucose, triglycerides, and high-density lipoprotein were excluded. Ultimately, 25,270 adults were included in this study (Supplementary Fig. 1). Whole body DXA data were available between 1999 and 2005; therefore, 11,317 participants were included in the subgroup analysis for body composition.
- Measurements
- WC was measured by placing a flexible tape around the uppermost lateral border of the ilium. BMI was defined as the weight (kg) divided by the square of the height (m). BP was measured three times after a minimum of 5 minutes of rest while the participant was in a sitting position, and the mean value of the three measurements was used in our analysis. Fasting blood glucose and lipid levels were measured using the enzymatic method. More detailed sample collection and test methods are described in the NHANES Laboratory Procedures Manual [12].
- Definition of the obesity phenotypes and CVD
- In the present study, overweight/obesity was defined as a BMI above 25 kg/m2 based on the World Health Organization criteria [13]. Owing to lack of a standard definition for metabolically healthy status, the revised National Cholesterol Education Program–Adult Treatment Panel III criteria (NCEP–ATP III criteria) for metabolic syndrome, which are the most commonly used criteria in previous studies [14151617], were also used. Metabolic abnormality was defined as having two or more metabolic risk factors according to the revised NCEP–ATP III criteria, including impaired fasting glucose (i.e., a fasting glucose level >100 mg/dL or a diagnosis of DM), high BP (hypertensive BP >130 mm Hg and/or diastolic BP >85 mm Hg, or a diagnosis of hypertension), triglyceride level ≥150 mg/dL, and a high-density lipoprotein cholesterol level <40 mg/dL in men and <50 mg/dL in women. Owing to the collinearity between BMI and WC, the central obesity criterion was not used. Based on these aforementioned criteria, the participants were classified into the following groups: metabolically healthy normal weight (MHNW), MHO, metabolically unhealthy normal weight (MUNW) and metabolically unhealthy overweight/obese (MUO). We identified the existence of a CVD event if 1 or more of the following structured questions were answered in the affirmative:
-
1. Has a doctor ever told you that you have congestive heart failure?
2. Has a doctor ever told you that you have coronary heart disease?
3. Has a doctor ever told you that you had a heart attack (or myocardial infarction)?
4. Has a doctor ever told you that you have angina pectoris?
5. Has a doctor ever told you that you have cerebrovascular disease?
- Measurement of body composition and ABSI
- Among the 25,270 study participants, 11,317 underwent a whole body DXA using a QDR 4500A fan beam X-ray bone densitometer (Hologic Inc., Marlborough, MA, USA). The total and regional body compositions as measured using the DXA scans were analyzed using the Hologic Discovery software version 12.1 (Hologic Inc.). The appendicular skeletal mass was defined as the sum of the total lean mass excluding bone mineral contents from the limbs, and the ASMI was defined as the appendicular skeletal mass divided by the square of the height (m). Sarcopenia was defined as an ASMI <7 kg/m2 in men and <5.5kg/m2 in women based on the revised European consensus on the definition and diagnosis of sarcopenia [18]. ABSI was calculated using the following equation: ABSI=WC/(BMI2/3×height1/2) [9].
- Statistical analysis
- The NHANES is a complex sample survey representing the United States population; the sample analysis was conducted using weighted values. Continuous variables are shown as mean values and 95% confidence intervals (CIs), while categorical variables are shown as the prevalence and percentage according to each obesity phenotype. Each variable was compared using 1-way analysis of variance and Pearson's chi-square test. We implemented Pearson's correlation coefficient to verify the correlation of ABSI with ASMI, BMI, and WC. A receiver operating characteristic (ROC) curve was used to analyze the correlation between ABSI and sarcopenia according to obesity phenotypes. A multivariate logistic regression analysis was performed to evaluate the odds ratio (OR) for CVD events according to the obesity phenotype. To determine the effects of muscle mass, groups were divided according to the presence of sarcopenia, and each group's OR for a CVD event was examined. Moreover, ABSI was divided into three categories, and the ORs for CVD events were calculated. Furthermore, changes in the ORs for CVD events in each obesity phenotype as a function of changes in ABSI were analyzed using the restricted cubic spline plots with 3 knots. The analysis was performed using R version 3.1.0 (R Foundation for Statistical Computing, Vienna, Austria; www.r-project.org) and IBM SPSS Statistics version 24.0 (IBM Co., Armonk, NY, USA). A P<0.05 indicated statistical significance.
- Ethics statement
- The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Institutional Review Board of Hallym University Kangnam Sacred Heart Hospital (IRB No. HKS 2017-07-007). All the NHANES protocols were approved by the Research Ethics Review Board of the National Center for Health Statistics, US Centers for Disease Control and Prevention (NCHS IRB/ERB protocol numbers: 1999–2004, Protocol #98-12; 2005–2010, Protocol #2005-06; and 2011–2012, Protocol #2011-17). All participants volunteered and provided written informed consent prior to their enrollment. All participants' records were anonymized before being accessed by the authors, and all methods were performed in accordance with approved guidelines and regulations.
METHODS
- Baseline characteristics
- The baseline characteristics of the participants according to their obesity phenotypes are summarized in Table 1. Of the 25,270 participants assessed in this study, 5,176 had MHNW, 6,688 were MHO, 2,671 were MUNW, and 10,735 were MUO. Compared to metabolically healthy participants, those metallically unhealthy participants were more likely to be men and of older age; they also had higher BP, poorer lipid and glucose profiles, and a higher prevalence of CVD. Metabolically unhealthy participants had higher ABSIs than metabolically healthy counterparts. DXA data were available for 11,317 of the 25,270 subjects; participants who were obese had significantly higher ASMIs than those who were not. Moreover, participants with normal weight showed a higher prevalence of sarcopenia than obese participants did.
- Association between obesity phenotypes and the risk of CVD events
- A total of 2,637 CVD events were reported. In the multivariate logistic regression model with adjustment for age, sex, ethnicity and smoking status, participants with MHO were at a moderate risk of developing CVD when compared with MHNW participants (OR, 1.543; 95% CI, 1.158 to 2.056), whereas participants with metabolic abnormalities were at high risk regardless of obesity status (OR in MUNW, 2.026; 95% CI, 1.539 to 2.667) (OR in MUO, 2.725; 95% CI, 2.186 to 3.398) (Table 2).
- Correlation of ABSI with ASMI and other obesity-related parameters
- ABSI showed a moderate negative correlation with ASMI as well as a strong positive correlation with WC, regardless of obesity phenotype (Table 3). In contrast to ABSI, WC and BMI both showed a strong positive correlation with ASMI (overall correlation coefficient for WC, 0.631, P<0.001; overall correlation coefficient for BMI, 0.655, P<0.001). The area under the ROC curve (AUC) for ABSI showed significant accuracy for identifying sarcopenia (Table 4).
- Effect of sarcopenia and ABSI on the risk of CVDs according to obesity phenotypes
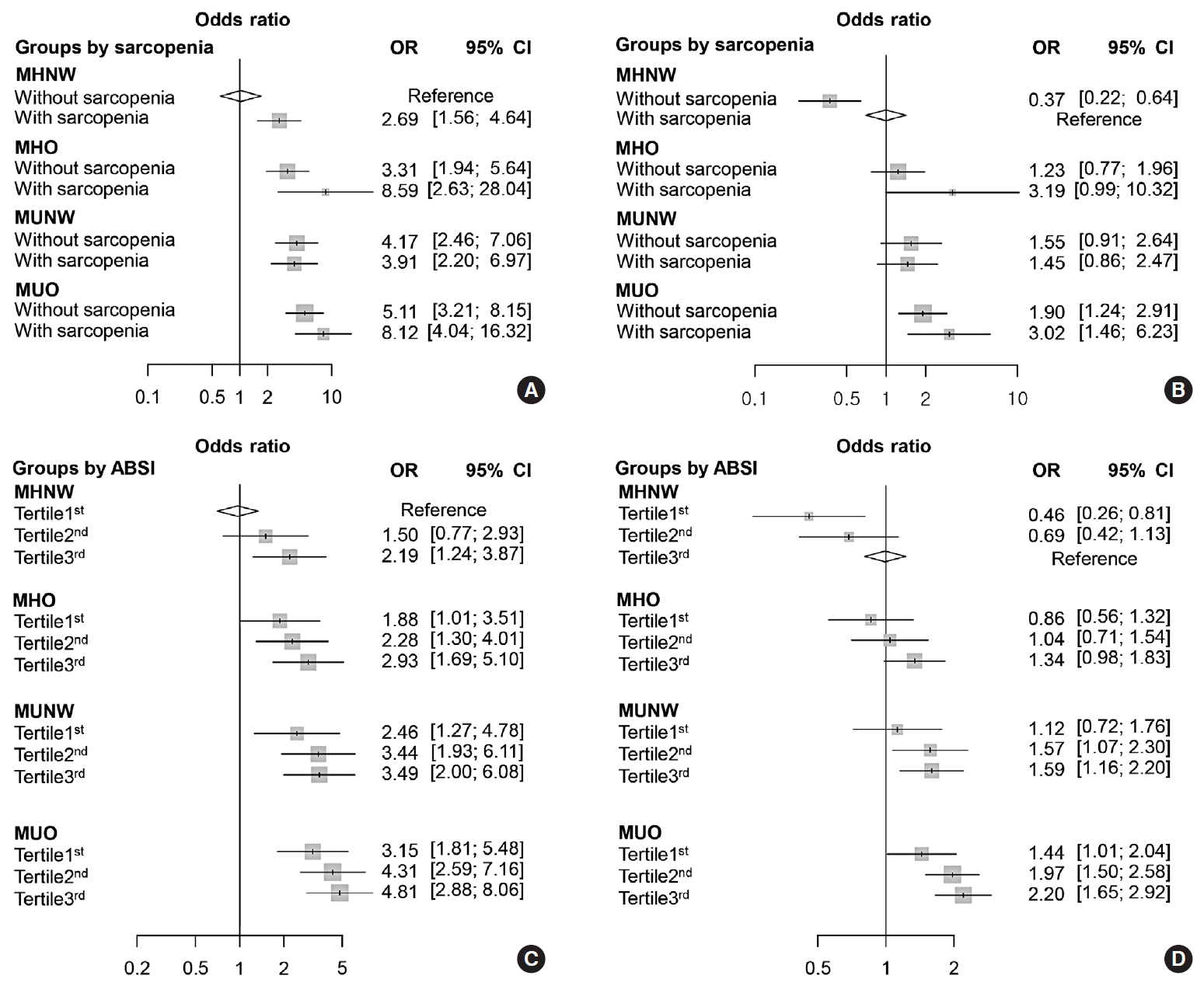
- The multivariate logistic regression analysis showed that the participants with sarcopenia had higher risk for CVD than those without sarcopenia in the group with MHNW (OR, 2.69; 95% CI, 1.56 to 4.64). The obese participants with sarcopenia showed a significantly higher ORs of CVD than those without sarcopenia in both the metabolically healthy and unhealthy groups (Fig. 1). Fig. 1A shows each OR according to obesity phenotype and sarcopenia status compared to MHNW participants without sarcopenia as a reference. The information in Fig. 1B is based on MHNW participants with sarcopenia as a reference. MHO participants had a significantly higher risk for CVD than did MHNW participants without sarcopenia (OR in MHO without sarcopenia, 3.31; 95% CI, 1.94 to 5.64) (OR in MHO with sarcopenia, 8.59; 95% CI, 2.63 to 28.04) (Fig. 1A). However, MHO participants did not have a significantly higher risk for CVD compared to the MHNW participants with sarcopenia (OR in MHO without sarcopenia, 1.23; 95% CI, 0.77 to 1.96) (OR in MHO with sarcopenia, 3.19; 95% CI, 0.99 to 10.23) (Fig. 1B).
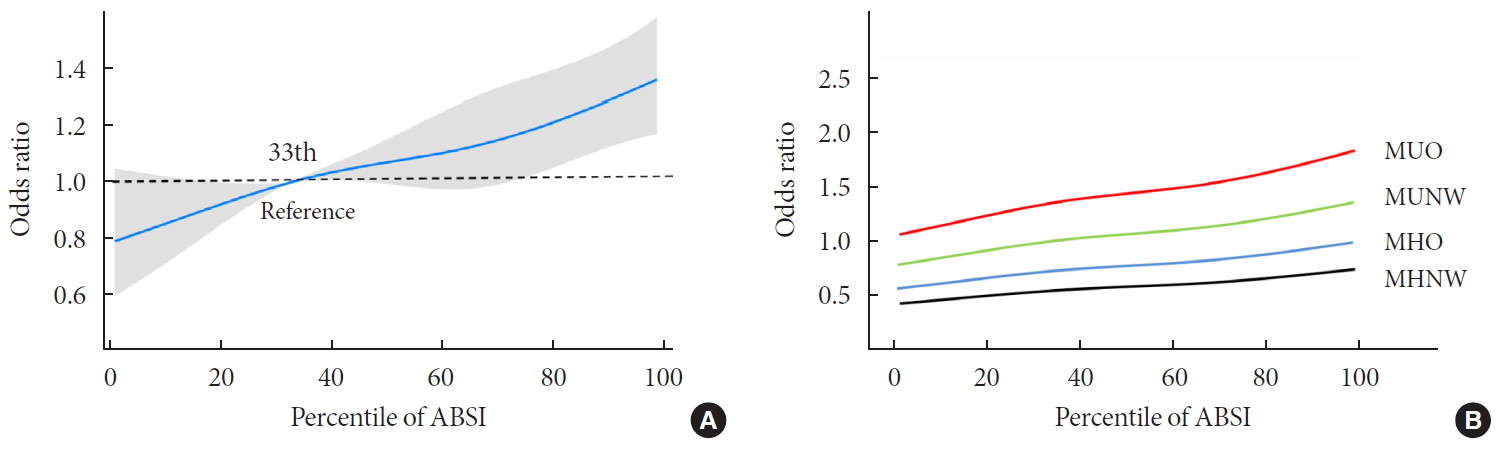
- The multivariate logistic regression analysis showed that MHO participants who were within the second and third tertiles of ABSI had significantly higher ORs for CVDs, while those who were within the first tertile of ABSI had only a slightly higher risk for CVD, compared to the MHNW participants who were within the first ABSI tertile (Fig. 1C). However, MHO participants did not have a significantly higher risk of CVD compared to the MHNW participants within the third ABSI tertile (OR in MHO participants within the first tertile, 0.86; 95% CI, 0.56 to 1.32) (OR in MHO participants within the second tertile, 1.04; 95% CI, 0.71 to 1.54) (OR in MHO participants within the third tertile, 1.34; 95% CI, 0.98 to 1.84) (Fig. 1D). On restricted cubic spline regression analysis, ORs for CVD increased by ABSI in each obesity phenotype (Fig. 2).
RESULTS
- The present study showed that sarcopenia was associated with a high risk of CVD in MHNW participants. We also observed that sarcopenia increased the risk of CVD even in obese participants regardless of metabolic abnormalities. Our large-scale data also revealed that ABSI is associated with sarcopenia and CVD risk according to obesity phenotypes.
- Notably, our results in MHNW participants with sarcopenia illustrated the need for taking into account muscle mass measurements when defining normal weight with BMI. Numerous epidemiological studies have found that sarcopenia is associated with insulin resistance [19], type 2 DM [20], increased risk of CVD-related mortality, and all-cause mortality [212223]. Our results were therefore consistent with those of previous studies. In addition, many studies showed that a combination of sarcopenia and obesity was more likely associated with metabolic disorders and morbidity [2425262728]. A recent meta-analysis found that sarcopenic obesity increased the risk of all-cause mortality by 21% [29]. Our results found that obese patients with sarcopenia had a higher risk of CVD than those without sarcopenia in both the metabolically healthy and unhealthy group.
- In the case of MHO phenotypes, several large-scale population-based studies have found an association between MHO and CVD risk [8], whereas several observational studies showed that MHO did not increase the risk of coronary atherosclerosis [30] or heart failure [31]. Our data suggested that if one study had an MHNW group with a high prevalence of sarcopenia as a control, their MHO phenotypes were not likely associated with an increased risk of CVD. Our data also revealed that if a study had an MHNW group with a low prevalence of sarcopenia as a control, their MHO phenotypes showed a remarkably higher risk for CVD. Therefore, the heterogeneity of information regarding prognoses in the various obesity studies could, at least in part, be due to overlooking the muscle mass measurement in their cohorts.
- Our result also revealed that ABSI was positively correlated with WC but inversely correlated with the ASMI and had moderate accuracy for identifying sarcopenia. This result is consistent with recent studies which found an association between ABSI and sarcopenic obesity [10113233]. Considering limited availability of DXA in a clinical setting and the inability of BMI for estimating muscle mass, ABSI (which is easily obtained from the weight, height, and WC) is a useful alternative for identifying individuals who are at risk of sarcopenic obesity.
- Several studies have examined the ABSI value as a predictor of CVD and mortality [9343536]. Moreover, a recent meta-analysis of 38 studies found that ABSI outperformed BMI and WC as a reliable predictor of all-cause mortality [37]. However, there is insufficient data on the association between ABSI and CVD according to obesity phenotypes. Only one study showed that a high level of modified ABSI increased the risk of CVD across obesity phenotypes using a Korean representative sample [38]. These data are consistent with our study using the United States representative sample. Considering the association between ABSI and sarcopenic obesity, the heterogeneity of CVD risk by ABSI in each obesity phenotype might reflect the influence of muscle loss on CVD.
- There were limitations to our study. First, the fact that it was cross-sectional indicates that additional prospective studies are necessary to clarify the relationship between each obesity phenotype and CVD events. Second, fatal CVD events may have been missed given that we did not assess mortality data. However, our study is the first study to investigate the association between sarcopenia and CVD events according to obesity phenotypes in the recent national representative sample. Our findings might provide one explanation for the heterogeneous results produced by previous studies with respect to the risk of developing CVD in obese individuals [83940].
- In conclusion, obese participants with sarcopenia had a higher risk of CVD than those without sarcopenia, regardless of metabolic abnormalities. We also showed that sarcopenia increased the risk of CVD even in healthy participants and these results persisted in ABSI. These results suggest that clinical approaches that consider muscle mass are required. However, since whole body DXA cannot be applicable to measure muscle mass in most clinical setting, ABSI is a useful alternative for identifying obese individuals who are at risk of sarcopenia and CVD. However, additional prospective studies must be conducted to determine the effect of muscle mass and ABSI on CVD according to the obesity phenotype.
DISCUSSION
SUPPLEMENTARY MATERIALS
Supplementary Fig. 1
-
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
AUTHOR CONTRIBUTIONS
Conception or design: S.M., J.G.K.
Acquisition, analysis, or interpretation of data: W.C., S.M., O.H.R.
Drafting the work or revising: H.W.C., W.C., S.M., M.K.K., J.G.K.
Final approval of the manuscript: H.W.C., W.C., S.M., O.H.R., M.K.K., J.G.K.
-
FUNDING
This work was supported by Research Resettlement Fund for the new faculty of Seoul National University and the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (grant No. 2017R1D1A1B03029575).
NOTES
-
Acknowledgements
- None
ACKNOWLEDGMENTS
- 1. Solomon CG, Manson JE. Obesity and mortality: a review of the epidemiologic data. Am J Clin Nutr 1997;66:4 Suppl. 1044S-1050S.ArticlePubMedPDF
- 2. Krauss RM, Winston M, Fletcher BJ, Grundy SM. Obesity: impact on cardiovascular disease. Circulation 1998;98:1472-1476.Article
- 3. Moon S, Oh CM, Choi MK, Park YK, Chun S, Choi M, et al. The influence of physical activity on risk of cardiovascular disease in people who are obese but metabolically healthy. PLoS One 2017;12:e0185127.ArticlePubMedPMC
- 4. Wallstrom P, Bjartell A, Gullberg B, Olsson H, Wirfalt E. A prospective Swedish study on body size, body composition, diabetes, and prostate cancer risk. Br J Cancer 2009;100:1799-1805.ArticlePubMedPMCPDF
- 5. Kushner RF. Clinical assessment and management of adult obesity. Circulation 2012;126:2870-2877.ArticlePubMed
- 6. Rey-Lopez JP, de Rezende LF, Pastor-Valero M, Tess BH. The prevalence of metabolically healthy obesity: a systematic review and critical evaluation of the definitions used. Obes Rev 2014;15:781-790.ArticlePubMed
- 7. Kim TN, Choi KM. The implications of sarcopenia and sarcopenic obesity on cardiometabolic disease. J Cell Biochem 2015;116:1171-1178.ArticlePubMed
- 8. Mirzababaei A, Djafarian K, Mozafari H, Shab-Bidar S. The long-term prognosis of heart diseases for different metabolic phenotypes: a systematic review and meta-analysis of prospective cohort studies. Endocrine 2019;63:439-462.ArticlePubMedPDF
- 9. Krakauer NY, Krakauer JC. A new body shape index predicts mortality hazard independently of body mass index. PLoS One 2012;7:e39504.ArticlePubMedPMC
- 10. Biolo G, Di Girolamo FG, Breglia A, Chiuc M, Baglio V, Vinci P, Toigo G, Lucchin L, Jurdana M, Praznikar ZJ, et al. Inverse relationship between “a body shape index” (ABSI) and fat-free mass in women and men: insights into mechanisms of sarcopenic obesity. Clin Nutr 2015;34:323-327.ArticlePubMed
- 11. Chung W, Park JH, Chung HS, Yu JM, Kim DS, Moon S. Utility of the Z-score of log-transformed A Body Shape Index (LBSIZ) in the assessment for sarcopenic obesity and cardiovascular disease risk in the United States. Sci Rep 2019;9:9292.ArticlePubMedPMCPDF
- 12. Centers for Disease Control and Prevention. The National Health and Nutrition Examination Survey (NHANES) MEC laboratory procedures manual cited 2020 Mar 10. Available from: https://wwwn.cdc.gov/nchs/data/nhanes/2015-2016/manuals/2016_mec_laboratory_procedures_manual.pdf.
- 13. World Health Organization. Fact sheet on obesity and overweight cited 2020 Mar 10. Available from: http://www.who.int/en/news-room/fact-sheets/detail/obesity-and-overweight.
- 14. Grundy SM, Cleeman JI, Daniels SR, Donato KA, Eckel RH, Franklin BA, et al. American Heart Association. National Heart, Lung, and Blood Institute. Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation 2005;112:2735-2752.ArticlePubMed
- 15. Jung CH, Lee MJ, Kang YM, Jang JE, Leem J, Hwang JY, et al. The risk of incident type 2 diabetes in a Korean metabolically healthy obese population: the role of systemic inflammation. J Clin Endocrinol Metab 2015;100:934-941.ArticlePubMedPDF
- 16. Heianza Y, Arase Y, Tsuji H, Fujihara K, Saito K, Hsieh SD, et al. Metabolically healthy obesity, presence or absence of fatty liver, and risk of type 2 diabetes in Japanese individuals: Toranomon Hospital Health Management Center Study 20 (TOPICS 20). J Clin Endocrinol Metab 2014;99:2952-2960.ArticlePubMedPDF
- 17. Hinnouho GM, Czernichow S, Dugravot A, Nabi H, Brunner EJ, Kivimaki M, et al. Metabolically healthy obesity and the risk of cardiovascular disease and type 2 diabetes: the Whitehall II cohort study. Eur Heart J 2015;36:551-559.ArticlePubMedPDF
- 18. Cruz-Jentoft AJ, Bahat G, Bauer J, Boirie Y, Bruyere O, Cederholm T, et al. Writing Group for the European Working Group on Sarcopenia in Older People 2 (EWGSOP2), and the Extended Group for EWGSOP2. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing 2019;48:16-31.ArticlePubMedPDF
- 19. Srikanthan P, Hevener AL, Karlamangla AS. Sarcopenia exacerbates obesity-associated insulin resistance and dysglycemia: findings from the National Health and Nutrition Examination Survey III. PLoS One 2010;5:e10805.ArticlePubMedPMC
- 20. Kim TN, Park MS, Yang SJ, Yoo HJ, Kang HJ, Song W, et al. Prevalence and determinant factors of sarcopenia in patients with type 2 diabetes: the Korean Sarcopenic Obesity Study (KSOS). Diabetes Care 2010;33:1497-1499.PubMedPMC
- 21. Han SS, Kim KW, Kim KI, Na KY, Chae DW, Kim S, et al. Lean mass index: a better predictor of mortality than body mass index in elderly Asians. J Am Geriatr Soc 2010;58:312-317.ArticlePubMed
- 22. Wannamethee SG, Shaper AG, Lennon L, Whincup PH. Decreased muscle mass and increased central adiposity are independently related to mortality in older men. Am J Clin Nutr 2007;86:1339-1346.ArticlePubMedPDF
- 23. Atkins JL, Whincup PH, Morris RW, Lennon LT, Papacosta O, Wannamethee SG. Sarcopenic obesity and risk of cardiovascular disease and mortality: a population-based cohort study of older men. J Am Geriatr Soc 2014;62:253-260.ArticlePubMedPMCPDF
- 24. Zamboni M, Mazzali G, Fantin F, Rossi A, Di Francesco V. Sarcopenic obesity: a new category of obesity in the elderly. Nutr Metab Cardiovasc Dis 2008;18:388-395.ArticlePubMed
- 25. Choi KM. Sarcopenia and sarcopenic obesity. Endocrinol Metab (Seoul) 2013;28:86-89.ArticlePubMedPMC
- 26. Lim S, Kim JH, Yoon JW, Kang SM, Choi SH, Park YJ, et al. Sarcopenic obesity: prevalence and association with metabolic syndrome in the Korean Longitudinal Study on Health and Aging (KLoSHA). Diabetes Care 2010;33:1652-1654.ArticlePubMedPMCPDF
- 27. Lu CW, Yang KC, Chang HH, Lee LT, Chen CY, Huang KC. Sarcopenic obesity is closely associated with metabolic syndrome. Obes Res Clin Pract 2013;7:e301-e307.ArticlePubMed
- 28. Choi KM. Sarcopenia and sarcopenic obesity. Korean J Intern Med 2016;31:1054-1060.ArticlePubMedPMCPDF
- 29. Zhang X, Xie X, Dou Q, Liu C, Zhang W, Yang Y, et al. Association of sarcopenic obesity with the risk of all-cause mortality among adults over a broad range of different settings: a updated meta-analysis. BMC Geriatr 2019;19:183.ArticlePubMedPMCPDF
- 30. Morkedal B, Vatten LJ, Romundstad PR, Laugsand LE, Janszky I. Risk of myocardial infarction and heart failure among metabolically healthy but obese individuals: HUNT (Nord-Trondelag Health Study), Norway. J Am Coll Cardiol 2014;63:1071-1078.PubMed
- 31. Voulgari C, Tentolouris N, Dilaveris P, Tousoulis D, Katsilambros N, Stefanadis C. Increased heart failure risk in normal-weight people with metabolic syndrome compared with metabolically healthy obese individuals. J Am Coll Cardiol 2011;58:1343-1350.ArticlePubMed
- 32. Gomez-Peralta F, Abreu C, Cruz-Bravo M, Alcarria E, Gutierrez-Buey G, Krakauer NY, et al. Relationship between “a body shape index (ABSI)” and body composition in obese patients with type 2 diabetes. Diabetol Metab Syndr 2018;10:21.ArticlePubMedPMCPDF
- 33. Dhana K, Koolhaas CM, Schoufour JD, Rivadeneira F, Hofman A, Kavousi M, et al. Association of anthropometric measures with fat and fat-free mass in the elderly: the Rotterdam study. Maturitas 2016;88:96-100.ArticlePubMed
- 34. Lee DY, Lee MY, Sung KC. Prediction of mortality with a body shape index in young Asians: comparison with body mass index and waist circumference. Obesity (Silver Spring) 2018;26:1096-1103.ArticlePubMedPDF
- 35. Dhana K, Kavousi M, Ikram MA, Tiemeier HW, Hofman A, Franco OH. Body shape index in comparison with other anthropometric measures in prediction of total and cause-specific mortality. J Epidemiol Community Health 2016;70:90-96.ArticlePubMed
- 36. Bozorgmanesh M, Sardarinia M, Hajsheikholeslami F, Azizi F, Hadaegh F. CVD-predictive performances of “a body shape index” versus simple anthropometric measures: Tehran lipid and glucose study. Eur J Nutr 2016;55:147-157.ArticlePubMedPDF
- 37. Ji M, Zhang S, An R. Effectiveness of A Body Shape Index (ABSI) in predicting chronic diseases and mortality: a systematic review and meta-analysis. Obes Rev 2018;19:737-759.ArticlePubMedPDF
- 38. Chung W, Park JH, Ryu OH, Yu JM, Yoo HJ, Moon S. Association of Z-score of the log-transformed a body shape index with cardiovascular disease in people who are obese but metabolically healthy: the Korea National Health and Nutrition Examination Survey 2007–2010. J Obes Metab Syndr 2018;27:158-165.ArticlePubMedPMCPDF
- 39. Arnlov J, Ingelsson E, Sundstrom J, Lind L. Impact of body mass index and the metabolic syndrome on the risk of cardiovascular disease and death in middle-aged men. Circulation 2010;121:230-236.ArticlePubMed
- 40. Hinnouho GM, Czernichow S, Dugravot A, Batty GD, Kivimaki M, Singh-Manoux A. Metabolically healthy obesity and risk of mortality: does the definition of metabolic health matter? Diabetes Care 2013;36:2294-2300.PubMedPMC
REFERENCES
Weighted odds ratio (OR) (95% confidence interval [CI]) for cardiovascular events in terms of (A, B) obesity phenotype and sarcopenia, or (C, D) tertiles of A Body Shape Index (ABSI). (A) Compared to metabolically healthy normal weight (MHNW) without sarcopenia, (B) compared to MHNW with sarcopenia, (C) compared to MHNW with the first ABSI tertile, and (D) compared to MHNW with the third ABSI tertile. Values were adjusted for age, sex, ethnicity, and smoking status. MHO, metabolically healthy overweight/obese; MUNW, metabolically healthy normal weight; MUO, metabolically unhealthy overweight/obese.
Relationship between continuous A Body Shape Index (ABSI) and the odds ratios for cardiovascular events according to obesity phenotypes. (A) Total population, and (B) obesity phenotype subgroups. Values were adjusted for age, sex, ethnicity, and smoking status. MUO, metabolically unhealthy overweight/obese; MUNW, metabolically unhealthy normal weight; MHO, metabolically healthy overweight/obese; MHNW, metabolically healthy normal weight.

| Variable |
Metabolically healthy |
Metabolically unhealthy |
P value | |||
|---|---|---|---|---|---|---|
| Normal weight (MHNW) (n=5,176) | Overweight/obesity (MHO) (n=6,688) | Normal weight (MUNW) (n=2,671) | Overweight/obesity (MUO) (n=10,735) | |||
| Age, yr | 38.2 (37.6–38.8) | 40.9 (40.4–41.5) | 54.7 (53.8–55.5) | 51.7 (51.3–52.2) | <0.001 | |
| Men, % | 39.6 (38.0–41.2) | 47.6 (46.3–49.0) | 48.1 (45.8–50.3) | 54.1 (53.0–55.2) | <0.001 | |
| Ethnicity/Race, % | <0.001 | |||||
| Mexican American | 6.2 (5.4–7.2) | 9.2 (7.7–10.9) | 4.6 (3.8–5.5) | 8.2 (6.7–9.8) | ||
| Other Hispanic | 4.3 (3.3–5.4) | 6.1 (4.8–7.7) | 4.4 (3.2–6.1) | 5.4 (4.3–6.9) | ||
| Non-Hispanic White | 73.9 (71.7–75.9) | 67.6 (64.7–70.3) | 73.4 (70.3–76.3) | 71.9 (69.1–74.6) | ||
| Non-Hispanic Black | 8.4 (7.4–9.6) | 13.2 (11.6–15) | 7.5 (6.4–8.9) | 10.2 (8.9–11.7) | ||
| Other race | 7.2 (6.2–8.3) | 4 (3.3–4.8) | 10 (8.3–12.1) | 4.3 (3.6–5.1) | ||
| CVD eventsa, % | 2.3 (1.8–2.9) | 4 (3.5–4.6) | 12.3 (10.9–13.9) | 12.5 (11.7–13.4) | ||
| Smoking, % | 45.4 (43.3–47.6) | 43.8 (42.1–45.7) | 55.5 (53–58.1) | 51.3 (49.9–52.7) | ||
| BMI, kg/m2 | 22 (22–22.1) | 30.2 (30–30.3) | 22.6 (22.5–22.7) | 32 (31.8–32.1) | <0.001 | |
| Waist circumference, cm | 80.7 (80.4–81) | 100.3 (99.9–100.8) | 85.5 (85.1–85.9) | 107.3 (106.8–107.7) | <0.001 | |
| ABSI | 0.0791 (0.0789–0.0793) | 0.0798 (0.0796–0.0800) | 0.0826 (0.0823–0.0828) | 0.0823 (0.0821–0.0824) | <0.001 | |
| ASMIa, kg/m2 | 6.55 (6.49 – 6.62) | 8.16 (8.10 – 8.22) | 6.45 (6.37 – 6.54) | 8.30 (8.24 – 8.36) | <0.001 | |
| Sarcopenia, % | 27.0 (24.4–29.8) | 1.4 (1.0–1.9) | 38.8 (35.9–41.8) | 2.1 (1.7–2.7) | <0.001 | |
| Systolic BP, mm Hg | 112 (111.5–112.5) | 115.6 (115.2–116) | 131 (129.8–132.2) | 129.1 (128.5–129.6) | <0.001 | |
| Diastolic BP, mm Hg | 67.9 (67.5–68.4) | 69.7 (69.3–70.1) | 72.5 (71.8–73.2) | 73.9 (73.5–74.4) | <0.001 | |
| FBG level, mg/dL | 90.8 (90.4–91.2) | 93.5 (93–94.1) | 105.9 (104.4–107.5) | 114.1 (112.8–115.4) | <0.001 | |
| HbA1c, % | 5.2 (5.2–5.2) | 5.3 (5.3–5.3) | 5.6 (5.6–5.7) | 5.9 (5.8–5.9) | <0.001 | |
| Total cholesterol, mg/dL | 185.7 (184.3–187.2) | 193.4 (192.2–194.6) | 209.2 (206.9–211.4) | 208.5 (207.1–209.8) | <0.001 | |
| HDL-C, mg/dL | 61.4 (60.8–62) | 54.9 (54.4–55.3) | 56.4 (55.3–57.5) | 46.5 (46.1–46.9) | <0.001 | |
| TG, mg/dL | 89.5 (86.7–92.3) | 107.9 (105.4–110.5) | 141.8 (131.7–151.8) | 183.3 (177.6–189.1) | <0.001 | |
| Metabolic state, % | ||||||
| High BP | 5.2 (4.5–6) | 6.8 (6–7.7) | 59.8 (57.2–62.4) | 51.4 (49.9–52.8) | <0.001 | |
| Hyperglycemia | 4.1 (3.5–4.7) | 5.9 (5.2–6.6) | 44.4 (41.7–47.1) | 55.6 (54–57.2) | <0.001 | |
| Low HDL-C level | 9.3 (8.2–10.4) | 13.1 (12–14.2) | 34 (31.4–36.8) | 52.5 (51.2–53.9) | <0.001 | |
| High TG level | 37.5 (35.9–39.2) | 48.3 (46.5–50) | 91.9 (90.4–93.2) | 91.8 (91–92.5) | <0.001 | |
Values are presented as mean (95% confidence interval).
MHNW, metabolically healthy normal weight; MHO, metabolically healthy overweight/obese; MUNW, metabolically unhealthy normal weight; MUO, metabolically unhealthy overweight/obese; CVD, cardiovascular disease; BMI, body mass index; ABSI, A Body Shape Index; ASMI, appendicular skeletal mass index; BP, blood pressure; FBG, fasting blood glucose; HbA1c, glycosylated hemoglobin; HDL-C, high-density lipoprotein cholesterol; TG, triglyceride.
a Participants who had either angina pectoris, coronary heart disease, myocardial infarction, congestive heart failure, or cerebrovascular disease.
| Variable | OR (95% CI) | P value |
|---|---|---|
| MHNW | 1 (reference) | |
| MHO | 1.543 (1.158–2.056) | 0.003 |
| MUNW | 2.026 (1.539–2.667) | <0.001 |
| MUO | 2.725 (2.186–3.398) | <0.001 |
| Group |
Correlation coefficients |
||
|---|---|---|---|
| ASMI | BMI | Waist circumference | |
| MHNW | |||
| Men | –0.586b | 0.039 | 0.695b |
| Women | –0.332b | –0.039a | 0.660b |
| MHO | |||
| Men | –0.400b | 0.082b | 0.552b |
| Women | –0.285b | –0.132b | 0.403b |
| MUNW | |||
| Men | –0.596b | 0.036 | 0.711b |
| Women | –0.283b | –0.043 | 0.694b |
| MUO | |||
| Men | –0.433b | –0.024 | 0.399b |
| Women | –0.351b | –0.249b | 0.251b |
Figure & Data
References
Citations
- Association of low muscle mass and obesity with increased all‐cause and cardiovascular disease mortality in US adults
Donghyun Kim, Junghoon Lee, Raekil Park, Chang‐Myung Oh, Shinje Moon
Journal of Cachexia, Sarcopenia and Muscle.2024; 15(1): 240. CrossRef - Metabolic-associated fatty liver disease and sarcopenia: A double whammy
Aditya Viswanath, Sherouk Fouda, Cornelius James Fernandez, Joseph M Pappachan
World Journal of Hepatology.2024; 16(2): 152. CrossRef - Association of Myosteatosis with Nonalcoholic Fatty Liver Disease, Severity, and Liver Fibrosis Using Visual Muscular Quality Map in Computed Tomography
Hwi Seung Kim, Jiwoo Lee, Eun Hee Kim, Min Jung Lee, In Young Bae, Woo Je Lee, Joong-Yeol Park, Hong-Kyu Kim, Chang Hee Jung
Diabetes & Metabolism Journal.2023; 47(1): 104. CrossRef - Additive impact of diabetes and sarcopenia on all-cause and cardiovascular mortality: A longitudinal nationwide population-based study
Eyun Song, Soon Young Hwang, Min Jeong Park, Ahreum Jang, Kyeong Jin Kim, Ji Hee Yu, Nam Hoon Kim, Hye Jin Yoo, Ji A. Seo, Sin Gon Kim, Nan Hee Kim, Sei Hyun Baik, Kyung Mook Choi
Metabolism.2023; 148: 155678. CrossRef - Association between a body shape index and abdominal aortic calcification in general population: A cross-sectional study
Wei Li, Zhenwei Wang, Min Li, Jing Xie, Jing Gong, Naifeng Liu
Frontiers in Cardiovascular Medicine.2023;[Epub] CrossRef - Metabolic Impact of Frailty Changes Diabetes Trajectory
Alan J. Sinclair, Ahmed H. Abdelhafiz
Metabolites.2023; 13(2): 295. CrossRef - Association between sarcopenic obesity and poor muscle quality based on muscle quality map and abdominal computed tomography
Yun Kyung Cho, Han Na Jung, Eun Hee Kim, Min Jung Lee, Joong‐Yeol Park, Woo Je Lee, Hong‐Kyu Kim, Chang Hee Jung
Obesity.2023; 31(6): 1547. CrossRef - Metabolic Characteristics of Frail Older People with Diabetes Mellitus—A Systematic Search for Phenotypes
Ahmed H. Abdelhafiz, Grace L. Keegan, Alan J. Sinclair
Metabolites.2023; 13(6): 705. CrossRef - Risk of Cardiovascular Diseases Among Different Metabolic Obesity Phenotypes: A Prospective Observational Study
Xiaowei Liu, Chan Yang, Yuanyuan Dang, Zhenqi Chang, Juan Li, Yi Zhao, Yuhong Zhang
Metabolic Syndrome and Related Disorders.2023; 21(6): 306. CrossRef - Effect of Hypoxia Conditioning on Body Composition in Middle-Aged and Older Adults: A Systematic Review and Meta-Analysis
Zhijian He, Lijun Qiang, Yusheng Liu, Wenfeng Gao, Tao Feng, Yang Li, Bing Yan, Olivier Girard
Sports Medicine - Open.2023;[Epub] CrossRef - Association Between a Body Shape Index and Subclinical Carotid Atherosclerosis in Population Free of Cardiovascular and Cerebrovascular Diseases
Xiaotian Ma, Lihong Chen, Wenchao Hu, Lanjie He
Journal of Atherosclerosis and Thrombosis.2022; 29(8): 1140. CrossRef - Impact of Sarcopenia on the Severity of the Liver Damage in Patients With Non-alcoholic Fatty Liver Disease
Vittoria Zambon Azevedo, Cristina Alina Silaghi, Thomas Maurel, Horatiu Silaghi, Vlad Ratziu, Raluca Pais
Frontiers in Nutrition.2022;[Epub] CrossRef - Identification of sarcopenic obesity in adults undergoing orthopaedic surgery: Relationship between “a body shape index” (ABSI) and fat-free mass. A cross -sectional study
Ana Tomažič, Boštjan Žvanut, Lilijana Vouk Grbac, Mihaela Jurdana, Fatih Özden
PLOS ONE.2022; 17(6): e0269956. CrossRef - Associations of Dynapenic Obesity and Sarcopenic Obesity with the Risk of Complications in COVID-19
Laura Pérez-Campos Mayoral, Carlos Alberto Matias-Cervantes, Eduardo Pérez-Campos, Carlos Romero Díaz, Luis Ángel Laguna Barrios, María del Socorro Pina Canseco, Margarito Martínez Cruz, Eduardo Pérez-Campos Mayoral, Carlos Josué Solórzano Mata, Francisco
International Journal of Molecular Sciences.2022; 23(15): 8277. CrossRef - Sex Differences in Adiposity and Cardiovascular Diseases
Haoyun Li, Daniels Konja, Luyao Wang, Yu Wang
International Journal of Molecular Sciences.2022; 23(16): 9338. CrossRef - The Applicability of the ESPEN and EASO-Defined Diagnostic Criteria for Sarcopenic Obesity in Japanese Patients after Stroke: Prevalence and Association with Outcomes
Yoshihiro Yoshimura, Hidetaka Wakabayashi, Fumihiko Nagano, Ayaka Matsumoto, Sayuri Shimazu, Ai Shiraishi, Yoshifumi Kido, Takahiro Bise
Nutrients.2022; 14(19): 4205. CrossRef - The value of combining the simple anthropometric obesity parameters, Body Mass Index (BMI) and a Body Shape Index (ABSI), to assess the risk of non-alcoholic fatty liver disease
Maobin Kuang, Guotai Sheng, Chong Hu, Song Lu, Nan Peng, Yang Zou
Lipids in Health and Disease.2022;[Epub] CrossRef - Sarcopenia and cardiovascular disease in patients with and without kidney disease: what do we know?
Ozkan Gungor, Mustafa Sevinc, Sena Ulu, Ismail Kocyigit
International Urology and Nephrology.2022; 55(5): 1161. CrossRef - Skeletal Muscle Should Not Be Overlooked
Ji A Seo
Diabetes & Metabolism Journal.2021; 45(2): 173. CrossRef - The Role of Sarcopenic Obesity in Cancer and Cardiovascular Disease: A Synthesis of the Evidence on Pathophysiological Aspects and Clinical Implications
Erika Aparecida Silveira, Rômulo Roosevelt da Silva Filho, Maria Claudia Bernardes Spexoto, Fahimeh Haghighatdoost, Nizal Sarrafzadegan, Cesar de Oliveira
International Journal of Molecular Sciences.2021; 22(9): 4339. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite