- Current
- Browse
- Collections
-
For contributors
- For Authors
- Instructions to authors
- Article processing charge
- e-submission
- For Reviewers
- Instructions for reviewers
- How to become a reviewer
- Best reviewers
- For Readers
- Readership
- Subscription
- Permission guidelines
- About
- Editorial policy
Articles
- Page Path
- HOME > Diabetes Metab J > Volume 37(3); 2013 > Article
-
Original ArticleOthers Safety and Efficacy of Modern Insulin Analogues
- Hye Jin Yoo1, Keun Yong Park2, Kang Seo Park3, Kyu Jeung Ahn4, Kyung Wan Min5, Jeong Hyun Park6, Sang Ah Chang7, Bong Soo Cha8, Dong-Jun Kim6, Yong Seong Kim9, Tae Keun Oh10, Suk Chon4, Il Seong Nam-Goong11, Mi Jin Kim12, Hye-Soon Kim13, Young Sik Choi14, You Hern Ahn15, Sora Lee16, Sei Hyun Baik1
-
Diabetes & Metabolism Journal 2013;37(3):181-189.
DOI: https://doi.org/10.4093/dmj.2013.37.3.181
Published online: June 14, 2013
- 4,093 Views
- 32 Download
- 9 Crossref
1Department of Internal Medicine, Korea University College of Medicine, Seoul, Korea.
2Department of Internal Medicine, Konyang University College of Medicine, Daejeon, Korea.
3Department of Internal Medicine, Eulji University School of Medicine, Daejeon, Korea.
4Department of Internal Medicine, Kyung Hee University School of Medicine, Seoul, Korea.
5Department of Internal Medicine, Eulji University School of Medicine, Seoul, Korea.
6Department of Internal Medicine, Inje University College of Medicine, Busan, Korea.
7Department of Internal Medicine, The Catholic University of Korea College of Medicine, Seoul, Korea.
8Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea.
9Department of Internal Medicine, Inha University School of Medicine, Incheon, Korea.
10Department of Internal Medicine, Chungbuk National University College of Medicine, Cheongju, Korea.
11Department of Internal Medicine, University of Ulsan College of Medicine, Ulsan, Korea.
12Department of Internal Medicine, Hongik Hospital, Seoul, Korea.
13Department of Internal Medicine, Keimyung University School of Medicine, Daegu, Korea.
14Department of Internal Medicine, Kosin University College of Medicine, Busan, Korea.
15Department of Internal Medicine, Hanyang University College of Medicine, Seoul, Korea.
16Novo Nordisk Pharma Korea, Seoul, Korea.
- Corresponding author: Sei Hyun Baik. Division of Endocrinology and Metabolism, Department of Internal Medicine, Korea University Guro Hospital, Korea University College of Medicine, 148 Gurodong-ro, Guro-gu, Seoul 152-703, Korea. 103hyun@korea.ac.kr
Copyright © 2013 Korean Diabetes Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Background
- A1chieve® was a noninterventional study evaluating the clinical safety and efficacy of biphasic insulin aspart 30, insulin detemir, and insulin aspart.
-
Methods
- Korean type 2 diabetes patients who have not been treated with the study insulin or have started it within 4 weeks before enrollment were eligible for the study. The patient selection and the choice of regimen were at the discretion of the physician. The safety and efficacy information was collected from the subjects at baseline, week 12, and week 24. The number of serious adverse drug reactions (SADRs) was the primary endpoint. The changes of clinical diabetic markers at week 12 and/or at week 24 compared to baseline were the secondary endpoints.
-
Results
- Out of 4,058 exposed patients, 3,003 completed the study. During the study period, three SADRs were reported in three patients (0.1%). No major hypoglycemic episodes were observed and the rate of minor hypoglycemic episodes marginally decreased during 24 weeks (from 2.77 to 2.42 events per patient-year). The overall quality of life score improved (from 66.7±15.9 to 72.5±13.5) while the mean body weight was slightly increased (0.6±3.0 kg). The 24-week reductions in glycated hemoglobin, fasting plasma glucose and postprandial plasma glucose were 1.6%±2.2%, 2.5±4.7 mmol/L, and 4.0±6.4 mmol/L, respectively.
-
Conclusion
- The studied regimens showed improvements in glycemic control with low incidence of SADRs, including no incidence of major hypoglycemic episodes in Korean patients with type 2 diabetes.
- Improved glycemic control is essential in reducing the complications of type 2 diabetes [1,2]. Reduction of glycated hemoglobin (HbA1c) by 1.0% is associated with 43% reduction in the risk of amputation, a 37% reduction in microvascular disease, and a 16% reduction in heart failure [2]. However, in routine clinical practice, the majority of people with diabetes still experience considerable periods where their HbA1c levels exceed the target range, thus rendering them vulnerable to diabetes-related complications later in life [3,4]. As the disease progresses, a large number of individuals with type 2 diabetes eventually require insulin therapy in order to maintain glycemic control, and many studies have suggested earlier initiation of insulin for strict glucose control [5]. U.K. Prospective Diabetes Study confirmed that early addition of insulin to oral therapy can safely control HbA1c close to the target level [6].
- Despite the demonstrated efficacy of insulin therapy in achieving glycemic control in type 2 diabetes, there are several barriers to initiation of insulin therapy, which are set by both physicians and patients. This reluctance to insulin treatment arises from fear of injection, nonacceptance of treatment failure with oral hypoglycemic agents, and special concerns about hypoglycemia and weight gain after insulin therapy [7,8]. Modern insulin analogue were designed to achieve better glycemic control and less side effects with their favorable action profiles [7,9]. Until now, various randomized controlled clinical trials (RCTs) and some observational studies have demonstrated that the change to the insulin analogues from oral hypoglycemic agents or conventional insulin preparations has resulted in the favorable treatment outcome [10-14]. However, RCTs usually focus on a much more select patient group with intensive clinical supervision, excluding those who are predicted to have unfavorable prognosis such as elderly and patient with serious comorbidities. Furthermore, RCTs are rarely performed in less well-resourced countries. As a result, these RCTs may not represent the real clinical practice; an observational study might be an effective way of assessing the effectiveness and safety of drugs under routine clinical conditions. Although there have been some observational studies of insulin analogues, a large-scale observation study involving basal, bolus and premix insulin analogues simultaneously, has not been performed as of yet.
- A1chieve® study was a 24-week, international, prospective, multicentre, open-labeled, noninterventional clinical research evaluating the benefits of biphasic insulin aspart 30, insulin detemir, and insulin aspart (alone or in combination) in a large and diverse population with type 2 diabetes (more than 66,000 people from 28 different countries across four continents). The aim of A1chieve® study was to reflect the postmarketing authorization experience regarding safety and efficacy with insulin analogues in routine clinical practice. This article presents a subgroup analysis of South Korean patients with type 2 diabetes who have been treated with study insulin analogues in A1chieve® study.
INTRODUCTION
- The study was performed in accordance with the Declaration of Helsinki and the guidelines for Good Pharmacoepidemiology Practices. The protocol was reviewed and approved by independent institutional review boards in the study sites, and all the participants gave written informed consent before any trial-related activity. A1chieve® was registered at ClinicalTrial.gov (trial number: NCT00869908). A total of 104 sites from South Korea were involved in this study.
- Study population
- Korean type 2 diabetes patients who were planned to use or who had started biphasic insulin aspart 30, insulin detemir, or insulin aspart within the last 4 weeks before inclusion into this study with no history of prior treatment with these insulins (alone or in combination) were eligible for this study. Intensive exclusion criteria are not applied to noninterventional study. Patients with hypersensitivity to the study products or women who were pregnant, breast feeding or had the intention of becoming pregnant within the next 6 months were excluded from the study. Patients were allowed to withdraw from the study at any time. The termination of study insulin was at the discretion of the physicians based upon their clinical evaluation.
- Study products
- Biphasic insulin aspart 30, insulin detemir, and insulin aspart (DK-2880; Novo Nordisk A/S, Bagsværd, Denmark) available as prefilled 3 mL FlexPen® (100 U/mL; Novo Nordisk A/S) or 3 mL Penfill® (Novo Nordisk A/S) were used as commercially available products. NovoFine® (Novo Nordisk A/S) disposable needles designed for use with the above devices were used. The study insulins were used in accordance with the label approved by the regulatory authorities or the respective product information.
- Study design
- The total duration of the study was 24 weeks. The data were collected at baseline, interim visit (approximately 12 weeks after the baseline visit), and final visit (approximately 24 weeks after the baseline visit). Because of the noninterventional "real-world" setting of the study, there was no study-related procedures defined for this study, and the selection of patients and the choice of insulin regimen were fully at the discretion of the physician based on clinical judgments. During the study period, the number of serious adverse drug reactions (SADRs), including major hypoglycemic events, was evaluated as primary safety endpoint. The secondary safety endpoints were as follows: 1) the change in number of 4-week hypoglycemic events and nocturnal hypoglycemic events before interim and final visit compared to the baseline visit or the start of study insulin if the study insulin was started before enrollment; 2) the number of adverse drug reaction (ADRs) from baseline to final visit; 3) the change in body weight at interim and final visit compared to baseline; 4) others (any adverse events, lipid profile, and creatinine level at week 24 compared to baseline). Hypoglycemic event was defined as an event with one of following characteristics: 1) symptoms of hypoglycemia that resolve with oral carbohydrate intake, glucagon or as intravenous glucose or 2) any symptomatic or asymptomatic plasma glucose <3.1 mmol/L or 56 mg/dL. Nocturnal hypoglycemic event was defined as individualized symptomatic events consistent with hypoglycemia that occur while the subject is asleep. Major hypoglycemic events was defined as an event with severe central nervous system symptoms consistent with hypoglycaemia in which the subject is unable to treat himself/herself and has one of the following characteristics: 1) plasma glucose <3.1 mmol/L or 56 mg/dl or 2) reversal of symptoms after either food intake or glucagon or intravenous glucose administration. Efficacy endpoints were all considered as the secondary study endpoints. The changes in clinical diabetic markers such as fasting plasma glucose (FPG), postprandial glucose (PPG, after breakfast), HbA1c, and lipid profile were evaluated at baseline, interim and final visit, and the quality of life (QoL) evaluated using EQ-5D-3L was measured only at final visit, which was compared to baseline. Considering the statistical power and 20% of drop-out rate, the target number of study subjects was determined as 60,000 worldwide; however, no sample size calculation specific to the South Korea region was performed.
- Statistical procedures
- All endpoints were summarized descriptively at each visit by treatment regimen and in total using observed data. Continuous variables were summarized using descriptive statistics (n, mean, standard deviation [SD]). Discrete variables were summarized using frequency tables (n, %). All statistical analyses were conducted using two-sided alternatives and a 5% significance level, unless otherwise stated. The primary safety end-points (SADRs and major hypoglycemic events reported as SADRs) and secondary endpoints of ADRs were summarized as the number of events and the number and percentage of patients with adverse events. The change from baseline in secondary effectiveness endpoints, including HbA1c, FPG, PPG, lipid profiles, and QoL, were summarized with descriptive statistical method and analysed using paired t-test. The summary of the baseline characteristics and safety data were based on full analysis set (FAS), which consisted of all patients with a baseline visit and who used any study insulin at least once. The analysis of the efficacy endpoints were repeated on efficacy analysis set (EAS), which consisted of all patients who made the final visit with at least one measurement of FPG, PPG, most recent HbA1c, weight or hypoglycemic events (yes, no) at baseline and at final visit. Only patients who maintained the same study insulin during the study, with or without addition of other insulin, were included in EAS.
METHODS
- Patient baseline characteristics and diabetes therapy during study period
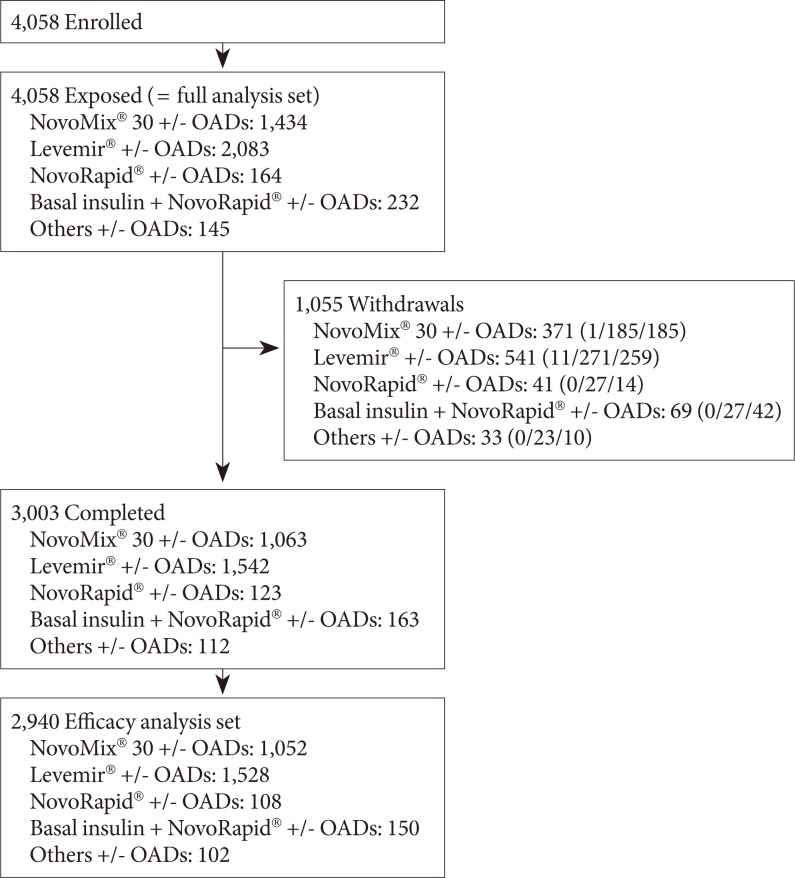
- Fig. 1 shows the participant disposition during the study period. A total of 4,058 patients were initially enrolled and were exposed to study insulins. A thousand and fifty-five patients ultimately withdrew from the study, and 3,003 completed the study, who constituted FAS. Among them, 2,940 patients (72.4% of FAS) were included as EAS.
- An overview of the demographics and baseline characteristics by treatment group for FAS is shown in Table 1. Patients were 57.1±13.0 years old, the body mass index (BMI) was 24.2±3.6 kg/m2, and the duration of diabetes was 10.1±7.8 years. The physicians' reasons for starting new therapy was to improve glycemic control (n=3,861, 95.1%), followed by trying new insulin (n=516, 12.7%), and reducing risk of hypoglycemia (n=462, 11.4%). Overall, the most common antidiabetic therapy prior to enrollment in the study was oral antidiabetic drugs (OADs) only (1,824 patients, 44.9%), followed by a combination of OADs and insulin therapy (1,229 patients, 30.3%), and no treatment (493 patients, 12.1%). The majority of enrolled patients received insulin detemir at baseline (2,083 patients, 51.3%).
- Safety outcomes
- A total of three SADRs from three patients were reported during the study period (0.1%). All SADRs were hypoglycemia with mild (two events) and moderate (one event) severity, and all were recoverable. At baseline, 31 patients reported 48 major (0.16 events per patient-year) and 816 minor (2.62 events per patient-year) 4-week hypoglycemic episodes, including 607 diurnal (1.95 events per patient-year), and 257 nocturnal (0.83 events per patient-year) episodes. During the total study period (24 weeks), there was no major hypoglycemic episode reported, and 267 patients reported 559 minor hypoglycemic episodes, including 451 diurnal and 108 nocturnal episodes. The overall rate of hypoglycemic episode was 2.77 events per patient-year at baseline, which decreased to 2.42 events per patient-year at week 24.
- In particular, the insulin-experienced patients who changed to the study insulin analogues upon the participation of the study showed significant decrease in the rate of hypoglycemic episode (from 4.68 events per patient-year to 2.68 events per patient-year). The change in the rate of hypoglycemic episode (events per patient-year) by the study visit is presented in Fig. 2. The mean body weight slightly increased from 63.7±11.5 kg (mean±SD) at baseline to 64.3±11.5 kg at week 24. The body weight of insulin-naïve patient increased by 0.8±2.9 kg after 24 weeks, whereas that of insulin-experienced patients increased by 0.4±3.1 kg.
- Efficacy outcomes
- The mean HbA1c decreased from 9.7% at baseline to 8.1% at week 24. In total, mean HbA1c was significantly reduced by 1.6%±2.2% after 24 weeks of treatment (P<0.001). The proportion of patients achieving the target of HbA1c <7.0% increased from 4.8% at baseline to 18.1% at week 12 and 22.7% at week 24. Mean HbA1c reduction was smallest in insulin aspart group (0.7%±2.3%; P=0.036 [P compared to baseline]), while it was greatest in the basal insulin+insulin aspart group (2.2%±2.5%; P<0.001 [P compared to baseline]). After 24 weeks of treatment, FPG and PPG was significantly reduced by 2.5±4.7 and 4.0±6.4 mmol/L, respectively (P<0.001). However, insulin aspart group showed less reductions in FPG and PPG from baseline (0.3±4.9, 1.3±5.0, respectively) compared to other groups. There was a significant reduction in low density lipoprotein cholesterol (LDL-C) by 0.3±1.1 mmol/L, in total cholesterol by 0.3±1.3 mmol/L, and in triglycerides by 0.2±1.2 mmol/L. Improvement (P<0.001) in the overall QoL score was observed from baseline (66.7±15.9) to the end of study (72.5±13.5, P<0.001). A subgroup analysis found insulin-naïve patients to show greater improvement in QoL than insulin-experienced patients (6.6±17.6 vs. 4.7±19.0). A summary of efficacy endpoints by time and treatment is depicted in Table 2.
RESULTS
- During the 24 weeks of treatment with the study products in 4,058 patients, modern insulin analogues (insulin detemir and insulin aspart alone or in combination) reduced the rate of hypoglycemic episodes over time compared to the previous conventional antidiabetic therapies. In regard to efficacy, modern insulin analogues were effective in reducing HbA1c, FPG, and PPG. They also improved the lipid profile as well as overall QoL regardless of prior insulin use.
- Insulin remains the most effective antihyperglycemic agent available for uncontrolled type 2 diabetes. Insulin initiation is indicated at FPG levels above 250 mg/dL, random glucose levels above 300 mg/dL, or the HbA1c above 10% [15]. Insulin should be also considered whenever HbA1c is above 8.5%, during treatment to achieve a more effective glycemic control. However, physicians, as well as their patients, are often resistant in starting insulin therapy due to the fear of hypoglycemia, weight gain, and perceived inconvenience and complexity of injection therapy.
- Hypoglycemia, a major barrier to achieving glycemic control in patients with type 2 diabetes, may lead to increased mortality due to proarrhythmic effect mediated by sympathoadrenal activation and hypokalemia [16]. In Action to Control Cardiovascular Risk in Type 2 Diabetes trial, the subjects who experienced a severe hypoglycemia event were found to have a higher mortality rate [17]. Recently, insulin analogues have been engineered to enhance their desired molecular properties: more rapid absorption or prolonged duration of action profiles and emulation of normal insulin physiology comprised of a stable basal secretion with surges of insulin closely temporarily related to food ingestion [18]. This manipulation enables modern insulin analogue to act more effectively with less hypoglycemic events. In a 26-week randomized, parallel, treat to target trial comparing insulin detemir with neutral protamine Hagedorn (NPH) insulin as add-on therapy to oral glucose lowering drugs in insulin-naïve population with type 2 diabetes, the risk of all hypoglycemia with insulin detemir was reduced by 47% (P<0.001) and nocturnal hypoglycemia by 55% (P<0.001) when compared with NPH insulin [10]. In a subgroup analysis from the 6 months of IMPROVETM study, which switched human premixed insulin to biphasic insulin aspart 30, a significant improvement in glycemic control combined with a reduced risk of hypoglycemia was reported [19]. Likewise, the present study showed that the change to the modern insulin analogues from conventional treatment brought a significant reduction in minor and nocturnal hypoglycemic events, and this phenomenon was much more remarkable in the previous insulin users.
- Another strong benefit of insulin analogues, especially levemir (basal insulin analogue), is less weight gain effect compared to human insulin or insulin glargine. Weight gain is an important barrier to initiating insulin therapy in clinical practice. In PREDICTIVE™ BMI clinical trial, use of once daily detemir for intensification of insulin therapy resulted in less weight gain compared to NPH (0.4 kg vs. 1.9 kg, P<0.0001) [13]. Raskin et al. [20] also reported a significantly reduced weight gain in insulin detemir-treated patients compared with the insulin glargine group (1.2±3.96 kg vs. 2.7±3.94 kg, P=0.001). The exact reason for the weight advantage of detemir is not fully understood. The proposed mechanisms of weight sparing effect of detemir may be explained by stronger central nervous anorexigenic efficacy [21] and increased urinary sodium excretion, thus reducing extracellular volume when compared with other kinds of insulin [22]. In the present study, the mean body weight slightly increased by only 0.6 kg during the study period, which is clinically insignificant, considering the benefits from the improvement in glycemic control after the switching to modern insulin analogue.
- People with diabetes have a worse QoL than people without other chronic illness due to daily management demands and diabetes related complications [23]. However, achieving better glycemic control is associated with better QoL: one study reported that patients whose HbA1c decreased by 1% or more within 1 year tended to have favorable mood and general well-being scores at follow-up [24]. The overall QoL score of the present study participants was significantly improved after initiating modern insulin analogue. Interestingly, there was much greater increase in the satisfaction score among insulin-naïve patients. This improvement may have been caused by reducing symptoms of high blood sugar and enhanced self-confidence to control their health status by themselves.
- Furthermore, there was a significant decrease in LDL-C and triglyceride, as well as an increase in high density lipoprotein cholesterol level, which is similar to the previous published A1chieve® study [25]. This result suggests the possibility that the studied modern insulin analogue may contribute to the prevention of cardiovascular complication when compared with conventional treatment modalities.
- This study has an inherent limitation of noninterventional study design. Observational study is nonrandomized and lacks a standardized treatment protocol and a control arm. Furthermore, most safety and efficacy parameters are based on the participants' recall and self-reported information, which may contain bias. Nevertheless, observational studies provide important information about how pharmaceutical therapies perform in real clinical practice because they have less stringent inclusion and exclusion criteria and can address larger numbers of people in more diverse environments [26].
- In conclusion, initiating or switching into study insulin analogues may provide a better chance of improving glycemic control with less side effects. During the study period, the subjects' blood glucose level improved greatly with low incidence of SADRs, including no incidence of major hypoglycemic episodes and a decrease in minor and nocturnal hypoglycemia. Moreover, the study participants showed the improvement in their QoL scores with a negligible weight gain.
DISCUSSION
-
Acknowledgements
- This study was sponsored by Novo Nordisk.
ACKNOWLEDGMENTS
- 1. Gaster B, Hirsch IB. The effects of improved glycemic control on complications in type 2 diabetes. Arch Intern Med 1998;158:134-140. ArticlePubMed
- 2. Stratton IM, Adler AI, Neil HA, Matthews DR, Manley SE, Cull CA, Hadden D, Turner RC, Holman RR. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. BMJ 2000;321:405-412. ArticlePubMedPMC
- 3. Saaddine JB, Cadwell B, Gregg EW, Engelgau MM, Vinicor F, Imperatore G, Narayan KM. Improvements in diabetes processes of care and intermediate outcomes: United States, 1988-2002. Ann Intern Med 2006;144:465-474. ArticlePubMed
- 4. Saydah SH, Fradkin J, Cowie CC. Poor control of risk factors for vascular disease among adults with previously diagnosed diabetes. JAMA 2004;291:335-342. ArticlePubMed
- 5. Riddle MC. Timely initiation of basal insulin. Am J Med 2004;116(Suppl 3A):3S-9S. Article
- 6. Wright A, Burden AC, Paisey RB, Cull CA, Holman RR; U.K. Prospective Diabetes Study Group. Sulfonylurea inadequacy: efficacy of addition of insulin over 6 years in patients with type 2 diabetes in the U.K. Prospective Diabetes Study (UKPDS 57). Diabetes Care 2002;25:330-336. PubMed
- 7. Korytkowski M. When oral agents fail: practical barriers to starting insulin. Int J Obes Relat Metab Disord 2002;26(Suppl 3):S18-S24. ArticlePDF
- 8. McCrimmon RJ, Frier BM. Hypoglycaemia, the most feared complication of insulin therapy. Diabete Metab 1994;20:503-512. PubMed
- 9. Peyrot M, Rubin RR, Lauritzen T, Skovlund SE, Snoek FJ, Matthews DR, Landgraf R, Kleinebreil L. International DAWN Advisory Panel. Resistance to insulin therapy among patients and providers: results of the cross-national Diabetes Attitudes, Wishes, and Needs (DAWN) study. Diabetes Care 2005;28:2673-2679. ArticlePubMedPDF
- 10. Hermansen K, Davies M, Derezinski T, Martinez Ravn G, Clauson P, Home P. A 26-week, randomized, parallel, treat-to-target trial comparing insulin detemir with NPH insulin as add-on therapy to oral glucose-lowering drugs in insulin-naive people with type 2 diabetes. Diabetes Care 2006;29:1269-1274. ArticlePubMedPDF
- 11. Philis-Tsimikas A, Charpentier G, Clauson P, Ravn GM, Roberts VL, Thorsteinsson B. Comparison of once-daily insulin detemir with NPH insulin added to a regimen of oral antidiabetic drugs in poorly controlled type 2 diabetes. Clin Ther 2006;28:1569-1581. ArticlePubMed
- 12. Dornhorst A, Luddeke HJ, Koenen C, Merilainen M, King A, Robinson A, Sreenan S. PREDICTIVE Study Group. Transferring to insulin detemir from NPH insulin or insulin glargine in type 2 diabetes patients on basal-only therapy with oral antidiabetic drugs improves glycaemic control and reduces weight gain and risk of hypoglycaemia: 14-week follow-up data from PREDICTIVE. Diabetes Obes Metab 2008;10:75-81. ArticlePubMed
- 13. Fajardo Montanana C, Hernandez Herrero C, Rivas Fernandez M. Less weight gain and hypoglycaemia with once-daily insulin detemir than NPH insulin in intensification of insulin therapy in overweight type 2 diabetes patients: the PREDICTIVE BMI clinical trial. Diabet Med 2008;25:916-923. PubMed
- 14. Sharma SK, Al-Mustafa M, Oh SJ, Azar ST, Shestakova M, Guler S, Vaz JA. Biphasic insulin aspart 30 treatment in patients with type 2 diabetes poorly controlled on prior diabetes treatment: results from the PRESENT study. Curr Med Res Opin 2008;24:645-652. ArticlePubMed
- 15. Nathan DM, Buse JB, Davidson MB, Ferrannini E, Holman RR, Sherwin R, Zinman B. American Diabetes Association. European Association for Study of Diabetes. Medical management of hyperglycemia in type 2 diabetes: a consensus algorithm for the initiation and adjustment of therapy: a consensus statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care 2009;32:193-203. ArticlePubMedPMCPDF
- 16. Donner T, Munoz M. Update on insulin therapy for type 2 diabetes. J Clin Endocrinol Metab 2012;97:1405-1413. ArticlePubMedPMC
- 17. Bonds DE, Miller ME, Bergenstal RM, Buse JB, Byington RP, Cutler JA, Dudl RJ, Ismail-Beigi F, Kimel AR, Hoogwerf B, Horowitz KR, Savage PJ, Seaquist ER, Simmons DL, Sivitz WI, Speril-Hillen JM, Sweeney ME. The association between symptomatic, severe hypoglycaemia and mortality in type 2 diabetes: retrospective epidemiological analysis of the ACCORD study. BMJ 2010;340:b4909ArticlePubMedPMC
- 18. Evans M, Schumm-Draeger PM, Vora J, King AB. A review of modern insulin analogue pharmacokinetic and pharmacodynamic profiles in type 2 diabetes: improvements and limitations. Diabetes Obes Metab 2011;13:677-684. ArticlePubMedPMCPDF
- 19. Shah S, Benroubi M, Borzi V, Gumprecht J, Kawamori R, Shaban J, Shestakova M, Wenying Y, Valensi P. IMPROVE Study Group Expert Panel. Safety and effectiveness of biphasic insulin aspart 30/70 (NovoMix 30) when switching from human premix insulin in patients with type 2 diabetes: subgroup analysis from the 6-month IMPROVE observational study. Int J Clin Pract 2009;63:574-582. ArticlePubMedPMC
- 20. Raskin P, Gylvin T, Weng W, Chaykin L. Comparison of insulin detemir and insulin glargine using a basal-bolus regimen in a randomized, controlled clinical study in patients with type 2 diabetes. Diabetes Metab Res Rev 2009;25:542-548. ArticlePubMed
- 21. Hallschmid M, Jauch-Chara K, Korn O, Molle M, Rasch B, Born J, Schultes B, Kern W. Euglycemic infusion of insulin detemir compared with human insulin appears to increase direct current brain potential response and reduces food intake while inducing similar systemic effects. Diabetes 2010;59:1101-1107. ArticlePubMedPMCPDF
- 22. Hendriksen KV, Jensen T, Oturai P, Feldt-Rasmussen B. Effects of insulin detemir and NPH insulin on renal handling of sodium, fluid retention and weight in type 2 diabetic patients. Diabetologia 2012;55:46-50. ArticlePubMedPDF
- 23. Rubin RR, Peyrot M. Quality of life and diabetes. Diabetes Metab Res Rev 1999;15:205-218. ArticlePubMed
- 24. van der Does FE, de Neeling JN, Snoek FJ, Grootenhuis PA, Kostense PJ, Bouter LM, Heine RJ. Randomized study of two different target levels of glycemic control within the acceptable range in type 2 diabetes. Effects on well-being at 1 year. Diabetes Care 1998;21:2085-2093. ArticlePubMedPDF
- 25. Home P, Naggar NE, Khamseh M, Gonzalez-Galvez G, Shen C, Chakkarwar P, Wenying Y. An observational non-interventional study of people with diabetes beginning or changed to insulin analogue therapy in non-Western countries: the A1chieve study. Diabetes Res Clin Pract 2011;94:352-363. ArticlePubMed
- 26. Yang W, Zilov A, Soewondo P, Bech OM, Sekkal F, Home PD. Observational studies: going beyond the boundaries of randomized controlled trials. Diabetes Res Clin Pract 2010;88(Suppl 1):S3-S9. ArticlePubMed
REFERENCES
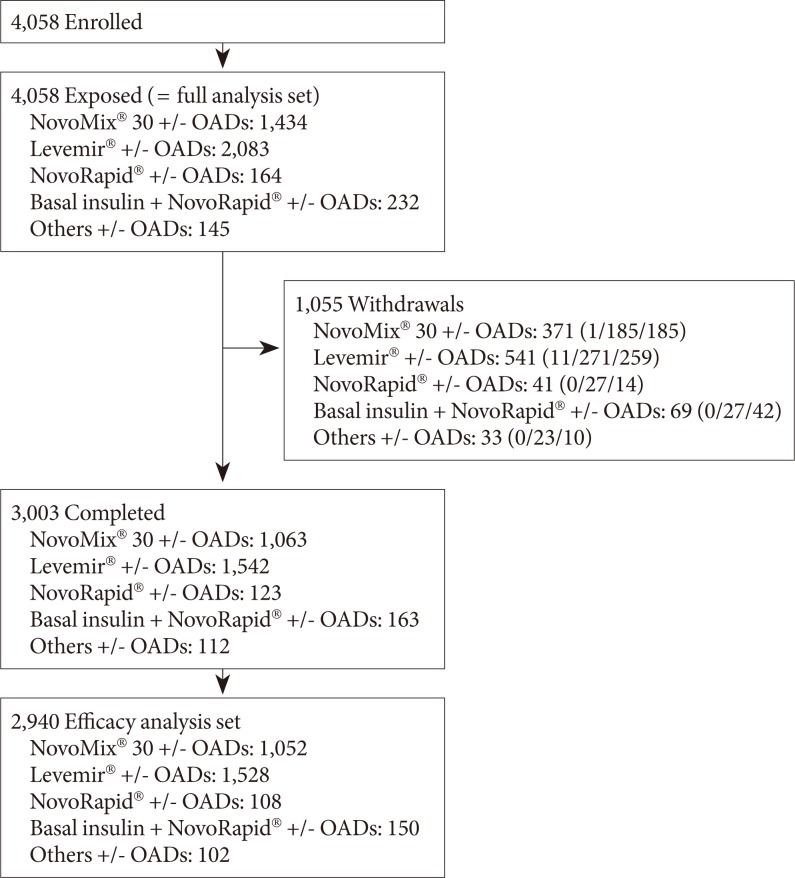
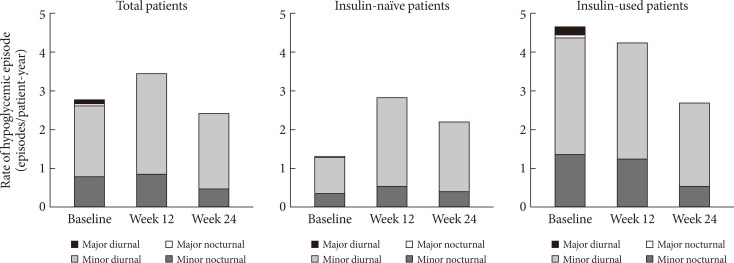
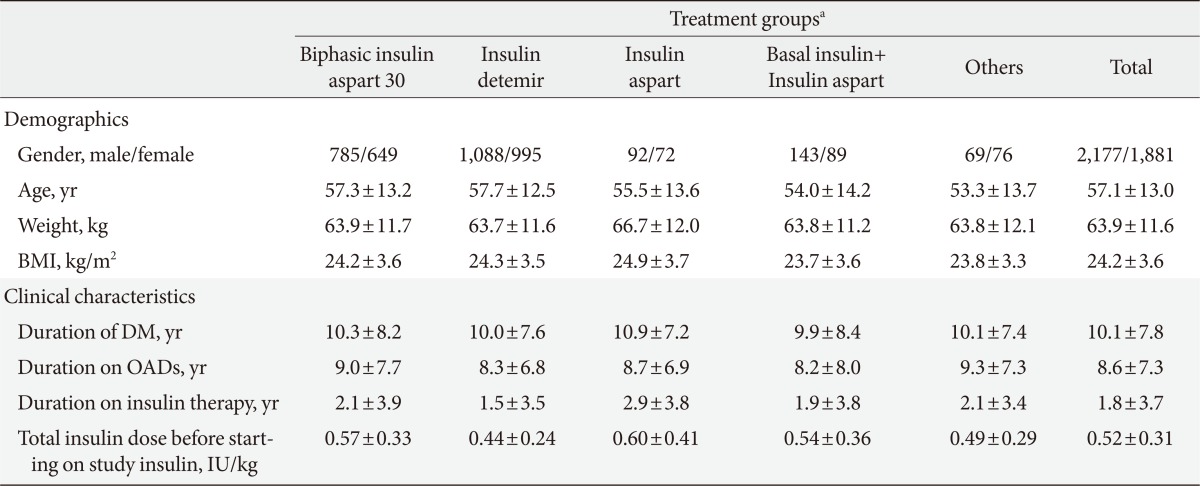
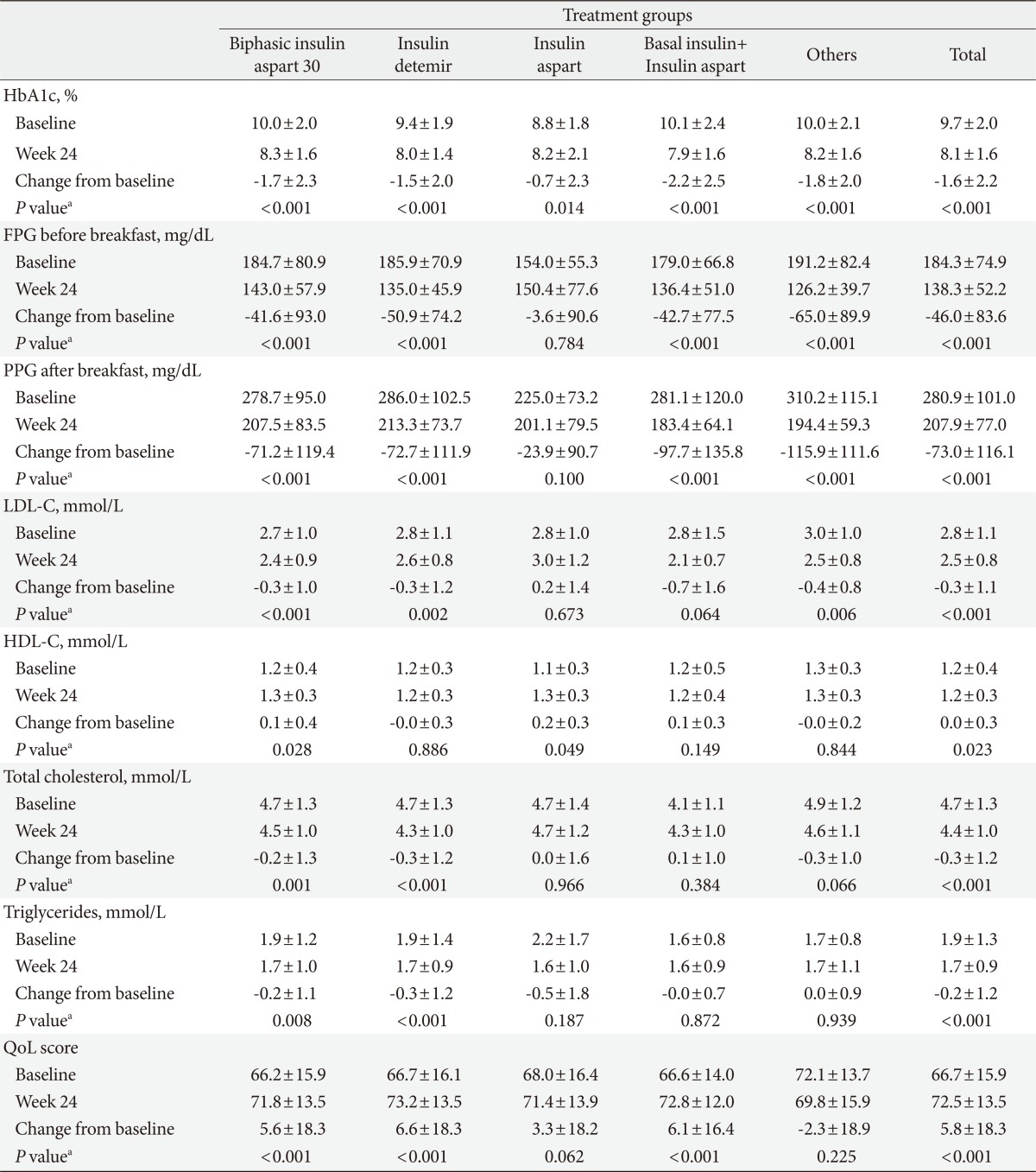
Figure & Data
References
Citations
- Insulin therapy for adult patients with type 2 diabetes mellitus: a position statement of the Korean Diabetes Association, 2017
Byung-Wan Lee, Jin Hwa Kim, Seung-Hyun Ko, Kyu Yeon Hur, Nan-Hee Kim, Sang Youl Rhee, Hyun Jin Kim, Min Kyong Moon, Seok-O Park, Kyung Mook Choi
The Korean Journal of Internal Medicine.2017; 32(6): 967. CrossRef - Insulin Therapy for Adult Patients with Type 2 Diabetes Mellitus: A Position Statement of the Korean Diabetes Association, 2017
Byung-Wan Lee, Jin Hwa Kim, Seung-Hyun Ko, Kyu-Yeon Hur, Nan-Hee Kim, Sang Youl Rhee, Hyun Jin Kim, Min Kyong Moon, Seok-O Park, Kyung Mook Choi
Diabetes & Metabolism Journal.2017; 41(5): 367. CrossRef - An information and communication technology-based centralized clinical trial to determine the efficacy and safety of insulin dose adjustment education based on a smartphone personal health record application: a randomized controlled trial
Gyuri Kim, Ji Cheol Bae, Byoung Kee Yi, Kyu Yeon Hur, Dong Kyung Chang, Moon-Kyu Lee, Jae Hyeon Kim, Sang-Man Jin
BMC Medical Informatics and Decision Making.2017;[Epub] CrossRef - Characteristics Predictive for a Successful Switch from Insulin Analogue Therapy to Oral Hypoglycemic Agents in Patients with Type 2 Diabetes
Gyuri Kim, Yong-ho Lee, Eun Seok Kang, Bong-Soo Cha, Hyun Chul Lee, Byung-Wan Lee
Yonsei Medical Journal.2016; 57(6): 1395. CrossRef - Avoiding or coping with severe hypoglycemia in patients with type 2 diabetes
Jae-Seung Yun, Seung-Hyun Ko
The Korean Journal of Internal Medicine.2015; 30(1): 6. CrossRef - Clinical Characteristics of Patients Responding to Once-Daily Basal Insulin Therapy in Korean Subjects with Type 2 Diabetes
Sun Ok Song, You-Cheol Hwang, Kyu-Jeung Ahn, Bong Soo Cha, Young Duk Song, Dae Wook Lee, Byung-Wan Lee
Diabetes Therapy.2015; 6(4): 547. CrossRef - The optimal morning:evening ratio in total dose of twice‐daily biphasic insulin analogue in poorly controlled Type 2 diabetes: a 24‐week multi‐centre prospective, randomized controlled, open‐labelled clinical study
C. H. Jung, J.‐Y. Park, J. H. Cho, K.‐H. Yoon, H. K. Yang, Y.‐H. Lee, B. S. Cha, B.‐W. Lee
Diabetic Medicine.2014; 31(1): 68. CrossRef -
The glycemic efficacies of insulin analogue regimens according to baseline glycemic status in Korean patients with type 2 diabetes: sub‐analysis from the A
1
chieve
®
study
Y.‐C. Hwang, J. G. Kang, K. J. Ahn, B. S. Cha, S.‐H. Ihm, S. Lee, M. Kim, B.‐W. Lee
International Journal of Clinical Practice.2014; 68(11): 1338. CrossRef - Letter: Efficacy and Safety of Biphasic Insulin Aspart 30/70 in Type 2 Diabetes Suboptimally Controlled on Oral Antidiabetic Therapy in Korea: A Multicenter, Open-Label, Single-Arm Study (Diabetes Metab J2013;37:117-24)
Byung-Wan Lee
Diabetes & Metabolism Journal.2013; 37(3): 212. CrossRef
 PubReader
PubReader Cite
Cite